*NURSING > Solutions Guide > NURSING 2535 Med Surg 3 - Endocrine Disorders (complete updated study guide) Spring 2021 (All)
NURSING 2535 Med Surg 3 - Endocrine Disorders (complete updated study guide) Spring 2021
Document Content and Description Below
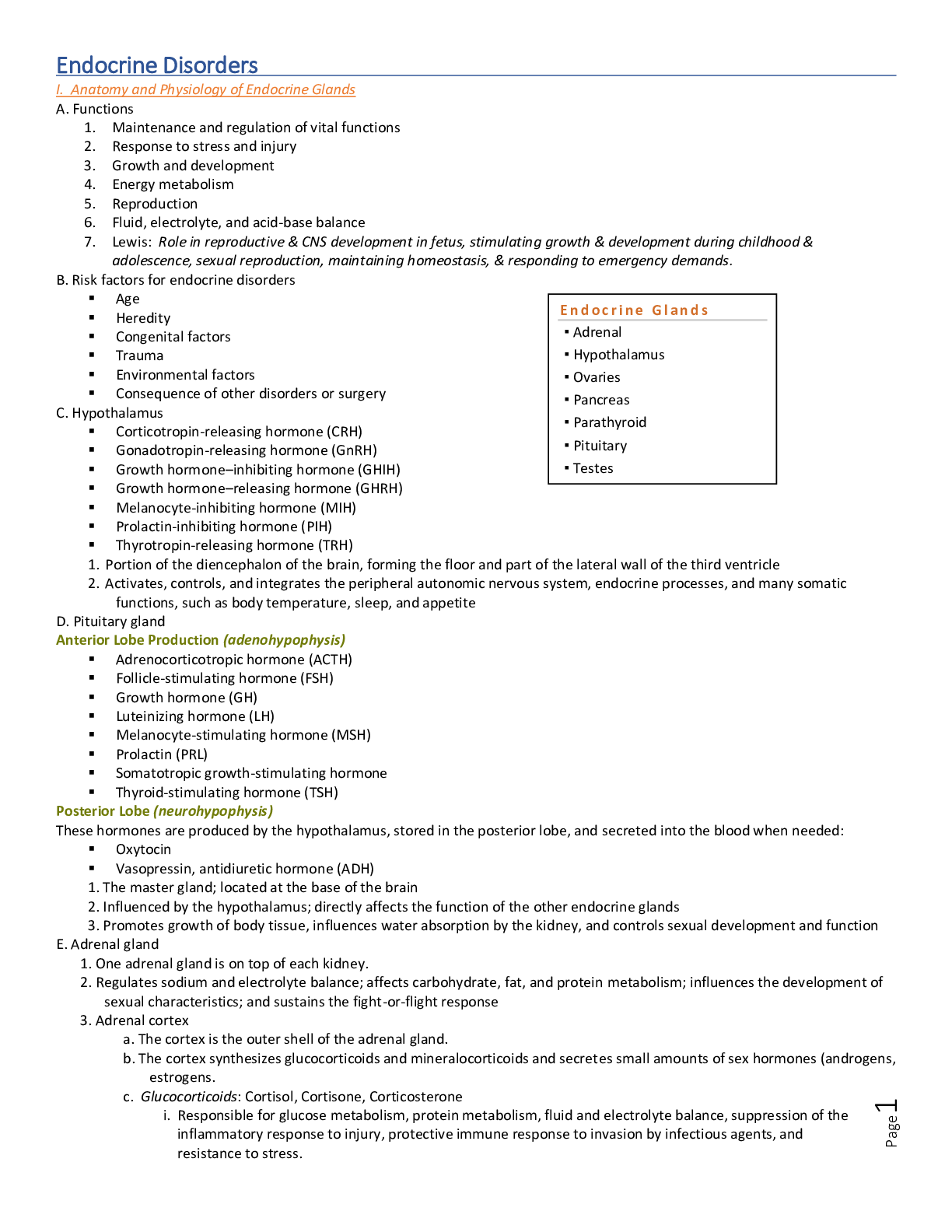
Endocrine Disorders I. Anatomy and Physiology of Endocrine Glands A. Functions 1. Maintenance and regulation of vital functions 2. Response to stress and injury 3. Growth and develop... ment 4. Energy metabolism 5. Reproduction 6. Fluid, electrolyte, and acid-base balance 7. Lewis: Role in reproductive & CNS development in fetus, stimulating growth & development during childhood & adolescence, sexual reproduction, maintaining homeostasis, & responding to emergency demands. B. Risk factors for endocrine disorders Age Heredity Congenital factors Trauma Environmental factors Consequence of other disorders or surgery C. Hypothalamus Corticotropin-releasing hormone (CRH) Gonadotropin-releasing hormone (GnRH) Growth hormone–inhibiting hormone (GHIH) Growth hormone–releasing hormone (GHRH) Melanocyte-inhibiting hormone (MIH) Prolactin-inhibiting hormone (PIH) Thyrotropin-releasing hormone (TRH) 1. Portion of the diencephalon of the brain, forming the floor and part of the lateral wall of the third ventricle 2. Activates, controls, and integrates the peripheral autonomic nervous system, endocrine processes, and many somatic functions, such as body temperature, sleep, and appetite D. Pituitary gland Anterior Lobe Production (adenohypophysis) Adrenocorticotropic hormone (ACTH) Follicle-stimulating hormone (FSH) Growth hormone (GH) Luteinizing hormone (LH) Melanocyte-stimulating hormone (MSH) Prolactin (PRL) Somatotropic growth-stimulating hormone Thyroid-stimulating hormone (TSH) Posterior Lobe (neurohypophysis) These hormones are produced by the hypothalamus, stored in the posterior lobe, and secreted into the blood when needed: Oxytocin Vasopressin, antidiuretic hormone (ADH) 1. The master gland; located at the base of the brain 2. Influenced by the hypothalamus; directly affects the function of the other endocrine glands 3. Promotes growth of body tissue, influences water absorption by the kidney, and controls sexual development and function E. Adrenal gland 1. One adrenal gland is on top of each kidney. 2. Regulates sodium and electrolyte balance; affects carbohydrate, fat, and protein metabolism; influences the development of sexual characteristics; and sustains the fight-or-flight response 3. Adrenal cortex a. The cortex is the outer shell of the adrenal gland. b. The cortex synthesizes glucocorticoids and mineralocorticoids and secretes small amounts of sex hormones (androgens, estrogens. c. Glucocorticoids: Cortisol, Cortisone, Corticosterone i. Responsible for glucose metabolism, protein metabolism, fluid and electrolyte balance, suppression of the inflammatory response to injury, protective immune response to invasion by infectious agents, and resistance to stress. d. Mineralocorticoids: Aldosterone i. Regulation of electrolyte balance by promoting sodium retention and potassium excretion. 4. Adrenal medulla a. The medulla is the inner core of the adrenal gland. b. The medulla works as part of the sympathetic nervous system and produces epinephrine and norepinephrine. F. Thyroid gland 1. Located in the anterior part of the neck 2. Controls the rate of body metabolism and growth and produces thyroxine (T4), triiodothyronine (T3), and thyrocalcitonin G. Parathyroid glands 1. Located on the thyroid gland 2. Controls calcium and phosphorus metabolism; produces parathyroid hormone H. Pancreas 1. Located posteriorly to the stomach 2. Influences carbohydrate metabolism, indirectly influences fat and protein metabolism, and produces insulin and glucagon I. Ovaries and testes 1. The ovaries are located in the pelvic cavity and produce estrogen and progesterone. 2. The testes are located in the scrotum, control the development of the secondary sex characteristics, & produce testosterone. J. Negative-feedback loop 1. Regulates hormone secretion by the hypothalamus and pituitary gland 2. Increased amounts of target gland hormones in the bloodstream decrease secretion of the same hormone and other hormones that stimulate its release. II. Diagnostic Tests A. Stimulation and suppression tests 1. Stimulation tests a. In the client with suspected underactivity of an endocrine gland, a stimulus may be provided to determine whether the gland is capable of normal hormone production. b. Measured amounts of selected hormones or substances are administered to stimulate the target gland to produce its hormone. c. Hormone levels produced by the target gland are measured. d. Failure of the hormone level to increase with stimulation indicates hypofunction. 2. Suppression tests a. Suppression tests are used when hormone levels are high or in the upper range of normal. b. Agents that normally induce a suppressed response are administered to determine whether normal negative feedback is intact. c. Failure of hormone production to be suppressed during standardized testing indicates hyperfunction. 3. Overnight dexamethasone suppression test a. Used to distinguish between Cushing’s syndrome and Cushing’s disease. b. In Cushing’s disease the source of excess cortisol is the pituitary gland rather than the adrenal cortex or exogenous corticosteroid administration. c. Dexamethasone, a potent long-acting corticosteroid given at bedtime, should suppress the morning cortisol in clients without Cushing’s disease by suppressing adrenocorticotropic hormone (ACTH) production; in the client with Cushing’s disease, this suppression will not occur. B. Radioactive iodine uptake 1. This thyroid function test measures the absorption of an iodine isotope to determine how the thyroid gland is functioning. 2. A small dose of radioactive iodine is given by mouth or intravenously; the amount of radioactivity is measured in 2 to 4 hours and again at 24 hours. 3. Normal values are 3% to 10% at 2 to 4 hours, and 5% to 30% in 24 hours. 4. Elevated values indicate hyperthyroidism, decreased iodine intake, or increased iodine excretion. 5. Decreased values indicate a low T4 level, the use of antithyroid medications, thyroiditis, myxedema, or hypothyroidism. 6. The test is contraindicated in pregnancy. C. T3 and T4 resin uptake test 1. Blood tests are used to diagnose thyroid disorders. 2. T3 and T4 regulate thyroid-stimulating hormone. 3. Normal values (normal findings vary between laboratory settings) a. Triiodothyronine, total T3: 70–205 ng/dL (1.2–3.4 nmol/L) b. Thyroxine, total T4: 5–12 mcg/dL (64–154 nmol/L) c. Thyroxine, free (FT4): 0.8–2.8 ng/dL (10–36 pmol/L) 4. The T4 level is elevated in hyperthyroidism and decreased in hypothyroidism. D. Thyroid-stimulating hormone 1. Blood test is used to differentiate the diagnosis of primary hypothyroidism. 2. Normal value is 2–10 mcU/L (2–10 mU/L). 3. Elevated values indicate primary hypothyroidism. 4. Decreased values indicate hyperthyroidism or secondary hypothyroidism. E. Thyroid scan 1. A thyroid scan is performed to identify nodules or growths in the thyroid gland. 2. A radioisotope of iodine or technetium is administered before scanning the thyroid gland. 3. Reassure the client that the level of radioactive medication is not dangerous to self or others. 4. Determine whether the client has received radiographic contrast agents within the past 3 months, because these may invalidate the scan. 5. Check with the health care provider (HCP) regarding discontinuing medications containing iodine for 14 days before the test and the need to discontinue thyroid medication before the test. 6. Instruct the client to maintain NPO (nothing by mouth) status after midnight on the day before the test; if iodine is used, the client will fast for an additional 45 minutes after ingestion of the oral isotope and the scan will be performed in 24 hours. 7. If technetium is used, it is administered by the intravenous (IV) route 30 minutes before the scan. 8. The test is contraindicated in pregnancy. F. Needle aspiration of thyroid tissue 1. Aspiration of thyroid tissue is done for cytological examination. 2. No client preparation is necessary; NPO status may or may not be prescribed. 3. Light pressure is applied to the aspiration site after the procedure. G. Glycosylated hemoglobin 1. HgbA1C is blood glucose bound to hemoglobin. 2. Hemoglobin A1c (glycosylated hemoglobin A; HbA1c) is a reflection of how well blood glucose levels have been controlled for the past 3 to 4 months. 3. Hyperglycemia in clients with diabetes is usually a cause of an increase in HbA1c. 4. Fasting is not required before the test. 5. Normal reference intervals: 4.0%–6.0% (4.0%–6.0%) 6. HgbA1C and estimated average glucose (eAG) reference intervals. Poor glycemic control in a client with diabetes mellitus is usually the cause of an increase in the HbA1c value. H. 24-hour urine collection for vanillylmandelic acid (VMA) 1. Diagnostic tests for pheochromocytoma include a 24-hour urine collection for VMA, a product of catecholamine metabolism, metanephrine, and catecholamines, all of which are elevated in the presence of pheochromocytoma. 2. The normal range of urinary catecholamines: a. Epinephrine: < 20 mcg/day (< 109 nmol/day) b. Norepinephrine: 15–80 mcg/day (89–473 nmol/day) III. Pituitary Gland Disorders Anterior Pituitary 80% of the gland itself Regulated by hypothalamus Secretes: Thyroid Stimulating Hormone; Adrenocorticotropic Hormone; Gonadotropic hormones: Follicle-stimulating hormone, Luteinizing hormone; and prolactin. Anterior Pituitary Disorders Clinical Manifestations Headaches Visual changes Loss of smell, nausea and vomiting Seizures Target glands-hormone deficiency o GH o FSH/LH o TSH o ACTH Diagnostic Studies for Pituitary Disorders (Lewis: pg. 1113-1114) History Physical Examination* MRI/CT Laboratory Tests Child, parental, and familial growth patterns Skeletal survey in children younger than 3 years of age o Hand–wrist x-ray to examine for centers of ossification Growth Hormone Excess: Acromegaly Excessive growth hormone production Results in overgrowth of bone ends and soft tissue Usually caused by a tumor Manifestations o Large hands and feet o Enlarged tongue o Deep voice o Visual disturbances o Increased facial hair o Malocclusion of the teeth o Glucose intolerance o Increased colon cancer risk o Cardiovascular complications Atherosclerosis Cardiomegaly Pituitary Hyperfunction GH excess: Gigantism Rare Begins in childhood before epiphyses closure Stature increases, but little bony deformity occurs. Soft-tissue swelling occurs, and the peripheral nerves are enlarged. Excess GH before closure of epiphyseal shafts results in overgrowth of the long bones Reach heights of 8 feet or more Delay in fontanel closure due to enlargement of the head circumference Vertical growth with rapid and increased muscle development Weight is generally in proportion to height Hyperpituitarism Prolactinomas o Most common type of pituitary adenoma Clinical manifestations • Sexual dysfunction • Menstrual dysfunction • Headaches • Visual disturbances • Galactorrhea Treatment • Drug therapy-Bromocriptine or cabergoline • Possible surgery and radiation Nursing and Interprofessional Management of GH Excess Prognosis depends upon age at onset, age when treatment started, and tumor size. Surgical treatment to remove the tumor Irradiation and radioactive implants to reduce the size of the tumor. Drug therapy Somatostatin Analogs, Dopamine Agonists, Gh antagonists Hormone replacement therapy after surgery in some cases Emotional Support Hypopituitarism: Growth Hormone (GH) Deficiency Inhibits somatic growth in all cells of the body. Primary site of dysfunction appears to be in the hypothalamus. Usually caused by a pituitary tumor in the adult and deficiency of pituitary hormones in the child. Symptoms and signs relate to the underlying disorder and to the specific pituitary hormones that are deficient or absent. Deficiencies of TSH and ACTH are life threatening and can lead to end organ failure. Treatment includes surgery or radiation and lifelong hormone replacement—thyroid, cortisol, testosterone, estrogen, progesterone, somatropin. Treatment for Pituitary Adenomas Surgery to remove tumor: Transsphenoidal hypophysectomy. Radiation Appropriate hormone therapy or drugs to reduce GH levels Post-Hypophysectomy Nursing care Elevate HOB 30 degrees. Pt should avoid coughing, sneezing, Valsalva maneuver. Be alert for CSF drainage: o Send clear nasal drainage to lab for glucose testing o Assess for persistent headaches Perform oral care but NO tooth brushing for ten days! Observe for any signs of bleeding. Post-Operative Teaching Lifelong hormone replacement is necessary if pituitary gland is damaged or removed. Teach about purpose and effects of each medication. Provide information regarding decreased fertility. Encourage colorectal screening. Posterior Pituitary Disorders Syndrome of Inappropriate Antidiuretic Hormone Pituitary stores and releases Antidiuretic Hormone (ADH) ADH causes reabsorption of water into the circulating volume SIADH occurs when there is too much ADH: o Body retains too much fluid (ECF expansion) o Leads to dilutional hyponatremia and decreased serum osmolality o GFR increases Causes of SIADH Medications Malignant tumors: o Small cell lung cancer o Pancreatic cancer o Lymphomas CNS Disorders: o Head trauma o Stroke o Brain tumors o Infection-Encephalitis Pulmonary Disorders: o Lung abscess o TB o Pneumonia Medications that stimulate ADH release Carbamazepine Chlorpropamide Opioids Oxytocin Thiazide diuretics Antidepressants: o SSRIs o TCAs Antineoplastic agents Clinical Manifestations of SIADH Muscle cramping, pain, & weakness Thirst Nausea and vomiting Fatigue Low urinary output Increased body weight Cerebral edema Seizures, coma, death Diagnostic Studies Lab assessment: o Serum sodium-decreased: Less than 134meq/L o Serum osmolality-decreased: Less than 290Mosm//kg o Urine Specific Gravity-increased: Greater than 1.025 o Urine sodium level-increased Nursing care for SIADH Goals are to treat the underlying condition and prevent further decline of the serum Na level. o Fluid restriction (<1L/day) o HOB flat o Seizure precautions o Frequent oral hygiene o Avoid meds that stimulate ADH release o Patient teaching: s/s of electrolyte imbalance related to diuretics. Medications and Treatment of SIADH Serum sodium level greater than 125meq/L o Fluid restriction only Loop diuretics-Serum Sodium 125meq/L o Demeclocycline o IV Hypertonic saline solution Serum sodium level below 120meq/L o GIVE SLOWLY Vasopressor receptor antagonists o Conivaptan and Tolvaptan Diabetes Insipidus Decreased ADH Leads to increased urinary output and increased plasma osmolality May be transient or lifelong 3 Types of Diabetes Insipidus Central: Problem with ADH synthesis or release. o (Most common) Nephrogenic: Inadequate renal response to ADH. o (From meds or renal damage) Primary: Caused by excessive water intake. COntinued.......................... [Show More]
Last updated: 1 year ago
Preview 1 out of 24 pages
Reviews( 0 )
Recommended For You
Managerial Economics> Solutions Guide > Managerial Economics in a Global Economy 8th Edition By Dominick Salvatore (Solutions Manual ) (All)
Managerial Economics in a Global Economy 8th Edition By Dominick Salvatore (Solutions Manual )
Reflecting the highly globalized nature of tastes, production, labor markets, and financial markets in today's world, Managerial Economics in a Global Economy, Eighth Edition, presents the theory of t...
By eBookSmTb , Uploaded: Jun 01, 2022
$20
Business Administration> Solutions Guide > Australasian Business Statistics 4th Edition By Black, Asafu ,Adjaye, Burke, Khan, King, Perera, Papadimos, Sherwood, Wasimi (Solution Manual All Chapters) (All)
Australasian Business Statistics 4th Edition By Black, Asafu ,Adjaye, Burke, Khan, King, Perera, Papadimos, Sherwood, Wasimi (Solution Manual All Chapters)
Data-driven decisions are driving the global knowledge economy. To get the edge, graduates need the power of statistical analysis to create business insight. This fourth edition of Australasian Busine...
By eBookSmTb , Uploaded: Nov 23, 2021
$20
Business Law> Solutions Guide > International Economics Theory and Policy 12th edition By Paul R. Krugman, Maurice Obstfeld, Marc Melitz (Solutions Manual ) (All)
International Economics Theory and Policy 12th edition By Paul R. Krugman, Maurice Obstfeld, Marc Melitz (Solutions Manual )
1. Introduction PART 1: INTERNATIONAL TRADE THEORY 2. Word Trade: An Overview 3. Labor Productivity and Comparative Advantage: The Ricardian Model 4. Specific Factors and Income Distribution 5....
By eBookSmTb , Uploaded: Nov 05, 2022
$25
Education> Solutions Guide > Essentials of Accounting for Governmental and Not-for-Profit Organizations, 14th Edition By Paul Copley (Solutions Manual ) (All)
.png)
Essentials of Accounting for Governmental and Not-for-Profit Organizations, 14th Edition By Paul Copley (Solutions Manual )
The focus of Copley's Essentials of Accounting for Governmental and Not-for-Profit Organizations, 14th edition is on the preparation of external financial statements which is a challenge for governmen...
By eBookSmTb , Uploaded: Oct 07, 2022
$20
Urban Policy and Planning> Solutions Guide > Dental list Yellow pages (All)
Dental list Yellow pages
HumanaDental PPO dental directory Location: 15 miles from 07304 May 16, 2018 Dentist Locations: 4638 Get the most out of your dental plan. the covered person must send us a letter requesting a...
By Academia1434 , Uploaded: Mar 30, 2021
$1
Statistics> Solutions Guide > MAT 240 Module Five Assignment Hypothesis Testing for Regional Real Estate Company (All)
MAT 240 Module Five Assignment Hypothesis Testing for Regional Real Estate Company
Scenario You have been hired by the Regional Real Estate Company to help them analyze real estate data. One of the company’s Pacific region salespeople just returned to the office with a newly desi...
By ACADEMICTUTORIAL , Uploaded: May 26, 2022
$4
Finance> Solutions Guide > Week 4 Mini Case Complete The Chapter 9 (All)
Week 4 Mini Case Complete The Chapter 9
During the last few years, Jana Industries has been too constrained by the high cost of capital to make many capital investments. Recently, though, capital costs have been declining, and the company h...
By ACADEMICTUTORIAL , Uploaded: May 26, 2022
$3.5
Accounting> Solutions Guide > ACCT370 Excel Project Part 3 (All)
ACCT370 Excel Project Part 3
EXCEL PROJECT: PROJECTING FINANCIAL STATEMENTS ASSIGNMENT INSTRUCTIONS OVERVIEW Common Sized Balance Sheets (Tabs 12), Common Sized Income Statements (Tab 13), Horizontal Analysis Balanc...
By ACADEMICTUTORIAL , Uploaded: Feb 14, 2023
$6.5
Business> Solutions Guide > Read the Chapter 19 Mini Case in Financial Management: Theory and Practice (All)
Read the Chapter 19 Mini Case in Financial Management: Theory and Practice
Chapter 18 leasing and financing Chapter 19 Mini Case in Financial Management Lewis Securities Inc Read the Chapter 19 Mini Case in Financial Management: Theory and Practice. Using complete sen...
By ACADEMICTUTORIAL , Uploaded: May 01, 2023
$5.5
Calculus> Solutions Guide > Applied Calculus, 6th Edition By Hughes-Hallett, Lock, Gleason (Solutions Manual) (All)
Applied Calculus, 6th Edition By Hughes-Hallett, Lock, Gleason (Solutions Manual)
A text for interactive Calculus courses, featuring innovative problems This sixth edition of Applied Calculus engages students with well-constructed problems and content to deepen understanding. The R...
By eBookSmTb , Uploaded: Dec 09, 2022
$25
Document information
Connected school, study & course
About the document
Uploaded On
Feb 22, 2021
Number of pages
24
Written in

Additional information
This document has been written for:
Uploaded
Feb 22, 2021
Downloads
0
Views
64