*NURSING > EXAM > NURSING 2501 Exam 1 Test Bank Chapter 7: End-of-Life Care Questions And Answers (All)
NURSING 2501 Exam 1 Test Bank Chapter 7: End-of-Life Care Questions And Answers
Document Content and Description Below
Exam 1 test bank Chapter 7: End-of-Life Care 1. A nurse cares for a dying client. Which manifestation of dying should the nurse treat first? a. Anorexia b. Pain c. Nausea d. Hair loss Only s... ymptoms that cause distress for a dying client should be treated. Such symptoms include pain, nausea and vomiting, dyspnea, and agitation. These problems interfere with the client’s comfort. Even when symptoms, such as anorexia or hair loss, disturb the family, they should be treated only if the client is distressed by their presence. The nurse should treat the client’s pain first. 2. A nurse plans care for a client who is nearing end of life. Which question should the nurse ask when developing this client’s plan of care? a. “Is your advance directive up to date and notarized?” b. “Do you want to be at home at the end of your life?” c. “Would you like a physical therapist to assist you with range-of-motion activities?” d. “Have your children discussed resuscitation with your health care provider?” When developing a plan of care for a dying client, consideration should be given for where the client wants to die. Advance directives do not need to be notarized. A physical therapist would not be involved in end-of-life care. The client should discuss resuscitation with the health care provider and children; do-not-resuscitate status should be the client’s decision, not the family’s decision. 3. A nurse is caring for a client who has lung cancer and is dying. Which prescription should the nurse question? a. Morphine 10 mg sublingual every 6 hours PRN for pain level greater than 5 b. Albuterol (Proventil) metered dose inhaler every 4 hours PRN for wheezes c. Atropine solution 1% sublingual every 4 hours PRN for excessive oral secretions d. Sodium biphosphate (Fleet) enema once a day PRN for impacted stool Pain medications should be scheduled around the clock to maintain comfort and prevent reoccurrence of pain. The other medications are appropriate for this client. 4. A client tells the nurse that, even though it has been 4 months since her sister’s death, she frequently finds herself crying uncontrollably. How should the nurse respond? a. “Most people move on within a few months. You should see a grief counselor.” b. “Whenever you start to cry, distract yourself from thoughts of your sister.” c. “You should try not to cry. I’m sure your sister is in a better place now.” d. “Your feelings are completely normal and may continue for a long time.” Frequent crying is not an abnormal response. The nurse should let the client know that this is normal and okay. Although the client may benefit from talking with a grief counselor, it is not unusual for her to still be grieving after a few months. The other responses are not as therapeutic because they justify or minimize the client’s response. 5. After teaching a client about advance directives, a nurse assesses the client’s understanding. Which statement indicates the client correctly understands the teaching? a. “An advance directive will keep my children from selling my home when I’m old.” b. “An advance directive will be completed as soon as I’m incapacitated and can’t think for myself.” c. “An advance directive will specify what I want done when I can no longer make decisions about health care.” d. “An advance directive will allow me to keep my money out of the reach of my family.” An advance directive is a written document prepared by a competent individual that specifies what, if any, extraordinary actions a person would want taken when he or she can no longer make decisions about personal health care. It does not address issues such as the client’s residence or financial matters. 6. A nurse teaches a client who is considering being admitted to hospice. Which statement should the nurse include in this client’s teaching? a. “Hospice admission has specific criteria. You may not be a viable candidate, so we will look at alternative plans for your discharge.” b. “Hospice care focuses on a holistic approach to health care. It is designed not to hasten death, but rather to relieve symptoms.” c. “Hospice care will not help with your symptoms of depression. I will refer you to the facility’s counseling services instead.” d. “You seem to be experiencing some difficulty with this stage of the grieving process. Let’s talk about your feelings.” As both a philosophy and a system of care, hospice care uses an interdisciplinary approach to assess and address the holistic needs of clients and families to facilitate quality of life and a peaceful death. This holistic approach neither hastens nor postpones death but provides relief of symptoms experienced by the dying client. 7. A nurse is caring for a dying client. The client’s spouse states, “I think he is choking to death.” How should the nurse respond? a. “Do not worry. The choking sound is normal during the dying process.” b. “I will administer more morphine to keep your husband comfortable.” c. “I can ask the respiratory therapist to suction secretions out through his nose.” d. “I will have another nurse assist me to turn your husband on his side.” The choking sound or “death rattle” is common in dying clients. The nurse should acknowledge the spouse’s concerns and provide interventions that will reduce the choking sounds. Repositioning the client onto one side with a towel under the mouth to collect secretions is the best intervention. The nurse should not minimize the spouse’s concerns. Morphine will assist with comfort but will not decrease the choking sounds. Nasotracheal suctioning is not appropriate in a dying client. 8. The nurse is teaching a family member about various types of complementary therapies that might be effective for relieving the dying client’s anxiety and restlessness. Which statement made by the family member indicates understanding of the nurse’s teaching? a. “Maybe we should just hire an around-the-clock sitter to stay with Grandmother.” b. “I have some of her favorite hymns on a CD that I could bring for music therapy.” c. “I don’t think that she’ll need pain medication along with her herbal treatments.” d. “I will burn therapeutic incense in the room so we can stop the anxiety pills.” Music therapy is a complementary therapy that may produce relaxation by quieting the mind and removing a client’s inner restlessness. Hiring an around-the-clock sitter does not demonstrate that the client’s family understands complementary therapies. 9. A nurse is caring for a terminally ill client who has just died in a hospital setting with family members at the bedside. Which action should the nurse take first? a. Call for emergency assistance so that resuscitation procedures can begin. b. Ask family members if they would like to spend time alone with the client. c. Ensure that a death certificate has been completed by the physician. d. Request family members to prepare the client’s body for the funeral home. Before moving the client’s body to the funeral home, the nurse should ask family members if they would like to be alone with the client. Emergency assistance will not be necessary. Although it is important to ensure that a death certificate has been completed before the client is moved to the mortuary, the nurse first should ask family members if they would like to be alone with the client. The client’s family should not be expected to prepare the body for the funeral home. 10. A nurse assesses a client who is dying. Which manifestation of a dying client should the nurse assess to determine whether the client is near death? a. Level of consciousness b. Respiratory rate c. Bowel sounds d. Pain level on a 0-to-10 scale Although all of these assessments should be performed during the dying process, periods of apnea and Cheyne- Strokes respirations indicate death is near. As peripheral circulation decreases, the client’s level of consciousness and bowel sounds decrease, and the client would be unable to provide a numeric number on a pain scale. Even with these other symptoms, the nurse should continue to assess respiratory rate throughout the dying process. As the rate drops significantly and breathing becomes agonal, death is near. 11. A nurse is caring for a client who is terminally ill. The client’s spouse states, “I am concerned because he does not want to eat.” How should the nurse respond? a. “Let him know that food is available if he wants it, but do not insist that he eat.” b. “A feeding tube can be placed in the nose to provide important nutrients.” c. “Force him to eat even if he does not feel hungry, or he will die sooner.” d. “He is getting all the nutrients he needs through his intravenous catheter.” When family members understand that the client is not suffering from hunger and is not “starving to death,” they may allow the client to determine when, what, or if to eat. Often, as death approaches, metabolic needs decrease and clients do not feel the sensation of hunger. Forcing them to eat frustrates the client and the family. 12. A nurse discusses inpatient hospice with a client and the client’s family. A family member expresses concern that her loved one will receive only custodial care. How should the nurse respond? a. “The goal of palliative care is to provide the greatest degree of comfort possible and help the dying person enjoy whatever time is left.” b. “Palliative care will release you from the burden of having to care for someone in the home. It does not mean that curative treatment will stop.” c. “A palliative care facility is like a nursing home and costs less than a hospital because only pain medications are given.” d. “Your relative is unaware of her surroundings and will not notice the difference between her home and a palliative care facility.” Palliative care provides an increased level of personal care designed to manage symptom distress. The focus is on pain control and helping the relative die with dignity. 13. An intensive care nurse discusses withdrawal of care with a client’s family. The family expresses concerns related to discontinuation of therapy. How should the nurse respond? a. “I understand your concerns, but in this state, discontinuation of care is not a form of active euthanasia.” b. “You will need to talk to the provider because I am not legally allowed to participate in the withdrawal of life support.” c. “I realize this is a difficult decision. Discontinuation of therapy will allow the client to die a natural death.” d. “There is no need to worry. Most religious organizations support the client’s decision to stop medical treatment.” The nurse should validate the family’s concerns and provide accurate information about the discontinuation of therapy. The other statements address specific issues related to the withdrawal of care but do not provide appropriate information about their purpose. If the client’s family asks for specific information about euthanasia, legal, or religious issues, the nurse should provide unbiased information about these topics. 14. A hospice nurse is caring for a variety of clients who are dying. Which end-of-life and death ritual is paired with the correct religion? a. Roman Catholic – Autopsies are not allowed except under special circumstances. b. Christian – Upon death, a religious leader should perform rituals of bathing and wrapping the body in cloth. c. Judaism – A person who is extremely ill and dying should not be left alone. d. Islam – An ill or dying person should receive the Sacrament of the Sick. According to Jewish law, a person who is extremely ill or dying should not be left alone. Orthodox Jews do not allow autopsies except under special circumstances. The Islamic faith requires a religious leader to perform rituals of bathing and wrapping the body in cloth upon death. A Catholic priest performs the Sacrament of the Sick for ill or dying people. 1. A hospice nurse is caring for a dying client and her family members. Which interventions should the nurse implement? (Select all that apply.) a. Teach family members about physical signs of impending death. b. Encourage the management of adverse symptoms. c. Assist family members by offering an explanation for their loss. d. Encourage reminiscence by both client and family members. e. Avoid spirituality because the client’s and the nurse’s beliefs may not be congruent. The nurse should teach family members about the physical signs of death, because family members often become upset when they see physiologic changes in their loved one. Palliative care includes management of symptoms so that the peaceful death of the client is facilitated. Reminiscence will help both the client and family members cope with the dying process. The nurse is not expected to explain why this is happening to the family’s loved one. The nurse can encourage spirituality if the client is agreeable, regardless of whether the client’s religion is the same. 2. A nurse admits an older adult client to the hospital. Which criterion should the nurse use to determine if the client can make his own medical decisions? (Select all that apply.) a. Can communicate his treatment preferences b. Is able to read and write at an eighth-grade level c. Is oriented enough to understand information provided d. Can evaluate and deliberate information e. Has completed an advance directive To have decision-making ability, a person must be able to perform three tasks: receive information (but not necessarily oriented ´ 4); evaluate, deliberate, and mentally manipulate information; and communicate a treatment preference. The client does not have to read or write at a specific level. 3. A hospice nurse plans care for a client who is experiencing pain. Which complementary therapies should the nurse incorporate in this client’s pain management plan? (Select all that apply.) a. Play music that the client enjoys. b. Massage tissue that is tender from radiation therapy. c. Rub lavender lotion on the client’s feet. d. Ambulate the client in the hall twice a day. e. Administer intravenous morphine. Complementary therapies for pain management include massage therapy, music therapy, Therapeutic Touch, and aromatherapy. Nurses should not massage over sites of tissue damage from radiation therapy. Ambulation and intravenous morphine are not complementary therapies for pain management. 4. A nurse teaches a client’s family members about signs and symptoms of approaching death. Which manifestations should the nurse include in this teaching? (Select all that apply.) a. Warm and flushed extremities b. Long periods of insomnia c. Increased respiratory rate d. Decreased appetite e. Congestion and gurgling Common physical signs and symptoms of approaching death including coolness of extremities, increased sleeping, irregular and slowed breathing rate, a decrease in fluid and food intake, congestion and gurgling, incontinence, disorientation, and restlessness. Chapter 8: Concepts of Emergency and Trauma Nursing 1. An emergency room nurse assesses a client who has been raped. With which health care team member should the nurse collaborate when planning this client’s care? a. Emergency medicine physician b. Case manager c. Forensic nurse examiner d. Psychiatric crisis nurse All other members of the health care team listed may be used in the management of this client’s care. However, the forensic nurse examiner is educated to obtain client histories and collect evidence dealing with the assault, and can offer the counseling and follow-up needed when dealing with the victim of an assault. 2. The emergency department team is performing cardiopulmonary resuscitation on a client when the client’s spouse arrives at the emergency department. Which action should the nurse take first? a. Request that the client’s spouse sit in the waiting room. b. Ask the spouse if he wishes to be present during the resuscitation. c. Suggest that the spouse begin to pray for the client. d. Refer the client’s spouse to the hospital’s crisis team. If resuscitation efforts are still under way when the family arrives, one or two family members may be given the opportunity to be present during lifesaving procedures. The other options do not give the spouse the opportunity to be present for the client or to begin to have closure. 3. An emergency room nurse is triaging victims of a multi-casualty event. Which client should receive care first? a. A 30-year-old distraught mother holding her crying child b. A 65-year-old conscious male with a head laceration c. A 26-year-old male who has pale, cool, clammy skin d. A 48-year-old with a simple fracture of the lower leg The client with pale, cool, clammy skin is in shock and needs immediate medical attention. The mother does not have injuries and so would be the lowest priority. The other two people need medical attention soon, but not at the expense of a person in shock. 4. While triaging clients in a crowded emergency department, a nurse assesses a client who presents with symptoms of tuberculosis. Which action should the nurse take first? a. Apply oxygen via nasal cannula. b. Administer intravenous 0.9% saline solution. c. Transfer the client to a negative-pressure room. d. Obtain a sputum culture and sensitivity. A client with signs and symptoms of tuberculosis or other airborne pathogens should be placed in a negative- pressure room to prevent contamination of staff, clients, and family members in the crowded emergency department. 5. A nurse is triaging clients in the emergency department (ED). Which client should the nurse prioritize to receive care first? a. A 22-year-old with a painful and swollen right wrist b. A 45-year-old reporting chest pain and diaphoresis c. A 60-year-old reporting difficulty swallowing and nausea d. An 81-year-old with a respiratory rate of 28 breaths/min and a temperature of 101° F A client experiencing chest pain and diaphoresis would be classified as emergent and would be triaged immediately to a treatment room in the ED. The other clients are more stable. 6. A nurse is evaluating levels and functions of trauma centers. Which function is appropriately paired with the level of the trauma center? a. Level I – Located within remote areas and provides advanced life support within resource capabilities b. Level II – Located within community hospitals and provides care to most injured clients c. Level III – Located in rural communities and provides only basic care to clients d. Level IV – Located in large teaching hospitals and provides a full continuum of trauma care for all clients Level I trauma centers are usually located in large teaching hospital systems and provide a full continuum of trauma care for all clients. Both Level II and Level III facilities are usually located in community hospitals. These trauma centers provide care for most clients and transport to Level I centers when client needs exceed resource capabilities. Level IV trauma centers are usually located in rural and remote areas. These centers provide basic care, stabilization, and advanced life support while transfer arrangements to higher-level trauma centers are made. 7. Emergency medical technicians arrive at the emergency department with an unresponsive client who has an oxygen mask in place. Which action should the nurse take first? a. Assess that the client is breathing adequately. b. Insert a large-bore intravenous line. c. Place the client on a cardiac monitor. d. Assess for the best neurologic response. The highest-priority intervention in the primary survey is to establish that the client is breathing adequately. Even though this client has an oxygen mask on, he or she may not be breathing, or may be breathing inadequately with the device in place. 8. A trauma client with multiple open wounds is brought to the emergency department in cardiac arrest. Which action should the nurse take prior to providing advanced cardiac life support? a. Contact the on-call orthopedic surgeon. b. Don personal protective equipment. c. Notify the Rapid Response Team. d. Obtain a complete history from the paramedic. Nurses must recognize and plan for a high risk of contamination with blood and body fluids when engaging in trauma resuscitation. Standard Precautions should be taken in all resuscitation situations and at other times when exposure to blood and body fluids is likely. Proper attire consists of an impervious cover gown, gloves, eye protection, a facemask, a surgical cap, and shoe covers. 9. A nurse is triaging clients in the emergency department. Which client should be considered “urgent”? a. A 20-year-old female with a chest stab wound and tachycardia b. A 45-year-old homeless man with a skin rash and sore throat c. A 75-year-old female with a cough and a temperature of 102° F d. A 50-year-old male with new-onset confusion and slurred speech A client with a cough and a temperature of 102° F is urgent. This client is at risk for deterioration and needs to be seen quickly, but is not in an immediately life-threatening situation. The client with a chest stab wound and tachycardia and the client with new-onset confusion and slurred speech should be triaged as emergent. The client with a skin rash and a sore throat is not at risk for deterioration and would be triaged as nonurgent. 10. An emergency department nurse is caring for a client who has died from a suspected homicide. Which action should the nurse take? a. Remove all tubes and wires in preparation for the medical examiner. b. Limit the number of visitors to minimize the family’s trauma. c. Consult the bereavement committee to follow up with the grieving family. d. Communicate the client’s death to the family in a simple and concrete manner. When dealing with clients and families in crisis, communicate in a simple and concrete manner to minimize confusion. Tubes must remain in place for the medical examiner. Family should be allowed to view the body. Offering to call for additional family support during the crisis is suggested. The bereavement committee should be consulted, but this is not the priority at this time. 11. An emergency department (ED) case manager is consulted for a client who is homeless. Which intervention should the case manager provide? a. Communicate client needs and restrictions to support staff. b. Prescribe low-cost antibiotics to treat community-acquired infection. c. Provide referrals to subsidized community-based health clinics. d. Offer counseling for substance abuse and mental health disorders. Case management interventions include facilitating referrals to primary care providers who are accepting new clients or to subsidized community-based health clinics for clients or families in need of routine services. The ED nurse is accountable for communicating pertinent staff considerations, client needs, and restrictions to support staff (e.g., physical limitations, isolation precautions) to ensure that ongoing client and staff safety issues are addressed. The ED physician prescribes medications and treatments. The psychiatric nurse team evaluates clients with emotional behaviors or mental illness and facilitates the follow-up treatment plan, including possible admission to an appropriate psychiatric facility. 12. An emergency department nurse is caring for a client who is homeless. Which action should the nurse take to gain the client’s trust? a. Speak in a quiet and monotone voice. b. Avoid eye contact with the client. c. Listen to the client’s concerns and needs. d. Ask security to store the client’s belongings. To demonstrate behaviors that promote trust with homeless clients, the emergency room nurse should make eye contact (if culturally appropriate), speak calmly, avoid any prejudicial or stereotypical remarks, show genuine care and concern by listening, and follow through on promises. The nurse should also respect the client’s belongings and personal space. 13. A nurse is triaging clients in the emergency department. Which client should the nurse classify as “nonurgent?” a. A 44-year-old with chest pain and diaphoresis b. A 50-year-old with chest trauma and absent breath sounds c. A 62-year-old with a simple fracture of the left arm d. A 79-year-old with a temperature of 104° F A client in a nonurgent category can tolerate waiting several hours for health care services without a significant risk of clinical deterioration. The client with a simple arm fracture and palpable radial pulses is currently stable, is not at significant risk of clinical deterioration, and would be considered nonurgent. The client with chest pain and diaphoresis and the client with chest trauma are emergent owing to the potential for clinical deterioration and would be seen immediately. The client with a high fever may be stable now but also has a risk of deterioration. 1. A nurse is caring for clients in a busy emergency department. Which actions should the nurse take to ensure client and staff safety? (Select all that apply.) a. Leave the stretcher in the lowest position with rails down so that the client can access the bathroom. b. Use two identifiers before each intervention and before mediation administration. c. Attempt de-escalation strategies for clients who demonstrate aggressive behaviors. d. Search the belongings of clients with altered mental status to gain essential medical information. e. Isolate clients who have immune suppression disorders to prevent hospital-acquired infections. To ensure client and staff safety, nurses should use two identifiers per The Joint Commission’s National Patient Safety Goals; follow the hospital’s security plan, including de-escalation strategies for people who demonstrate aggressive or violent tendencies; and search belongings to identify essential medical information. Nurses should also use standard fall prevention interventions, including leaving stretchers in the lowest position with rails up, and isolating clients who present with signs and symptoms of contagious infectious disorders. 2. An emergency department (ED) nurse is preparing to transfer a client to the trauma intensive care unit. Which information should the nurse include in the nurse-to-nurse hand-off report? (Select all that apply.) a. Mechanism of injury b. Diagnostic test results c. Immunizations d. List of home medications e. Isolation precautions Hand-off communication should be comprehensive so that the receiving nurse can continue care for the client fluidly. Communication should be concise and should include only the most essential information for a safe transition in care. Hand-off communication should include the client’s situation (reason for being in the ED), brief medical history, assessment and diagnostic findings, Transmission-Based Precautions needed, interventions provided, and response to those interventions. 3. An emergency room nurse is caring for a trauma client. Which interventions should the nurse perform during the primary survey? (Select all that apply.) a. Foley catheterization b. Needle decompression c. Initiating IV fluids d. Splinting open fractures e. Endotracheal intubation f. Removing wet clothing g. Laceration repair 4. The complex care provided during an emergency requires interdisciplinary collaboration. Which interdisciplinary team members are paired with the correct responsibilities? (Select all that apply.) a. Psychiatric crisis nurse – Interacts with clients and families when sudden illness, serious injury, or death of a loved one may cause a crisis b. Forensic nurse examiner – Performs rapid assessments to ensure clients with the highest acuity receive the quickest evaluation, treatment, and prioritization of resources c. Triage nurse – Provides basic life support interventions such as oxygen, basic wound care, splinting, spinal immobilization, and monitoring of vital signs d. Emergency medical technician – Obtains client histories, collects evidence, and offers counseling and follow- up care for victims of rape, child abuse, and domestic violence e. Paramedic – Provides prehospital advanced life support, including cardiac monitoring, advanced airway management, and medication administration The psychiatric crisis nurse evaluates clients with emotional behaviors or mental illness and facilitates follow- up treatment plans. The psychiatric crisis nurse also works with clients and families when experiencing a crisis. Paramedics are advanced life support providers who can perform advanced techniques that may include cardiac monitoring, advanced airway management and intubation, establishing IV access, and administering drugs en route to the emergency department. The forensic nurse examiner is trained to recognize evidence of abuse and to intervene on the client’s behalf. The forensic nurse examiner will obtain client histories, collect evidence, and offer counseling and follow-up care for victims of rape, child abuse, and domestic violence. The triage nurse performs rapid assessments to ensure clients with the highest acuity receive the quickest evaluation, treatment, and prioritization of resources. The emergency medical technician is usually the first caregiver and provides basic life support and transportation to the emergency department. 5. A nurse prepares to discharge an older adult client home from the emergency department (ED). Which actions should the nurse take to prevent future ED visits? (Select all that apply.) a. Provide medical supplies to the family. b. Consult a home health agency. c. Encourage participation in community activities. d. Screen for depression and suicide. e. Complete a functional assessment. Due to the high rate of suicide among older adults, a nurse should assess all older adults for depression and suicide. The nurse should also screen older adults for functional assessment, cognitive assessment, and risk for falls to prevent future ED visits. Chapter 13: Infusion Therapy 1.A nurse is caring for a client who has just had a central venous access line inserted. Which action should the nurse take next? a. Begin the prescribed infusion via the new access. b. Ensure an x-ray is completed to confirm placement. c. Check medication calculations with a second RN. d. Make sure the solution is appropriate for a central line. A central venous access device, once placed, needs an x-ray confirmation of proper placement before it is used. The bedside nurse would be responsible for beginning the infusion once placement has been verified. Any IV solution can be given through a central line. 2.A nurse assesses a client who has a radial artery catheter. Which assessment should the nurse complete first? a. Amount of pressure in fluid container b. Date of catheter tubing change c. Percent of heparin in infusion container d. Presence of an ulnar pulse An intra-arterial catheter may cause arterial occlusion, which can lead to absent or decreased perfusion to the extremity. Assessment of an ulnar pulse is one way to assess circulation to the arm in which the catheter is located. The nurse would note that there is enough pressure in the fluid container to keep the system flushed, and would check to see whether the catheter tubing needs to be changed. However, these are not assessments of greatest concern. Because of heparin-induced thrombocytopenia, heparin is not used in most institutions for an arterial catheter. 3.A nurse teaches a client who is being discharged home with a peripherally inserted central catheter (PICC). Which statement should the nurse include in this client’s teaching? “Avoid carrying your grandchild with the arm that has a. the central catheter.” b “Be sure to place the arm with the central catheter in a . sling during the day.” “Flush the peripherally inserted central catheter line c. with normal saline daily.” d “You can use the arm with the central catheter for most . activities of daily living.” A properly placed PICC (in the antecubital fossa or the basilic vein) allows the client considerable freedom of movement. Clients can participate in most activities of daily living; however, heavy lifting can dislodge the catheter or occlude the lumen. Although it is important to keep the insertion site and tubing dry, the client can shower. The device is flushed with heparin. 4.A nurse is caring for a client who is having a subclavian central venous catheter inserted. The client begins to report chest pain and difficulty breathing. After administering oxygen, which action should the nurse take next? a. Administer a sublingual nitroglycerin tablet. b. Prepare to assist with chest tube insertion. c. Place a sterile dressing over the IV site. d. Re-position the client into the Trendelenburg position. An insertion-related complication of central venous catheters is a pneumothorax. Signs and symptoms of a pneumothorax include chest pain and dyspnea. Treatment includes removing the catheter, administering oxygen, and placing a chest tube. Pain is caused by the pneumothorax, which must be taken care of with a chest tube insertion. Use of a sterile dressing and placement of the client in a Trendelenburg position are not indicated for the primary problem of a pneumothorax. 5.A nurse is caring for a client who is receiving an epidural infusion for pain management. Which assessment finding requires immediate intervention from the nurse? a. Redness at the catheter insertion site b. Report of headache and stiff neck c. Temperature of 100.1° F (37.8° C) d. Pain rating of 8 on a scale of 0 to 10 Complications of epidural therapy include infection, bleeding, leakage of cerebrospinal fluid, occlusion of the catheter lumen, and catheter migration. Headache, neck stiffness, and a temperature higher than 101° F are signs of meningitis and should be reported to the provider immediately. The other findings are important but do not require immediate intervention. 6.A nurse assesses a client who had an intraosseous catheter placed in the left leg. Which assessment finding is of greatest concern? a. The catheter has been in place for 20 hours. b The client has poor vascular access in the upper . extremities. c. The catheter is placed in the proximal tibia. d . The client’s left lower extremity is cool to the touch. Compartment syndrome is a condition in which increased tissue perfusion in a confined anatomic space causes decreased blood flow to the area. A cool extremity can signal the possibility of this syndrome. All other findings are important; however, the possible development of compartment syndrome requires immediate intervention because the client could require amputation of the limb if the nurse does not correctly assess this perfusion problem. 7.A nurse is assessing clients who have intravenous therapy prescribed. Which assessment finding for a client with a peripherally inserted central catheter (PICC) requires immediate attention? a. The initial site dressing is 3 days old. b. The PICC was inserted 4 weeks ago. c. A securement device is absent. d. Upper extremity swelling is noted. Upper extremity swelling could indicate infiltration, and the PICC will need to be removed. The initial dressing over the PICC site should be changed within 24 hours. This does not require immediate attention, but the swelling does. The dwell time for PICCs can be months or even years. Securement devices are being used more often now to secure the catheter in place and prevent complications such as phlebitis and infiltration. The IV should have one, but this does not take priority over the client whose arm is swollen. 8.A nurse assesses a client’s peripheral IV site, and notices edema and tenderness above the site. Which action should the nurse take next? a. Apply cold compresses to the IV site. b. Elevate the extremity on a pillow. c. Flush the catheter with normal saline. d. Stop the infusion of intravenous fluids. Infiltration occurs when the needle dislodges partially or completely from the vein. Signs of infiltration include edema and tenderness above the site. The nurse should stop the infusion and remove the catheter. Cold compresses and elevation of the extremity can be done after the catheter is discontinued to increase client comfort. Alternatively, warm compresses may be prescribed per institutional policy and may help speed circulation to the area. 9.While assessing a client’s peripheral IV site, the nurse observes a streak of red along the vein path and palpates a 4-cm venous cord. How should the nurse document this finding? a. “Grade 3 phlebitis at IV site” b. “Infection at IV site” c. “Thrombosed area at IV site” d. “Infiltration at IV site” The presence of a red streak and palpable cord indicates grade 3 phlebitis. No information in the description indicates that infection, thrombosis, or infiltration is present. 10.A nurse responds to an IV pump alarm related to increased pressure. Which action should the nurse take first? a. Check for kinking of the catheter. b. Flush the catheter with a thrombolytic enzyme. c. Get a new infusion pump. d. Remove the IV catheter. Fluid flow through the infusion system requires that pressure on the external side be greater than pressure at the catheter tip. Fluid flow can be slowed for many reasons. A common reason, and one that is easy to correct, is a kinked catheter. If this is not the cause of the pressure alarm, the nurse may have to ascertain whether a clot has formed inside the catheter lumen, or if the pump is no longer functional. Removal of the IV catheter and placement of a new IV catheter should be completed when no other option has resolved the problem. 11.A nurse prepares to insert a peripheral venous catheter in an older adult client. Which action should the nurse take to protect the client’s skin during this procedure? a. Lower the extremity below the level of the heart. b. Apply warm compresses to the extremity. c. Tap the skin lightly and avoid slapping. d. Place a washcloth between the skin and tourniquet. To protect the client’s skin, the nurse should place a washcloth or the client’s gown between the skin and tourniquet. The other interventions are methods to distend the vein but will not protect the client’s skin. 12.A nurse delegates care to an unlicensed assistive personnel (UAP). Which statement should the nurse include when delegating hygiene for a client who has a vascular access device? “Provide a bed bath instead of letting the client take a a. shower.” b . “Use sterile technique when changing the dressing.” “Disconnect the intravenous fluid tubing prior to the c. client’s bath.” d “Use a plastic bag to cover the extremity with the . device.” The nurse should ask the UAP to cover the extremity with the vascular access device with a plastic bag or wrap to keep the dressing and site dry. The client may take a shower with a vascular device. The nurse should disconnect IV fluid tubing prior to the bath and change the dressing using sterile technique if necessary. These options are not appropriate to delegate to the UAP. 13.A nurse teaches a client who is prescribed a central vascular access device. Which statement should the nurse include in this client’s teaching? “You will need to wear a sling on your arm while the a. device is in place.” b “There is no risk of infection because sterile technique . will be used during insertion.” “Ask all providers to vigorously clean the connections c. prior to accessing the device.” d “You will not be able to take a bath with this vascular . access device.” Clients should be actively engaged in the prevention of catheter-related bloodstream infections and taught to remind all providers to perform hand hygiene and vigorously clean connections prior to accessing the device. The other statements are incorrect. 14.A nurse is caring for a client with a peripheral vascular access device who is experiencing pain, redness, and swelling at the site. After removing the device, which action should the nurse take to relieve pain? a. Administer topical lidocaine to the site. b. Place warm compresses on the site. c. Administer prescribed oral pain medication. d. Massage the site with scented oils. At the first sign of phlebitis, the catheter should be removed and warm compresses used to relieve pain. The other options are not appropriate for this type of pain. 15.A nurse assesses a client who was started on intraperitoneal therapy 5 days ago. The client reports abdominal pain and “feeling warm.” For which complication of this therapy should the nurse assess this client? a. Allergic reaction b. Bowel obstruction c. Catheter lumen occlusion d. Infection Fever, abdominal pain, abdominal rigidity, and rebound tenderness may be present in the client who has peritonitis related to intraperitoneal therapy. Peritonitis is preventable by using strict aseptic technique in handling all equipment and infusion supplies. An allergic reaction would occur earlier in the course of treatment. Bowel obstruction and catheter lumen occlusion can occur but would present clinically in different ways. 16.A medical-surgical nurse is concerned about the incidence of complications related to IV therapy, including bloodstream infection. Which intervention should the nurse suggest to the management team to make the biggest impact on decreasing complications? a. Initiate a dedicated team to insert access devices. b . Require additional education for all nurses. c. Limit the use of peripheral venous access devices. d Perform quality control testing on skin preparation . products. The Centers for Disease Control and Prevention recommends having a dedicated IV team to reduce complications, save money, and improve client satisfaction and outcomes. In-service education would always be helpful, but it would not have the same outcomes as an IV team. Limiting IV starts to the most experienced nurses does not allow newer nurses to gain this expertise. The quality of skin preparation products is only one aspect of IV insertion that could contribute to infection. 17.A nurse prepares to flush a peripherally inserted central catheter (PICC) line with 50 units of heparin. The pharmacy supplies a multi-dose vial of heparin with a concentration of 100 units/mL. Which of the syringes shown below should the nurse use to draw up and administer the heparin? a. b. c. d. 10 mL Always use a 10-mL syringe when flushing PICC lines because a smaller syringe creates higher pressure, which could rupture the lumen of the PICC. 18.A home care nurse prepares to administer intravenous medication to a client. The nurse assesses the site and reviews the client’s chart prior to administering the medication: January 23 (Today): Right upper extremity PICC is intact, patent, and has a good blood return. Site clean and free from manifestations of infiltration, irritation, and infection. –Sue Franks, RN. January 20: Purulent drainage from sacral wound. Wound cleansed and dressing changed. Dr. Smith notified and updated on client status. New orders received for intravenous antibiotics. –Sue Franks, RN. January 13: Client alert and oriented. Sacral wound dressing changed. –Sue Franks, RN. January 6: Right upper extremity PICC inserted. No complications. Discharged with home health care. –Dr. Smith Based on the information provided, which action should the nurse take? a. Notify the health care provider. b. Administer the prescribed medication. c. Discontinue the PICC. d. Switch the medication to the oral route. A PICC that is functioning well without inflammation or infection may remain in place for months or even years. Because the line shows no signs of complications, it is permissible to administer the IV antibiotic. There is no need to call the physician to have the IV route changed to an oral route. 1.A registered nurse (RN) delegates client care to an experienced licensed practical nurse (LPN). Which standards should guide the RN when delegating aspects of IV therapy to the LPN? (Select all that apply.) a. State Nurse Practice Act b. The facility’s Policies and Procedures manual c. The LPN’s level of education and experience d. The Joint Commission’s goals and criterion e. Client needs and prescribed orders The state Nurse Practice Act will have the information the RN needs, and in some states, LPNs are able to perform specific aspects of IV therapy. However, in a client care situation, it may be difficult and time- consuming to find it and read what LPNs are permitted to do, so another good solution would be for the nurse to check facility policy and follow it. 2.A nurse assesses a client who has a peripherally inserted central catheter (PICC). For which complications should the nurse assess? (Select all that apply.) a. Phlebitis b. Pneumothorax c. Thrombophlebitis d. Excessive bleeding e. Extravasation Although the complication rate with PICCs is fairly low, the most common complications are phlebitis, thrombophlebitis, and catheter-related bloodstream infection. Pneumothorax, excessive bleeding, and extravasation are not common complications. 3.A nurse prepares to administer a blood transfusion to a client, and checks the blood label with a second registered nurse using the International Society of Blood Transfusion (ISBT) universal bar-coding system to ensure the right blood for the right client. Which components must be present on the blood label in bar code and in eye-readable format? (Select all that apply.) a. Unique facility identifier b. Lot number related to the donor c. Name of the client receiving blood d. ABO group and Rh type of the donor e. Blood type of the client receiving blood The ISBT universal bar-coding system includes four components: (1) the unique facility identifier, (2) the lot number relating to the donor, (3) the product code, and (4) the ABO group and Rh type of the donor. 4.A nurse assists with the insertion of a central vascular access device. Which actions should the nurse ensure are completed to prevent a catheter-related bloodstream infection? (Select all that apply.) Include a review for the need of the device each day in a. the client’s plan of care. b Remind the provider to perform hand hygiene prior to . starting the procedure. Cleanse the preferred site with alcohol and let it dry c. completely before insertion. d Ask everyone in the room to wear a surgical mask . during the procedure. Plan to complete a sterile dressing change on the device e. every day. 1.A client is prescribed 1000 mL of normal saline to infuse over 24 hours. At what rate should the nurse set the pump (mL/hr) to deliver this infusion? (Record your answer using a whole number.) mL/hr 42 1000 mL ÷ 24 hours = 41.6 mL/hr. 2.A client is prescribed 250 mL of normal saline to infuse over 4 hours via gravity. The facility supplies gravity tubing with a drip factor of 15 drops/mL. At what rate (drops/min) should the nurse set the infusion to deliver? (Record your answer using a whole number.) 16 drops/min Chapter 15: Care of Intraoperative Patients 1. The circulating nurse is plugging in a piece of equipment and notes that the cord is frayed. What action by the nurse is best? a. Call maintenance for repair. b. Check the machine before using. c. Get another piece of equipment. d. Notify the charge nurse. The circulating nurse is responsible for client safety. If an electrical cord is frayed, the risk of fire or sparking increases. The nurse should obtain a replacement. The nurse should also tag the original equipment for repair as per agency policy. Checking the equipment is not important as the nurse should not even attempt to use it. Calling maintenance or requesting maintenance per facility protocol is important, but first ensure client safety by having a properly working piece of equipment for the procedure about to take place. The charge nurse probably does need to know of the need for equipment repair, but ensuring client safety is the priority. 2. The circulating nurse and preoperative nurse are reviewing the chart of a client scheduled for minimally invasive surgery (MIS). What information on the chart needs to be reported to the surgeon as a priority? a. Allergies noted and allergy band on b. Consent for MIS procedure only c. No prior anesthesia exposure d. NPO status for the last 8 hours All MIS procedures have the potential for becoming open procedures depending on findings and complications. The client’s consent should include this possibility. The nurse should report this finding to the surgeon prior to surgery taking place. Having allergies noted and an allergy band applied is standard procedure. Not having any prior surgical or anesthesia exposure is not the priority. Maintaining NPO status as prescribed is standard procedure. 3. A client is having robotic surgery. The circulating nurse observes the instruments being inserted, then the surgeon appears to “break scrub” when going to the console and sitting down. What action by the nurse is best? a. Call a “time-out” to discuss sterile procedure and scrub technique. b. Document the time the robotic portion of the procedure begins. c. Inform the surgeon that the scrub preparation has been compromised. d. Report the surgeon’s actions to the charge nurse and unit manager. During a robotic operative procedure, the surgeon inserts the articulating arms into the client, then “breaks scrub” to sit at the viewing console to perform the operation. The nurse should document the time the robotic portion of the procedure began. There is no need for the other interventions. 4. The circulating nurse is in the operating room and sees the surgeon don gown and gloves using appropriate sterile procedure. The surgeon then folds the hands together and places them down below the hips. What action by the nurse is most appropriate? a. Ask the surgeon to change the sterile gown. b. Do nothing; this is acceptable sterile procedure. c. Inform the surgeon that the sterile field has been broken. d. Obtain a new pair of sterile gloves for the surgeon to put on. The surgical gown is considered sterile from the chest to the level of the surgical field. By placing the hands down by the hips, the surgeon has broken sterile field. 5. A client is in stage 2 of general anesthesia. What action by the nurse is most important? a. Keeping the room quiet and calm b. Being prepared to suction the airway c. Positioning the client correctly d. Warming the client with blankets During stage 2 of general anesthesia (excitement, delirium), the client can vomit and aspirate. The nurse must be ready to react to this potential occurrence by being prepared to suction the client’s airway. Keeping the room quiet and calm does help the client enter the anesthetic state, but is not the priority. Positioning the client usually occurs during stage 3 (operative anesthesia). Keeping the client warm is important throughout to prevent hypothermia. 6. A client is having surgery. The circulating nurse notes the client’s oxygen saturation is 90% and the heart rate is 110 beats/min. What action by the nurse is best? a. Assess the client’s end-tidal carbon dioxide level. b. Document the findings in the client’s chart. c. Inform the anesthesia provider of these values. d. Prepare to administer dantrolene sodium (Dantrium). Malignant hyperthermia is a rare but serious reaction to anesthesia. The triad of early signs include decreased oxygen saturation, tachycardia, and elevated end-tidal carbon dioxide (CO2) level. The nurse should quickly check the end-tidal CO2 and then report findings to the anesthesia provider and surgeon. Documentation is vital, but not the most important action at this stage. Dantrolene sodium is the drug of choice if the client does have malignant hyperthermia. 7. A nurse is monitoring a client after moderate sedation. The nurse documents the client’s Ramsay Sedation Scale (RSS) score at 3. What action by the nurse is best? a. Assess the client’s gag reflex. b. Begin providing discharge instructions. c. Document findings and continue to monitor. d. Increase oxygen and notify the provider. An RSS score of 3 means the client is able to respond quickly, but only to commands. The client has not had enough time to fully arouse. The nurse should document the findings and continue to monitor per agency policy. If the client had an oral endoscopy or was intubated, checking the gag reflex would be appropriate prior to permitting eating or drinking. The client is not yet awake enough for teaching. There is no need to increase oxygen and notify the provider. 8. A client is scheduled for a below-the-knee amputation. The circulating nurse ensures the proper side is marked prior to the start of surgery. What action by the nurse is most appropriate? a. Facilitate marking the site with the client and surgeon. b. Have the client mark the operative site. c. Mark the operative site with a waterproof marker. d. Tell the surgeon it is time to mark the surgical site. The Joint Commission now recommends that both the client and the surgeon mark the operative site together in order to prevent wrong-site surgery. The nurse should facilitate this process. 9. A client has received intravenous anesthesia during an operation. What action by the postanesthesia care nurse is most important? a. Assist with administering muscle relaxants to the client. b. Place the client on a cardiac monitor and pulse oximeter. c. Prepare to administer intravenous antiemetics to the client. d. Prevent the client from experiencing postoperative shivering. Intravenous anesthetic agents have the potential to cause respiratory and circulatory depression. The nurse should ensure the client is on a cardiac monitor and pulse oximeter. Muscle relaxants are not indicated for this client at this time. Intravenous anesthetics have a lower rate of postoperative nausea and vomiting than other types. Shivering can occur in any client, but is more common after inhalation agents. 10. A circulating nurse has transferred an older client to the operating room. What action by the nurse is most important for this client? a. Allow the client to keep hearing aids in until anesthesia begins. b. Pad the table as appropriate for the surgical procedure. c. Position the client for maximum visualization of the site. d. Stay with the client, providing emotional comfort and support. Many older clients have sensory loss. To help prevent disorientation, facilities often allow older clients to keep their eyeglasses on and hearing aids in until the start of anesthesia. The other actions are appropriate for all operative clients. 11. A circulating nurse wishes to provide emotional support to a client who was just transferred to the operating room. What action by the nurse would be best? a. Administer anxiolytics. b. Give the client warm blankets. c. Introduce the surgical staff. d. Remain with the client. The nurse can provide emotional support by remaining with the client until anesthesia has been provided. An extremely anxious client may need anxiolytics, but not all clients require this for emotional support. Physical comfort and introductions can also help decrease anxiety. 12. A client in the operating room has developed malignant hyperthermia. The client’s potassium is 6.5 mEq/L. What action by the nurse takes priority? a. Administer 10 units of regular insulin. b. Administer nifedipine (Procardia). c. Assess urine for myoglobin or blood. d. Monitor the client for dysrhythmias. For hyperkalemia in a client with malignant hyperthermia, the nurse administers 10 units of regular insulin in 50 mL of 50% dextrose. This will force potassium back into the cells rapidly. Nifedipine is a calcium channel blocker used to treat hypertension and dysrhythmias, and should not be used in a client with malignant hyperthermia. Assessing the urine for blood or myoglobin is important, but does not take priority. Monitoring the client for dysrhythmias is also important due to the potassium imbalance, but again does not take priority over treating the potassium imbalance. 1. A student nurse observing in the operating room notes that the functions of the Certified Registered Nurse First Assistant (CRNFA) include which activities? (Select all that apply.) a. Dressing the surgical wound b. Grafting new or synthetic skin c. Reattaching severed nerves d. Suctioning the surgical site e. Suturing the surgical wound The CRNFA can perform tasks under the direction of the surgeon such as suturing and dressing surgical wounds, cutting away tissue, suctioning the wound to improve visibility, and holding retractors. Reattaching severed nerves and performing grafts would be the responsibility of the surgeon. 2. The nursing student observing in the perioperative area notes the unique functions of the circulating nurse, which include which roles? (Select all that apply.) a. Ensuring the client’s safety b. Accounting for all sharps c. Documenting all care given d. Maintaining the sterile field e. Monitoring traffic in the room The circulating nurse has several functions, including maintaining client safety and privacy, monitoring traffic in and out of the operating room, assessing fluid losses, reporting findings to the surgeon and anesthesia provider, anticipating needs of the team, and communicating to the family. The circulating nurse and scrub person work together to ensure accurate counts of sharps, sponges, and instruments. The circulating nurse also documents care, but in the perioperative area, the preoperative or holding room nurse would also document care received there. Maintaining the sterile field is a joint responsibility among all members of the surgical team. 3. The circulating nurse reviews the day’s schedule and notes clients who are at higher risk of anesthetic overdose and other anesthesia-related complications. Which clients does this include? (Select all that apply.) a. A 75-year-old client scheduled for an elective procedure b. Client who drinks a 6-pack of beer each day c. Client with a serum creatinine of 3.8 mg/dL d. Client who is taking birth control pills e. Young male client with a RYR1 gene mutation People at higher risk for anesthetic overdose or other anesthesia-related complications include people with a slowed metabolism (older adults generally have slower metabolism than younger adults), those with kidney or liver impairments, and those with mutations of the RYR1 gene. Drinking a 6-pack of beer per day possibly indicates some liver disease; a creatinine of 3.8 is high, indicating renal disease; and the genetic mutation increases the chance of malignant hyperthermia. Taking birth control pills is not a risk factor. 4. A client is having shoulder surgery with regional anesthesia. What actions by the nurse are most important to enhance client safety related to this anesthesia? (Select all that apply.) a. Assessing distal circulation to the operative arm after positioning b. Keeping the client warm during the operative procedure c. Padding the client’s shoulder and arm on the operating table d. Preparing to suction the client’s airway if the client vomits e. Speaking in a low, quiet voice as anesthesia is administered After regional anesthesia is administered, the client loses all sensation distally. The nurse ensures client safety by assessing distal circulation and padding the shoulder and arm appropriately. Although awake, the client will not be able to report potential injury. Keeping the client warm is not related to this anesthesia, nor is suctioning or speaking quietly. 5. What actions by the circulating nurse are important to promote client comfort? (Select all that apply.) a. Correct positioning b. Introducing one’s self c. Providing warmth d. Remaining present e. Removing hearing aids The circulating nurse can do many things to promote client comfort, including positioning the client correctly and comfortably, introducing herself or himself to the client, keeping the client warm, and remaining present with the client. Removing hearing aids does not promote comfort and, if the client is still awake when they are removed, may contribute to disorientation and anxiety. 1. A client has developed malignant hyperthermia. The client weighs 136 pounds. What is the safe dose range for one dose of dantrolene sodium (Dantrium)? (Enter your answer using whole numbers, separated by a hyphen with no spaces.) mg 124-186 mg The dose of dantrolene is 2 to 3 mg/kg. The client weighs 62 kg, so the safe dose range is 124 to 186 mg. Chapter 27: Assessment of the Respiratory System 1. A nurse obtains the health history of a client who is recently diagnosed with lung cancer and identifies that the client has a 60–pack-year smoking history. Which action is most important for the nurse to take when interviewing this client? a. Tell the client that he needs to quit smoking to stop further cancer development. b. Encourage the client to be completely honest about both tobacco and marijuana use. c. Maintain a nonjudgmental attitude to avoid causing the client to feel guilty. d. Avoid giving the client false hope regarding cancer treatment and prognosis. Smoking history includes the use of cigarettes, cigars, pipe tobacco, marijuana, and other controlled substances. Because the client may have guilt or denial about this habit, assume a nonjudgmental attitude during the interview. This will encourage the client to be honest about the exposure. Ask the client whether any of these substances are used now or were used in the past. Assess whether the client has passive exposure to smoke in the home or workplace. If the client smokes, ask for how long, how many packs per day, and whether he or she has quit smoking (and how long ago). 2. A nurse assesses a client after an open lung biopsy. Which assessment finding is matched with the correct intervention? a. Client states he is dizzy. – Nurse applies oxygen and pulse oximetry. b. Client’s heart rate is 55 beats/min. – Nurse withholds pain medication. c. Client has reduced breath sounds. – Nurse calls physician immediately. d. Client’s respiratory rate is 18 breaths/min. – Nurse decreases oxygen flow rate. A potentially serious complication after biopsy is pneumothorax, which is indicated by decreased or absent breath sounds. The physician needs to be notified immediately. Dizziness after the procedure is not an expected finding. If the client’s heart rate is 55 beats/min, no reason is known to withhold pain medication. A respiratory rate of 18 breaths/min is a normal finding and would not warrant changing the oxygen flow rate. 3. A nurse assesses a client’s respiratory status. Which information is of highest priority for the nurse to obtain? a. Average daily fluid intake b. Neck circumference c. Height and weight d. Occupation and hobbies Many respiratory problems occur as a result of chronic exposure to inhalation irritants used in a client’s occupation and hobbies. Although it will be important for the nurse to assess the client’s fluid intake, height, and weight, these will not be as important as determining his occupation and hobbies. Determining the client’s neck circumference will not be an important part of a respiratory assessment. 4. A nurse is caring for an older adult client who has a pulmonary infection. Which action should the nurse take first? a. Encourage the client to increase fluid intake. b. Assess the client’s level of consciousness. c. Raise the head of the bed to at least 45 degrees. d. Provide the client with humidified oxygen. Assessing the client’s level of consciousness will be most important because it will show how the client is responding to the presence of the infection. Although it will be important for the nurse to encourage the client to turn, cough, and frequently breathe deeply; raise the head of the bed; increase oral fluid intake; and humidify the oxygen administered, none of these actions will be as important as assessing the level of consciousness. 5. A nurse is providing care after auscultating clients’ breath sounds. Which assessment finding is correctly matched to the nurse’s primary intervention? a. Hollow sounds are heard over the trachea. – The nurse increases the oxygen flow rate. b. Crackles are heard in bases. – The nurse encourages the client to cough forcefully. c. Wheezes are heard in central areas. – The nurse administers an inhaled bronchodilator. d. Vesicular sounds are heard over the periphery. – The nurse has the client breathe deeply. Wheezes are indicative of narrowed airways, and bronchodilators help to open the air passages. Hollow sounds are typically heard over the trachea, and no intervention is necessary. If crackles are heard, the client may need a diuretic. Crackles represent a deep interstitial process, and coughing forcefully will not help the client expectorate secretions. Vesicular sounds heard in the periphery are normal and require no intervention. 6. A nurse observes that a client’s anteroposterior (AP) chest diameter is the same as the lateral chest diameter. Which question should the nurse ask the client in response to this finding? a. “Are you taking any medications or herbal supplements?” b. “Do you have any chronic breathing problems?” c. “How often do you perform aerobic exercise?” d. “What is your occupation and what are your hobbies?” The normal chest has a lateral diameter that is twice as large as the AP diameter. When the AP diameter approaches or exceeds the lateral diameter, the client is said to have a barrel chest. Most commonly, barrel chest occurs as a result of a long-term chronic airflow limitation problem, such as chronic obstructive pulmonary disease or severe chronic asthma. It can also be seen in people who have lived at a high altitude for many years. Therefore, an AP chest diameter that is the same as the lateral chest diameter should be rechecked but is not as indicative of underlying disease processes as an AP diameter that exceeds the lateral diameter. Medications, herbal supplements, and aerobic exercise are not associated with a barrel chest. Although occupation and hobbies may expose a client to irritants that can cause chronic lung disorders and barrel chest, asking about chronic breathing problems is more direct and should be asked first. 7. A nurse is assessing a client who is recovering from a lung biopsy. Which assessment finding requires immediate action? a. Increased temperature b. Absent breath sounds c. Productive cough d. Incisional discomfort Absent breath sounds may indicate that the client has a pneumothorax, a serious complication after a needle biopsy or open lung biopsy. The other manifestations are not life threatening. 8. A nurse is caring for a client who is scheduled to undergo a thoracentesis. Which intervention should the nurse complete prior to the procedure? a. Measure oxygen saturation before and after a 12-minute walk. b. Verify that the client understands all possible complications. c. Explain the procedure in detail to the client and the family. d. Validate that informed consent has been given by the client. A thoracentesis is an invasive procedure with many potentially serious complications. Verifying that the client understands complications and explaining the procedure to be performed will be done by the physician or nurse practitioner, not the nurse. Measurement of oxygen saturation before and after a 12-minute walk is not a procedure unique to a thoracentesis. 9. A nurse assesses a client after a thoracentesis. Which assessment finding warrants immediate action? a. The client rates pain as a 5/10 at the site of the procedure. b. A small amount of drainage from the site is noted. c. Pulse oximetry is 93% on 2 liters of oxygen. d. The trachea is deviated toward the opposite side of the neck. A deviated trachea is a manifestation of a tension pneumothorax, which is a medical emergency. The other findings are normal or near normal. 10. A nurse cares for a client who had a bronchoscopy 2 hours ago. The client asks for a drink of water. Which action should the nurse take next? a. Call the physician and request a prescription for food and water. b. Provide the client with ice chips instead of a drink of water. c. Assess the client’s gag reflex before giving any food or water. d. Let the client have a small sip to see whether he or she can swallow. The topical anesthetic used during the procedure will have affected the client’s gag reflex. Before allowing the client anything to eat or drink, the nurse must check for the return of this reflex. 11. A nurse plans care for a client who is experiencing dyspnea and must stop multiple times when climbing a flight of stairs. Which intervention should the nurse include in this client’s plan of care? a. Assistance with activities of daily living b. Physical therapy activities every day c. Oxygen therapy at 2 liters per nasal cannula d. Complete bedrest with frequent repositioning A client with dyspnea and difficulty completing activities such as climbing a flight of stairs has class III dyspnea. The nurse should provide assistance with activities of daily living. These clients should be encouraged to participate in activities as tolerated. They should not be on complete bedrest, may not be able to tolerate daily physical therapy, and only need oxygen if hypoxia is present. 12. A nurse teaches a client who is prescribed nicotine replacement therapy. Which statement should the nurse include in this client’s teaching? a. “Make a list of reasons why smoking is a bad habit.” b. “Rise slowly when getting out of bed in the morning.” c. “Smoking while taking this medication will increase your risk of a stroke.” d. “Stopping this medication suddenly increases your risk for a heart attack.” Clients who smoke while using drugs for nicotine replacement therapy increase the risk of stroke and heart attack. Nurses should teach clients not to smoke while taking this drug. The other responses are inappropriate. 13. A nurse is caring for a client who received benzocaine spray prior to a recent bronchoscopy. The client presents with continuous cyanosis even with oxygen therapy. Which action should the nurse take next? a. Administer an albuterol treatment. b. Notify the Rapid Response Team. c. Assess the client’s peripheral pulses. d. Obtain blood and sputum cultures. Cyanosis unresponsive to oxygen therapy is a manifestation of methemoglobinemia, which is an adverse effect of benzocaine spray. Death can occur if the level of methemoglobin rises and cyanosis occurs. The nurse should notify the Rapid Response Team to provide advanced nursing care. 14. A nurse auscultates a harsh hollow sound over a client’s trachea and larynx. Which action should the nurse take first? a. Document the findings. b. Administer oxygen therapy. c. Position the client in high-Fowler’s position. d. Administer prescribed albuterol. Bronchial breath sounds, including harsh, hollow, tubular, and blowing sounds, are a normal finding over the trachea and larynx. The nurse should document this finding. There is no need to implement oxygen therapy, administer albuterol, or change the client’s position because the finding is normal. 1. A nurse assesses a client who is prescribed varenicline (Chantix) for smoking cessation. Which manifestations should the nurse identify as adverse effects of this medication? (Select all that apply.) a. Visual hallucinations b. Tachycardia c. Decreased cravings d. Impaired judgment e. Increased thirst Varenicline (Chantix) has a black box warning stating that the drug can cause manic behavior and hallucinations. The nurse should assess for changes in behavior and thought processes, including impaired judgment and visual hallucinations. Tachycardia and increased thirst are not adverse effects of this medication. Decreased cravings is a therapeutic response to this medication. 2. A nurse plans care for a client who is at high risk for a pulmonary infection. Which interventions should the nurse include in this client’s plan of care? (Select all that apply.) a. Encourage deep breathing and coughing. b. Implement an air mattress overlay. c. Ambulate the client three times each day. d. Provide a diet high in protein and vitamins. e. Administer acetaminophen (Tylenol) twice daily. ANS: A, C, D Regular pulmonary hygiene and activities to maintain health and fitness help to maximize functioning of the respiratory system and prevent infection. A client at high risk for a pulmonary infection may need a specialty bed to help with postural drainage or percussion; this would not include an air mattress overlay, which is used to prevent pressure ulcers. Tylenol would not decrease the risk of a pulmonary infection. 3. While obtaining a client’s health history, the client states, “I am allergic to avocados.” Which responses by the nurse are best? (Select all that apply.) a. “What response do you have when you eat avocados?” b. “I will remove any avocados that are on your lunch tray.” c. “When was the last time you ate foods containing avocados?” d. “I will document this in your record so all of your providers will know.” e. “Have you ever been treated for this allergic reaction?” Nurses should assess clients who have allergies for the specific cause, treatment, and response to treatment. The nurse should also document the allergies in a prominent place in the client’s medical record. The nurse should collaborate with food services to ensure no avocados are placed on the client’s meal trays. Asking about the last time the client ate avocados does not provide any pertinent information for the client’s plan of care. 4. A nurse collaborates with a respiratory therapist to complete pulmonary function tests (PFTs) for a client. Which statements should the nurse include in communications with the respiratory therapist prior to the tests? (Select all that apply.) a. “I held the client’s morning bronchodilator medication.” b. “The client is ready to go down to radiology for this examination.” c. “Physical therapy states the client can run on a treadmill.” d. “I advised the client not to smoke for 6 hours prior to the test.” e. “The client is alert and can follow your commands.” To ensure the PFTs are accurate, the therapist needs to know that no bronchodilators have been administered in the past 4 to 6 hours, the client did not smoke within 6 to 8 hours prior to the test, and the client can follow basic commands, including different breathing maneuvers. The respiratory therapist can perform PFTs at the bedside. A treadmill is not used for this test. 5. A nurse teaches a client who is interested in smoking cessation. Which statements should the nurse include in this client’s teaching? (Select all that apply.) a. “Find an activity that you enjoy and will keep your hands busy.” b. “Keep snacks like potato chips on hand to nibble on.” c. “Identify a punishment for yourself in case you backslide.” d. “Drink at least eight glasses of water each day.” e. “Make a list of reasons you want to stop smoking.” The nurse should teach a client who is interested in smoking cessation to find an activity that keeps the hands busy, to keep healthy snacks on hand to nibble on, to drink at least 8 glasses of water each day, and to make a list of reasons for quitting smoking. The nurse should also encourage the client not to be upset if he or she backslides and has a cigarette. 1. A nurse assesses a 66-year-old client who is attempting to quit smoking. The client states, “I started smoking at age 16, and smoked one pack each day until 10 years ago. Then I decreased to a half of a pack per day.” How many pack-years should the nurse document for this client? (Record your answer using a whole number.) pack-years 45 pack-years 66 (current age) – 16 (year started smoking) = 50 years of smoking. (40 years ´ 1 pack per day) + (10 years ´ 0.5 pack per day) = 45 pack-years. Chapter 32: Care of Critically Ill Patients with Respiratory Problems 1.A nurse answers a call light and finds a client anxious, short of breath, reporting chest pain, and having a blood pressure of 88/52 mm Hg on the cardiac monitor. What action by the nurse takes priority? a. Assess the client’s lung sounds. b. Notify the Rapid Response Team. c. Provide reassurance to the client. d. Take a full set of vital signs. This client has manifestations of a pulmonary embolism, and the most critical action is to notify the Rapid Response Team for speedy diagnosis and treatment. The other actions are appropriate also but are not the priority. 2.A client is admitted with a pulmonary embolism (PE). The client is young, healthy, and active and has no known risk factors for PE. What action by the nurse is most appropriate? a. Encourage the client to walk 5 minutes each hour. b . Refer the client to smoking cessation classes. c. Teach the client about factor V Leiden testing. d Tell the client that sometimes no cause for disease is . found. Factor V Leiden is an inherited thrombophilia that can lead to abnormal clotting events, including PE. A client with no known risk factors for this disorder should be referred for testing. Encouraging the client to walk is healthy, but is not related to the development of a PE in this case, nor is smoking. Although there are cases of disease where no cause is ever found, this assumption is premature. 3.A client has a pulmonary embolism and is started on oxygen. The student nurse asks why the client’s oxygen saturation has not significantly improved. What response by the nurse is best? a. “Breathing so rapidly interferes with oxygenation.” b . “Maybe the client has respiratory distress syndrome.” c. “The blood clot interferes with perfusion in the lungs.” d “The client needs immediate intubation and mechanical . ventilation.” A large blood clot in the lungs will significantly impair gas exchange and oxygenation. Unless the clot is dissolved, this process will continue unabated. Hyperventilation can interfere with oxygenation by shallow breathing, but there is no evidence that the client is hyperventilating, and this is also not the most precise physiologic answer. Respiratory distress syndrome can occur, but this is not as likely. The client may need to be mechanically ventilated, but without concrete data on FiO2 and SaO2, the nurse cannot make that judgment. 4.A client is on intravenous heparin to treat a pulmonary embolism. The client’s most recent partial thromboplastin time (PTT) was 25 seconds. What order should the nurse anticipate? a. Decrease the heparin rate. b. Increase the heparin rate. c. No change to the heparin rate. d. Stop heparin; start warfarin (Coumadin). For clients on heparin, a PTT of 1.5 to 2.5 times the normal value is needed to demonstrate the heparin is working. A normal PTT is 25 to 35 seconds, so this client’s PTT value is too low. The heparin rate needs to be increased. Warfarin is not indicated in this situation. 5.A client is hospitalized with a second episode of pulmonary embolism (PE). Recent genetic testing reveals the client has an alteration in the gene CYP2C19. What action by the nurse is best? Instruct the client to eliminate all vitamin K from the a. diet. b Prepare preoperative teaching for an inferior vena cava . (IVC) filter. c. Refer the client to a chronic illness support group. d . Teach the client to use a soft-bristled toothbrush. Often clients are discharged from the hospital on warfarin (Coumadin) after a PE. However, clients with a variation in the CYP2C19 gene do not metabolize warfarin well and have higher blood levels and more side effects. This client is a poor candidate for warfarin therapy, and the prescriber will most likely order an IVC filter device to be implanted. The nurse should prepare to do preoperative teaching on this procedure. It would be impossible to eliminate all vitamin K from the diet. A chronic illness support group may be needed, but this is not the best intervention as it is not as specific to the client as the IVC filter. A soft-bristled toothbrush is a safety measure for clients on anticoagulation therapy. 6.A nurse is caring for four clients on intravenous heparin therapy. Which laboratory value possibly indicates that a serious side effect has occurred? a. Hemoglobin: 14.2 g/dL b. Platelet count: 82,000/L c. Red blood cell count: 4.8/mm3 d. White blood cell count: 8.7/mm3 This platelet count is low and could indicate heparin-induced thrombocytopenia. The other values are normal for either gender. 7.A client appears dyspneic, but the oxygen saturation is 97%. What action by the nurse is best? a. Assess for other manifestations of hypoxia. b. Change the sensor on the pulse oximeter. c. Obtain a new oximeter from central supply. d. Tell the client to take slow, deep breaths. Pulse oximetry is not always the most accurate assessment tool for hypoxia as many factors can interfere, producing normal or near-normal readings in the setting of hypoxia. The nurse should conduct a more thorough assessment. The other actions are not appropriate for a hypoxic client. 8.A nurse is assisting the health care provider who is intubating a client. The provider has been attempting to intubate for 40 seconds. What action by the nurse takes priority? a. Ensure the client has adequate sedation. b. Find another provider to intubate. c. Interrupt the procedure to give oxygen. d. Monitor the client’s oxygen saturation. Each intubation attempt should not exceed 30 seconds (15 is preferable) as it causes hypoxia. The nurse should interrupt the intubation attempt and give the client oxygen. The nurse should also have adequate sedation during the procedure and monitor the client’s oxygen saturation, but these do not take priority. Finding another provider is not appropriate at this time. 9.An intubated client’s oxygen saturation has dropped to 88%. What action by the nurse takes priority? a. Determine if the tube is kinked. b. Ensure all connections are patent. c. Listen to the client’s lung sounds. d. Suction the endotracheal tube. When an intubated client shows signs of hypoxia, check for DOPE: displaced tube (most common cause), obstruction (often by secretions), pneumothorax, and equipment problems. The nurse listens for equal, bilateral breath sounds first to determine if the endotracheal tube is still correctly placed. If this assessment is normal, the nurse would follow the mnemonic and assess the patency of the tube and connections and perform suction. 10.A client is on a ventilator and is sedated. What care may the nurse delegate to the unlicensed assistive personnel (UAP)? a. Assess the client for sedation needs. b. Get family permission for restraints. c. Provide frequent oral care per protocol. d. Use nonverbal pain assessment tools. The client on mechanical ventilation needs frequent oral care, which can be delegated to the UAP. The other actions fall within the scope of practice of the nurse. 11.A nurse is caring for a client on mechanical ventilation. When double-checking the ventilator settings with the respiratory therapist, what should the nurse ensure as a priority? a. The client is able to initiate spontaneous breaths. b. The inspired oxygen has adequate humidification. c. The upper peak airway pressure limit alarm is off. d. The upper peak airway pressure limit alarm is on. The upper peak airway pressure limit alarm will sound when the airway pressure reaches a preset maximum. This is critical to prevent damage to the lungs. Alarms should never be turned off. Initiating spontaneous breathing is important for some modes of ventilation but not others. Adequate humidification is important but does not take priority over preventing injury. 12.A nurse is caring for a client on mechanical ventilation and finds the client agitated and thrashing about. What action by the nurse is most appropriate? a. Assess the cause of the agitation. b. Reassure the client that he or she is safe. c. Restrain the client’s hands. d. Sedate the client immediately. The nurse needs to determine the cause of the agitation. The inability to communicate often makes clients anxious, even to the point of panic. Pain and confusion can also cause agitation. Once the nurse determines the cause of the agitation, he or she can implement measures to relieve the underlying cause. Reassurance is also important but may not address the etiology of the agitation. Restraints and more sedation may be necessary, but not as a first step. 13.A nurse is preparing to admit a client on mechanical ventilation from the emergency department. What action by the nurse takes priority? a. Assessing that the ventilator settings are correct b. Ensuring there is a bag-valve-mask in the room c. Obtaining personal protective equipment d. Planning to suction the client upon arrival to the room Having a bag-valve-mask device is critical in case the client needs manual breathing. The respiratory therapist is usually primarily responsible for setting up the ventilator, although the nurse should know and check the settings. Personal protective equipment is important, but ensuring client safety takes priority. The client may or may not need suctioning on arrival. 14.A client is on mechanical ventilation and the client’s spouse wonders why ranitidine (Zantac) is needed since the client “only has lung problems.” What response by the nurse is best? “It will increase the motility of the gastrointestinal a. tract.” b “It will keep the gastrointestinal tract functioning . normally.” “It will prepare the gastrointestinal tract for enteral c. feedings.” d “It will prevent ulcers from the stress of mechanical . ventilation.” Stress ulcers occur in many clients who are receiving mechanical ventilation, and often prophylactic medications are used to prevent them. Frequently used medications include antacids, histamine blockers, and proton pump inhibitors. Zantac is a histamine blocking agent. 15.A client has been brought to the emergency department with a life-threatening chest injury. What action by the nurse takes priority? a. Apply oxygen at 100%. b. Assess the respiratory rate. c. Ensure a patent airway. d. Start two large-bore IV lines. The priority for any chest trauma client is airway, breathing, circulation. The nurse first ensures the client has a patent airway. Assessing respiratory rate and applying oxygen are next, followed by inserting IVs. 16.A client is being discharged soon on warfarin (Coumadin). What menu selection for dinner indicates the client needs more education regarding this medication? a. Hamburger and French fries b. Large chef’s salad and muffin c. No selection; spouse brings pizza d. Tuna salad sandwich and chips Warfarin works by inhibiting the synthesis of vitamin K–dependent clotting factors. Foods high in vitamin K thus interfere with its action and need to be eaten in moderate, consistent amounts. The chef’s salad most likely has too many leafy green vegetables, which contain high amounts of vitamin K. The other selections, while not particularly healthy, will not interfere with the medication’s mechanism of action. 17.A nurse is teaching a client about warfarin (Coumadin). What assessment finding by the nurse indicates a possible barrier to self-management? a. Poor visual acuity b. Strict vegetarian c. Refusal to stop smoking d. Wants weight loss surgery Warfarin works by inhibiting the synthesis of vitamin K–dependent clotting factors. Foods high in vitamin K thus interfere with its action and need to be eaten in moderate, consistent amounts. A vegetarian may have trouble maintaining this diet. The nurse should explore this possibility with the client. The other options are not related. 18.A student nurse is preparing to administer enoxaparin (Lovenox) to a client. What action by the student requires immediate intervention by the supervising nurse? a. Assessing the client’s platelet count b. Choosing an 18-gauge, 2-inch needle c. Not aspirating prior to injection d. Swabbing the injection site with alcohol Enoxaparin is given subcutaneously, so the 18-gauge, 2-inch needle is too big. The other actions are appropriate. 19.A client in the emergency department has several broken ribs. What care measure will best promote comfort? a. Allowing the client to choose the position in bed b. Humidifying the supplemental oxygen c. Offering frequent, small drinks of water d. Providing warmed blankets Allow the client with respiratory problems to assume a position of comfort if it does not interfere with care. Often the client will choose a more upright position, which also improves oxygenation. The other options are less effective comfort measures. 20.A client has been diagnosed with a very large pulmonary embolism (PE) and has a dropping blood pressure. What medication should the nurse anticipate the client will need as the priority? a. Alteplase (Activase) b. Enoxaparin (Lovenox) c. Unfractionated heparin d. Warfarin sodium (Coumadin) Activase is a “clot-busting” agent indicated in large PEs in the setting of hemodynamic instability. The nurse knows this drug is the priority, although heparin may be started initially. Enoxaparin and warfarin are not indicated in this setting. 21.A client is brought to the emergency department after sustaining injuries in a severe car crash. The client’s chest wall does not appear to be moving normally with respirations, oxygen saturation is 82%, and the client is cyanotic. What action by the nurse is the priority? a. Administer oxygen and reassess. b. Auscultate the client’s lung sounds. c. Facilitate a portable chest x-ray. d. Prepare to assist with intubation. This client has manifestations of flail chest and, with the other signs, needs to be intubated and mechanically ventilated immediately. The nurse does not have time to administer oxygen and wait to reassess, or to listen to lung sounds. A chest x-ray will be taken after the client is intubated. 22.A student nurse asks for an explanation of “refractory hypoxemia.” What answer by the nurse instructor is best? “It is chronic hypoxemia that accompanies restrictive a. airway disease.” b “It is hypoxemia from lung damage due to mechanical . ventilation.” “It is hypoxemia that continues even after the client is c. weaned from oxygen.” d “It is hypoxemia that persists even with 100% oxygen . administration.” Refractory hypoxemia is hypoxemia that persists even with the administration of 100% oxygen. It is a cardinal sign of acute respiratory distress syndrome. It does not accompany restrictive airway disease and is not caused by the use of mechanical ventilation or by being weaned from oxygen. 23.A nurse is caring for a client on the medical stepdown unit. The following data are related to this client: Subjective Information Shortness of breath for 20 minutes Feels frightened “Can’t catch my breath” Laboratory Analysis pH: 7.12 PaCO2: 28 mm Hg PaO2: 58 mm Hg SaO2: 88% Physical Assessment Pulse: 120 beats/min Respiratory rate: 34 breaths/min Blood pressure 158/92 mm Hg Lungs have crackles What action by the nurse is most appropriate? a. Call respiratory therapy for a breathing treatment. b. Facilitate a STAT pulmonary angiography. c. Prepare for immediate endotracheal intubation. d. Prepare to administer intravenous anticoagulants. This client has manifestations of pulmonary embolism (PE); however, many conditions can cause the client’s presentation. The gold standard for diagnosing a PE is pulmonary angiography. The nurse should facilitate this test as soon as possible. The client does not have wheezing, so a respiratory treatment is not needed. The client is not unstable enough to need intubation and mechanical ventilation. IV anticoagulants are not given without a diagnosis of PE. 1.A nurse is caring for five clients. For which clients would the nurse assess a high risk for developing a pulmonary embolism (PE)? (Select all that apply.) a. Client who had a reaction to contrast dye yesterday b. Client with a new spinal cord injury on a rotating bed c. Middle-aged man with an exacerbation of asthma d. Older client who is 1-day post hip replacement surgery e. Young obese client with a fractured femur Conditions that place clients at higher risk of developing PE include prolonged immobility, central venous catheters, surgery, obesity, advancing age, conditions that increase blood clotting, history of thromboembolism, smoking, pregnancy, estrogen therapy, heart failure, stroke, cancer (particularly lung or prostate), and trauma. A contrast dye reaction and asthma pose no risk for PE. 2.When working with women who are taking hormonal birth control, what health promotion measures should the nurse teach to prevent possible pulmonary embolism (PE)? (Select all that apply.) a. Avoid drinking alcohol. b. Eat more omega-3 fatty acids. c. Exercise on a regular basis. d. Maintain a healthy weight. e. Stop smoking cigarettes. Health promotion measures for clients to prevent thromboembolic events such as PE include maintaining a healthy weight, exercising on a regular basis, and not smoking. Avoiding alcohol and eating more foods containing omega-3 fatty acids are heart-healthy actions but do not relate to the prevention of PE. 3.A client with a new pulmonary embolism (PE) is anxious. What nursing actions are most appropriate? (Select all that apply.) a. Acknowledge the frightening nature of the illness. b Delegate a back rub to the unlicensed assistive . personnel (UAP). c. Give simple explanations of what is happening. d . Request a prescription for antianxiety medication. e. Stay with the client and speak in a quiet, calm voice. Clients with PEs are often anxious. The nurse can acknowledge the client’s fears, delegate comfort measures, give simple explanations the client will understand, and stay with the client. Using a calm, quiet voice is also reassuring. Sedatives and antianxiety medications are not used routinely because they can contribute to hypoxia. If the client’s anxiety is interfering with diagnostic testing or treatment, they can be used, but there is no evidence that this is the case. 4.The nurse caring for mechanically ventilated clients uses best practices to prevent ventilator-associated pneumonia. What actions are included in this practice? (Select all that apply.) a. Adherence to proper hand hygiene b. Administering anti-ulcer medication c. Elevating the head of the bed d. Providing oral care per protocol e. Suctioning the client on a regular schedule The “ventilator bundle” is a group of care measures to prevent ventilator-associated pneumonia. Actions in the bundle include using proper hand hygiene, giving anti-ulcer medications, elevating the head of the bed, providing frequent oral care per policy, preventing aspiration, and providing pulmonary hygiene measures. Suctioning is done as needed. 5.A nurse is caring for a client who is on mechanical ventilation. What actions will promote comfort in this client? (Select all that apply.) a. Allow visitors at the client’s bedside. b. Ensure the client can communicate if awake. c. Keep the television tuned to a favorite channel. d. Provide back and hand massages when turning. e. Turn the client every 2 hours or more. ANS: A, B, D, E There are many basic care measures that can be employed for the client who is on a ventilator. Allowing visitation, providing a means of communication, massaging the client’s skin, and routinely turning and repositioning the client are some of them. Keeping the TV on will interfere with sleep and rest. 6.The nurse caring for mechanically ventilated clients knows that older adults are at higher risk for weaning failure. What age-related changes contribute to this? (Select all that apply.) a. Chest wall stiffness b. Decreased muscle strength c. Inability to cooperate d. Less lung elasticity e. Poor vision and hearing Age-related changes that increase the difficulty of weaning older adults from mechanical ventilation include increased stiffness of the chest wall, decreased muscle strength, and less elasticity of lung tissue. Not all older adults have an inability to cooperate or poor sensory acuity. 1.A 242-pound client is being mechanically ventilated. To prevent lung injury, what setting should the nurse anticipate for tidal volume? (Record your answer using a whole number.) mL 660 mL A low tidal volume of 6 mL/kg is used to prevent lung injury. 242 pounds = 110 kg. 110 kg × 6 mL/kg = 660 mL. Chapter 33: Assessment of the Cardiovascular System 1. A nurse assesses a client who had a myocardial infarction and is hypotensive. Which additional assessment finding should the nurse expect? a. Heart rate of 120 beats/min b. Cool, clammy skin c. Oxygen saturation of 90% d. Respiratory rate of 8 breaths/min When a client experiences hypotension, baroreceptors in the aortic arch sense a pressure decrease in the vessels. The parasympathetic system responds by lessening the inhibitory effect on the sinoatrial node. This results in an increase in heart rate and respiratory rate. This tachycardia is an early response and is seen even when blood pressure is not critically low. An increased heart rate and respiratory rate will compensate for the low blood pressure and maintain oxygen saturations and perfusion. The client may not be able to compensate for long, and decreased oxygenation and cool, clammy skin will occur later. 2. A nurse assesses a client after administering a prescribed beta blocker. Which assessment should the nurse expect to find? a. Blood pressure increased from 98/42 mm Hg to 132/60 mm Hg b. Respiratory rate decreased from 25 breaths/min to 14 breaths/min c. Oxygen saturation increased from 88% to 96% d. Pulse decreased from 100 beats/min to 80 beats/min Beta blockers block the stimulation of beta1-adrenergic receptors. They block the sympathetic (fight-or-flight) response and decrease the heart rate (HR). The beta blocker will decrease HR and blood pressure, increasing ventricular filling time. It usually does not have effects on beta2-adrenergic receptor sites. Cardiac output will drop because of decreased HR. 3. A nurse assesses clients on a medical-surgical unit. Which client should the nurse identify as having the greatest risk for cardiovascular disease? a. An 86-year-old man with a history of asthma b. A 32-year-old Asian-American man with colorectal cancer c. A 45-year-old American Indian woman with diabetes mellitus d. A 53-year-old postmenopausal woman who is on hormone therapy The incidence of coronary artery disease and hypertension is higher in American Indians than in whites or Asian Americans. Diabetes mellitus increases the risk for hypertension and coronary artery disease in people of any race or ethnicity. Asthma, colorectal cancer, and hormone therapy do not increase risk for cardiovascular disease. 4. A nurse assesses an older adult client who has multiple chronic diseases. The client’s heart rate is 48 beats/min. Which action should the nurse take first? a. Document the finding in the chart. b. Initiate external pacing. c. Assess the client’s medications. d. Administer 1 mg of atropine. Pacemaker cells in the conduction system decrease in number as a person ages, resulting in bradycardia. The nurse should check the medication reconciliation for medications that might cause such a drop in heart rate, then should inform the health care provider. Documentation is important, but it is not the priority action. The heart rate is not low enough for atropine or an external pacemaker to be needed. 5. An emergency room nurse obtains the health history of a client. Which statement by the client should alert the nurse to the occurrence of heart failure? a. “I get short of breath when I climb stairs.” b. “I see halos floating around my head.” c. “I have trouble remembering things.” d. “I have lost weight over the past month.” Dyspnea on exertion is an early manifestation of heart failure and is associated with an activity such as stair climbing. The other findings are not specific to early occurrence of heart failure. 6. A nurse obtains the health history of a client who is newly admitted to the medical unit. Which statement by the client should alert the nurse to the presence of edema? a. “I wake up to go to the bathroom at night.” b. “My shoes fit tighter by the end of the day.” c. “I seem to be feeling more anxious lately.” d. “I drink at least eight glasses of water a day.” Weight gain can result from fluid accumulation in the interstitial spaces. This is known as edema. The nurse should note whether the client feels that his or her shoes or rings are tight, and should observe, when present, an indentation around the leg where the socks end. The other answers do not describe edema. 7. A nurse assesses an older adult client who is experiencing a myocardial infarction. Which clinical manifestation should the nurse expect? a. Excruciating pain on inspiration b. Left lateral chest wall pain c. Disorientation and confusion d. Numbness and tingling of the arm In older adults, disorientation or confusion may be the major manifestation of myocardial infarction caused by poor cardiac output. Pain manifestations and numbness and tingling of the arm could also be related to the myocardial infarction. However, the nurse should be more concerned about the new onset of disorientation or confusion caused by decreased perfusion. 8. A nurse assesses a client 2 hours after a cardiac angiography via the left femoral artery. The nurse notes that the left pedal pulse is weak. Which action should the nurse take? a. Elevate the leg and apply a sandbag to the entrance site. b. Increase the flow rate of intravenous fluids. c. Assess the color and temperature of the left leg. d. Document the finding as “left pedal pulse of +1/4.” Loss of a pulse distal to an angiography entry site is serious, indicating a possible arterial obstruction. The pulse may be faint because of edema. The left pulse should be compared with the right, and pulses should be compared with previous assessments, especially before the procedure. Assessing color (pale, cyanosis) and temperature (cool, cold) will identify a decrease in circulation. Once all peripheral and vascular assessment data are acquired, the primary health care provider should be notified. Simply documenting the findings is inappropriate. The leg should be positioned below the level of the heart or dangling to increase blood flow to the distal portion of the leg. Increasing intravenous fluids will not address the client’s problem. 9. A nurse assesses a client who is recovering after a left-sided cardiac catheterization. Which assessment finding requires immediate intervention? a. Urinary output less than intake b. Bruising at the insertion site c. Slurred speech and confusion d. Discomfort in the left leg A left-sided cardiac catheterization specifically increases the risk for a cerebral vascular accident. A change in neurologic status needs to be acted on immediately. Discomfort and bruising are expected at the site. If intake decreases, a client can become dehydrated because of dye excretion. The second intervention would be to increase the client’s fluid status. Neurologic changes would take priority. 10. A nurse assesses a client who is scheduled for a cardiac catheterization. Which assessment should the nurse complete prior to this procedure? a. Client’s level of anxiety b. Ability to turn self in bed c. Cardiac rhythm and heart rate d. Allergies to iodine-based agents Before the procedure, the nurse should ascertain whether the client has an allergy to iodine-containing preparations, such as seafood or local anesthetics. The contrast medium used during the procedure is iodine based. This allergy can cause a life-threatening reaction, so it is a high priority. Second, it is important for the nurse to assess anxiety, mobility, and baseline cardiac status. 11. A nurse cares for a client who is prescribed magnetic resonance imaging (MRI) of the heart. The client’s health history includes a previous myocardial infarction and pacemaker implantation. Which action should the nurse take? a. Schedule an electrocardiogram just before the MRI. b. Notify the health care provider before scheduling the MRI. c. Call the physician and request a laboratory draw for cardiac enzymes. d. Instruct the client to increase fluid intake the day before the MRI. The magnetic fields of the MRI can deactivate the pacemaker. The nurse should call the health care provider and report that the client has a pacemaker so the provider can order other diagnostic tests. The client does not need an electrocardiogram, cardiac enzymes, or increased fluids. 12. A nurse assesses a client who is recovering from a myocardial infarction. The client’s pulmonary artery pressure reading is 25/12 mm Hg. Which action should the nurse take first? a. Compare the results with previous pulmonary artery pressure readings. b. Increase the intravenous fluid rate because these readings are low. c. Immediately notify the health care provider of the elevated pressures. d. Document the finding in the client’s chart as the only action. Normal pulmonary artery pressures range from 15 to 26 mm Hg for systolic and from 5 to 15 mm Hg for diastolic. Although this client’s readings are within normal limits, the nurse needs to assess any trends that may indicate a need for medical treatment to prevent complications. There is no need to increase intravenous fluids or notify the provider. 13. A nurse cares for a client who has an 80% blockage of the right coronary artery (RCA) and is scheduled for bypass surgery. Which intervention should the nurse be prepared to implement while this client waits for surgery? a. Administration of IV furosemide (Lasix) b. Initiation of an external pacemaker c. Assistance with endotracheal intubation d. Placement of central venous access The RCA supplies the right atrium, the right ventricle, the inferior portion of the left ventricle, and the atrioventricular (AV) node. It also supplies the sinoatrial node in 50% of people. If the client totally occludes the RCA, the AV node would not function and the client would go into heart block, so emergency pacing should be available for the client. Furosemide, intubation, and central venous access will not address the primary complication of RCA occlusion, which is AV node malfunction. 14. A nurse teaches a client with diabetes mellitus and a body mass index of 42 who is at high risk for coronary artery disease. Which statement related to nutrition should the nurse include in this client’s teaching? a. “The best way to lose weight is a high-protein, low-carbohydrate diet.” b. “You should balance weight loss with consuming necessary nutrients.” c. “A nutritionist will provide you with information about your new diet.” d. “If you exercise more frequently, you won’t need to change your diet.” Clients at risk for cardiovascular diseases should follow the American Heart Association guidelines to combat obesity and improve cardiac health. The nurse should encourage the client to eat vegetables, fruits, unrefined whole-grain products, and fat-free dairy products while losing weight. High-protein food items are often high in fat and calories. Although the nutritionist can assist with client education, the nurse should include nutrition education and assist the client to make healthy decisions. Exercising and eating nutrient-rich foods are both important components in reducing cardiovascular risk. 15. A nurse cares for a client who has advanced cardiac disease and states, “I am having trouble sleeping at night.” How should the nurse respond? a. “I will consult the provider to prescribe a sleep study to determine the problem.” b. “You become hypoxic while sleeping; oxygen therapy via nasal cannula will help.” c. “A continuous positive airway pressure, or CPAP, breathing mask will help you breathe at night.” d. “Use pillows to elevate your head and chest while you are sleeping.” The client is experiencing orthopnea (shortness of breath while lying flat). The nurse should teach the client to elevate the head and chest with pillows or sleep in a recliner. A sleep study is not necessary to diagnose this client. Oxygen and CPAP will not help a client with orthopnea. 16. A nurse cares for a client who is recovering from a myocardial infarction. The client states, “I will need to stop eating so much chili to keep that indigestion pain from returning.” How should the nurse respond? a. “Chili is high in fat and calories; it would be a good idea to stop eating it.” b. “The provider has prescribed an antacid for you to take every morning.” c. “What do you understand about what happened to you?” d. “When did you start experiencing this indigestion?” Clients who experience myocardial infarction often respond with denial, which is a defense mechanism. The nurse should ask the client what he or she thinks happened, or what the illness means to him or her. The other responses do not address the client’s misconception about recent pain and the cause of that pain. 17. A nurse prepares a client for coronary artery bypass graft surgery. The client states, “I am afraid I might die.” How should the nurse respond? a. “This is a routine surgery and the risk of death is very low.” b. “Would you like to speak with a chaplain prior to surgery?” c. “Tell me more about your concerns about the surgery.” d. “What support systems do you have to assist you?” The nurse should discuss the client’s feelings and concerns related to the surgery. The nurse should not provide false hope or push the client’s concerns off on the chaplain. The nurse should address support systems after addressing the client’s current issue. 18. An emergency department nurse triages clients who present with chest discomfort. Which client should the nurse plan to assess first? a. A 42-year-old female who describes her pain as a dull ache with numbness in her fingers b. A 49-year-old male who reports moderate pain that is worse on inspiration c. A 53-year-old female who reports substernal pain that radiates to her abdomen d. A 58-year-old male who describes his pain as intense stabbing that spreads across his chest All clients who have chest pain should be assessed more thoroughly. To determine which client should be seen first, the nurse must understand common differences in pain descriptions. Intense stabbing, vise-like substernal pain that spreads through the client’s chest, arms, jaw, back, or neck is indicative of a myocardial infarction. The nurse should plan to see this client first to prevent cardiac cell death. A dull ache with numbness in the fingers is consistent with anxiety. Pain that gets worse with inspiration is usually related to a pleuropulmonary problem. Pain that spreads to the abdomen is often associated with an esophageal-gastric problem, especially when this pain is experienced by a male client. Female clients may experience abdominal discomfort with a myocardial event. Although clients with anxiety, pleuropulmonary, and esophageal-gastric problems should be seen, they are not a higher priority than myocardial infarction. 19. A nurse auscultated heart tones on an older adult client. Which action should the nurse take based on heart tones heard? a. Administer a diuretic. b. Document the finding. c. Decrease the IV flow rate. d. Evaluate the client’s medications. The sound heard is an atrial gallop S4. An atrial gallop may be heard in older clients because of a stiffened ventricle. The nurse should document the finding, but no other intervention is needed at this time. 20. A nurse assesses a client who has aortic regurgitation. In which location in the illustration shown below should the nurse auscultate to best hear a cardiac murmur related to aortic regurgitation? a. Location A b. Location B c. Location C d. Location D The aortic valve is auscultated in the second intercostal space just to the right of the sternum. 1. A nurse is caring for a client with a history of renal insufficiency who is scheduled for a cardiac catheterization. Which actions should the nurse take prior to the catheterization? (Select all that apply.) a. Assess for allergies to iodine. b. Administer intravenous fluids. c. Assess blood urea nitrogen (BUN) and creatinine results. d. Insert a Foley catheter. e. Administer a prophylactic antibiotic. f. Insert a central venous catheter. If the client has kidney disease (as indicated by BUN and creatinine results), fluids and Mucomyst may be given 12 to 24 hours before the procedure for renal protection. The client should be assessed for allergies to iodine, including shellfish; the contrast medium used during the catheterization contains iodine. A Foley catheter and central venous catheter are not required for the procedure and would only increase the client’s risk for infection. Prophylactic antibiotics are not administered prior to a cardiac catheterization. 2. An emergency room nurse assesses a female client. Which assessment findings should alert the nurse to request a prescription for an electrocardiogram? (Select all that apply.) a. Hypertension b. Fatigue despite adequate rest c. Indigestion d. Abdominal pain e. Shortness of breath Women may not have chest pain with myocardial infarction, but may feel discomfort or indigestion. They often present with a triad of symptoms—indigestion or feeling of abdominal fullness, feeling of chronic fatigue despite adequate rest, and feeling unable to catch their breath. Frequently, women are not diagnosed and therefore are not treated adequately. Hypertension and abdominal pain are not associated with acute coronary syndrome. 3. A nurse assesses a client who is recovering after a coronary catheterization. Which assessment findings in the first few hours after the procedure require immediate action by the nurse? (Select all that apply.) a. Blood pressure of 140/88 mm Hg b. Serum potassium of 2.9 mEq/L c. Warmth and redness at the site d. Expanding groin hematoma e. Rhythm changes on the cardiac monitor In the first few hours postprocedure, the nurse monitors for complications such as bleeding from the insertion site, hypotension, acute closure of the vessel, dye reaction, hypokalemia, and dysrhythmias. The client’s blood pressure is slightly elevated but does not need immediate action. Warmth and redness at the site would indicate an infection, but this would not be present in the first few hours. 4. A nurse reviews a client’s laboratory results. Which findings should alert the nurse to the possibility of atherosclerosis? (Select all that apply.) a. Total cholesterol: 280 mg/dL b. High-density lipoprotein cholesterol: 50 mg/dL c. Triglycerides: 200 mg/dL d. Serum albumin: 4 g/dL e. Low-density lipoprotein cholesterol: 160 mg/dL A lipid panel is often used to screen for cardiovascular risk. Total cholesterol, triglycerides, and low-density lipoprotein cholesterol levels are all high, indicating higher risk for cardiovascular disease. 5. A nurse prepares a client for a pharmacologic stress echocardiogram. Which actions should the nurse take when preparing this client for the procedure? (Select all that apply.) a. Assist the provider to place a central venous access device. b. Prepare for continuous blood pressure and pulse monitoring. c. Administer the client’s prescribed beta blocker. d. Give the client nothing by mouth 3 to 6 hours before the procedure. e. Explain to the client that dobutamine will simulate exercise for this examination. Clients receiving a pharmacologic stress echocardiogram will need peripheral venous access and continuous blood pressure and pulse monitoring. The client must be NPO 3 to 6 hours prior to the procedure. Education about dobutamine, which will be administered during the procedure, should be performed. Beta blockers are often held prior to the procedure. 6. A nurse cares for a client who is recovering from a right-sided heart catheterization. For which complications of this procedure should the nurse assess? (Select all that apply.) a. Thrombophlebitis b. Stroke c. Pulmonary embolism d. Myocardial infarction e. Cardiac tamponade Complications from a right-sided heart catheterization include thrombophlebitis, pulmonary embolism, and vagal response. Cardiac tamponade is a risk of both right- and left-sided heart catheterizations. Stroke and myocardial infarction are complications of left-sided heart catheterizations. 1. A nurse prepares a client with acute renal insufficiency for a cardiac catheterization. The provider prescribes 0.9% normal saline to infuse at 125 mL/hr for renal protection. The nurse obtains gravity tubing with a drip rate of 15 drops/mL. At what rate (drops/min) should the nurse infuse the fluids? (Record your answer using a whole number, and rounding to the nearest drop.) drops/min 31 drops/min Chapter 35: Care of Patients with Cardiac Problems 1. A nurse assesses clients on a cardiac unit. Which client should the nurse identify as being at greatest risk for the development of left-sided heart failure? a. A 36-year-old woman with aortic stenosis b. A 42-year-old man with pulmonary hypertension c. A 59-year-old woman who smokes cigarettes daily d. A 70-year-old man who had a cerebral vascular accident Although most people with heart failure will have failure that progresses from left to right, it is possible to have left-sided failure alone for a short period. It is also possible to have heart failure that progresses from right to left. Causes of left ventricular failure include mitral or aortic valve disease, coronary artery disease, and hypertension. Pulmonary hypertension and chronic cigarette smoking are risk factors for right ventricular failure. A cerebral vascular accident does not increase the risk of heart failure. 2. A nurse assesses a client in an outpatient clinic. Which statement alerts the nurse to the possibility of left-sided heart failure? a. “I have been drinking more water than usual.” b. “I am awakened by the need to urinate at night.” c. “I must stop halfway up the stairs to catch my breath.” d. “I have experienced blurred vision on several occasions.” Clients with left-sided heart failure report weakness or fatigue while performing normal activities of daily living, as well as difficulty breathing, or “catching their breath.” This occurs as fluid moves into the alveoli. Nocturia is often seen with right-sided heart failure. Thirst and blurred vision are not related to heart failure. 3. A nurse assesses a client admitted to the cardiac unit. Which statement by the client alerts the nurse to the possibility of right-sided heart failure? a. “I sleep with four pillows at night.” b. “My shoes fit really tight lately.” c. “I wake up coughing every night.” d. “I have trouble catching my breath.” Signs of systemic congestion occur with right-sided heart failure. Fluid is retained, pressure builds in the venous system, and peripheral edema develops. Left-sided heart failure symptoms include respiratory symptoms. Orthopnea, coughing, and difficulty breathing all could be results of left-sided heart failure. 4. While assessing a client on a cardiac unit, a nurse identifies the presence of an S3 gallop. Which action should the nurse take next? a. Assess for symptoms of left-sided heart failure. b. Document this as a normal finding. c. Call the health care provider immediately. d. Transfer the client to the intensive care unit. The presence of an S3 gallop is an early diastolic filling sound indicative of increasing left ventricular pressure and left ventricular failure. The other actions are not warranted. 5. A nurse cares for a client with right-sided heart failure. The client asks, “Why do I need to weigh myself every day?” How should the nurse respond? a. “Weight is the best indication that you are gaining or losing fluid.” b. “Daily weights will help us make sure that you’re eating properly.” c. “The hospital requires that all inpatients be weighed daily.” d. “You need to lose weight to decrease the incidence of heart failure.” Daily weights are needed to document fluid retention or fluid loss. One liter of fluid equals 2.2 pounds. The other responses do not address the importance of monitoring fluid retention or loss. 6. A nurse is teaching a client with heart failure who has been prescribed enalapril (Vasotec). Which statement should the nurse include in this client’s teaching? a. “Avoid using salt substitutes.” b. “Take your medication with food.” c. “Avoid using aspirin-containing products.” d. “Check your pulse daily.” Angiotensin-converting enzyme (ACE) inhibitors such as enalapril inhibit the excretion of potassium. Hyperkalemia can be a life-threatening side effect, and clients should be taught to limit potassium intake. Salt substitutes are composed of potassium chloride. ACE inhibitors do not need to be taken with food and have no impact on the client’s pulse rate. Aspirin is often prescribed in conjunction with ACE inhibitors and is not contraindicated. 7. After administering newly prescribed captopril (Capoten) to a client with heart failure, the nurse implements interventions to decrease complications. Which priority intervention should the nurse implement for this client? a. Provide food to decrease nausea and aid in absorption. b. Instruct the client to ask for assistance when rising from bed. c. Collaborate with unlicensed assistive personnel to bathe the client. d. Monitor potassium levels and check for symptoms of hypokalemia. Administration of the first dose of angiotensin-converting enzyme (ACE) inhibitors is often associated with hypotension, usually termed first-dose effect. The nurse should instruct the client to seek assistance before arising from bed to prevent injury from postural hypotension. ACE inhibitors do not need to be taken with food. Collaboration with unlicensed assistive personnel to provide hygiene is not a priority. The client should be encouraged to complete activities of daily living as independently as possible. The nurse should monitor for hyperkalemia, not hypokalemia, especially if the client has renal insufficiency secondary to heart failure. 8. A nurse assesses a client after administering isosorbide mononitrate (Imdur). The client reports a headache. Which action should the nurse take? a. Initiate oxygen therapy. b. Hold the next dose of Imdur. c. Instruct the client to drink water. d. Administer PRN acetaminophen. The vasodilating effects of isosorbide mononitrate frequently cause clients to have headaches during the initial period of therapy. Clients should be told about this side effect and encouraged to take the medication with food. Some clients obtain relief with mild analgesics, such as acetaminophen. The client’s headache is not related to hypoxia or dehydration; therefore, these interventions would not help. The client needs to take the medication as prescribed to prevent angina; the medication should not be held. 9. A nurse teaches a client who is prescribed digoxin (Lanoxin) therapy. Which statement should the nurse include in this client’s teaching? a. “Avoid taking aspirin or aspirin-containing products.” b. “Increase your intake of foods that are high in potassium.” c. “Hold this medication if your pulse rate is below 80 beats/min.” d. “Do not take this medication within 1 hour of taking an antacid.” Gastrointestinal absorption of digoxin is erratic. Many medications, especially antacids, interfere with its absorption. Clients are taught to hold their digoxin for bradycardia; a heart rate of 80 beats/min is too high for this cutoff. Potassium and aspirin have no impact on digoxin absorption, nor do these statements decrease complications of digoxin therapy. 10. A nurse teaches a client who has a history of heart failure. Which statement should the nurse include in this client’s discharge teaching? a. “Avoid drinking more than 3 quarts of liquids each day.” b. “Eat six small meals daily instead of three larger meals.” c. “When you feel short of breath, take an additional diuretic.” d. “Weigh yourself daily while wearing the same amount of clothing.” Clients with heart failure are instructed to weigh themselves daily to detect worsening heart failure early, and thus avoid complications. Other signs of worsening heart failure include increasing dyspnea, exercise intolerance, cold symptoms, and nocturia. Fluid overload increases symptoms of heart failure. The client should be taught to eat a heart-healthy diet, balance intake and output to prevent dehydration and overload, and take medications as prescribed. The most important discharge teaching is daily weights as this provides the best data related to fluid retention. 11. A nurse admits a client who is experiencing an exacerbation of heart failure. Which action should the nurse take first? a. Assess the client’s respiratory status. b. Draw blood to assess the client’s serum electrolytes. c. Administer intravenous furosemide (Lasix). d. Ask the client about current medications. Assessment of respiratory and oxygenation status is the priority nursing intervention for the prevention of complications. Monitoring electrolytes, administering diuretics, and asking about current medications are important but do not take priority over assessing respiratory status. 12. A nurse assesses a client with mitral valve stenosis. What clinical manifestation should alert the nurse to the possibility that the client’s stenosis has progressed? a. Oxygen saturation of 92% b. Dyspnea on exertion c. Muted systolic murmur d. Upper extremity weakness Dyspnea on exertion develops as the mitral valvular orifice narrows and pressure in the lungs increases. The other manifestations do not relate to the progression of mitral valve stenosis. 13. A nurse cares for a client recovering from prosthetic valve replacement surgery. The client asks, “Why will I need to take anticoagulants for the rest of my life?” How should the nurse respond? a. “The prosthetic valve places you at greater risk for a heart attack.” b. “Blood clots form more easily in artificial replacement valves.” c. “The vein taken from your leg reduces circulation in the leg.” d. “The surgery left a lot of small clots in your heart and lungs.” Synthetic valve prostheses and scar tissue provide surfaces on which platelets can aggregate easily and initiate the formation of blood clots. The other responses are inaccurate. 14. After teaching a client who is being discharged home after mitral valve replacement surgery, the nurse assesses the client’s understanding. Which client statement indicates a need for additional teaching? a. “I’ll be able to carry heavy loads after 6 months of rest.” b. “I will have my teeth cleaned by my dentist in 2 weeks.” c. “I must avoid eating foods high in vitamin K, like spinach.” d. “I must use an electric razor instead of a straight razor to shave.” Clients who have defective or repaired valves are at high risk for endocarditis. The client who has had valve surgery should avoid dental procedures for 6 months because of the risk for endocarditis. When undergoing a mitral valve replacement surgery, the client needs to be placed on anticoagulant therapy to prevent vegetation forming on the new valve. Clients on anticoagulant therapy should be instructed on bleeding precautions, including using an electric razor. If the client is prescribed warfarin, the client should avoid foods high in vitamin K. Clients recovering from open heart valve replacements should not carry anything heavy for 6 months while the chest incision and muscle heal. 15. A nurse cares for a client with infective endocarditis. Which infection control precautions should the nurse use? a. Standard Precautions b. Bleeding precautions c. Reverse isolation d. Contact isolation ANS: A The client with infective endocarditis does not pose any specific threat of transmitting the causative organism. Standard Precautions should be used. Bleeding precautions or reverse or contact isolation is not necessary. 16. A nurse assesses a client with pericarditis. Which assessment finding should the nurse expect to find? a. Heart rate that speeds up and slows down b. Friction rub at the left lower sternal border c. Presence of a regular gallop rhythm d. Coarse crackles in bilateral lung bases The client with pericarditis may present with a pericardial friction rub at the left lower sternal border. This sound is the result of friction from inflamed pericardial layers when they rub together. The other assessments are not related. 17. After teaching a client who is recovering from a heart transplant to change positions slowly, the client asks, “Why is this important?” How should the nurse respond? a. “Rapid position changes can create shear and friction forces, which can tear out your internal vascular sutures.” b. “Your new vascular connections are more sensitive to position changes, leading to increased intravascular pressure and dizziness.” c. “Your new heart is not connected to the nervous system and is unable to respond to decreases in blood pressure caused by position changes.” d. “While your heart is recovering, blood flow is diverted away from the brain, increasing the risk for stroke when you stand up.” Because the new heart is denervated, the baroreceptor and other mechanisms that compensate for blood pressure drops caused by position changes do not function. This allows orthostatic hypotension to persist in the postoperative period. The other options are false statements and do not correctly address the client’s question. 18. A nurse teaches a client recovering from a heart transplant who is prescribed cyclosporine (Sandimmune). Which statement should the nurse include in this client’s discharge teaching? a. “Use a soft-bristled toothbrush and avoid flossing.” b. “Avoid large crowds and people who are sick.” c. “Change positions slowly to avoid hypotension.” d. “Check your heart rate before taking the medication.” These agents cause immune suppression, leaving the client more vulnerable to infection. The medication does not place the client at risk for bleeding, orthostatic hypotension, or a change in heart rate. 19. A nurse cares for a client with end-stage heart failure who is awaiting a transplant. The client appears depressed and states, “I know a transplant is my last chance, but I don’t want to become a vegetable.” How should the nurse respond? a. “Would you like to speak with a priest or chaplain?” b. “I will arrange for a psychiatrist to speak with you.” c. “Do you want to come off the transplant list?” d. “Would you like information about advance directives?” The client is verbalizing a real concern or fear about negative outcomes of the surgery. This anxiety itself can have a negative effect on the outcome of the surgery because of sympathetic stimulation. The best action is to allow the client to verbalize the concern and work toward a positive outcome without making the client feel as though he or she is crazy. The client needs to feel that he or she has some control over the future. The nurse personally provides care to address the client’s concerns instead of pushing the client’s issues off on a chaplain or psychiatrist. The nurse should not jump to conclusions and suggest taking the client off the transplant list, which is the best treatment option. 20. A nurse assesses a client who has a history of heart failure. Which question should the nurse ask to assess the extent of the client’s heart failure? a. “Do you have trouble breathing or chest pain?” b. “Are you able to walk upstairs without fatigue?” c. “Do you awake with breathlessness during the night?” d. “Do you have new-onset heaviness in your legs?” Clients with a history of heart failure generally have negative findings, such as shortness of breath. The nurse needs to determine whether the client’s activity is the same or worse, or whether the client identifies a decrease in activity level. Trouble breathing, chest pain, breathlessness at night, and peripheral edema are symptoms of heart failure, but do not provide data that can determine the extent of the client’s heart failure. 21. A nurse cares for an older adult client with heart failure. The client states, “I don’t know what to do. I don’t want to be a burden to my daughter, but I can’t do it alone. Maybe I should die.” How should the nurse respond? a. “Would you like to talk more about this?” b. “You are lucky to have such a devoted daughter.” c. “It is normal to feel as though you are a burden.” d. “Would you like to meet with the chaplain?” Depression can occur in clients with heart failure, especially older adults. Having the client talk about his or her feelings will help the nurse focus on the actual problem. Open-ended statements allow the client to respond safely and honestly. The other options minimize the client’s concerns and do not allow the nurse to obtain more information to provide client-centered care. 22. A nurse teaches a client with heart failure about energy conservation. Which statement should the nurse include in this client’s teaching? a. “Walk until you become short of breath, and then walk back home.” b. “Gather everything you need for a chore before you begin.” c. “Pull rather than push or carry items heavier than 5 pounds.” d. “Take a walk after dinner every day to build up your strength.” A client who has heart failure should be taught to conserve energy. Gathering all supplies needed for a chore at one time decreases the amount of energy needed. The client should not walk until becoming short of breath because he or she may not make it back home. Pushing a cart takes less energy than pulling or lifting. Although walking after dinner may help the client, the nurse should teach the client to complete activities when he or she has the most energy. This is usually in the morning. 23. A nurse is caring for a client with acute pericarditis who reports substernal precordial pain that radiates to the left side of the neck. Which nonpharmacologic comfort measure should the nurse implement? a. Apply an ice pack to the client’s chest. b. Provide a neck rub, especially on the left side. c. Allow the client to lie in bed with the lights down. d. Sit the client up with a pillow to lean forward on. Pain from acute pericarditis may worsen when the client lays supine. The nurse should position the client in a comfortable position, which usually is upright and leaning slightly forward. Pain is decreased by using gravity to take pressure off the heart muscle. An ice pack and neck rub will not relieve this pain. 24. A nurse assesses a client who has mitral valve regurgitation. For which cardiac dysrhythmia should the nurse assess? a. Preventricular contractions b. Atrial fibrillation c. Symptomatic bradycardia d. Sinus tachycardia Atrial fibrillation is a clinical manifestation of mitral valve regurgitation and stenosis. Preventricular contractions and bradycardia are not associated with valvular problems. These are usually identified in clients with electrolyte imbalances, myocardial infarction, and sinus node problems. Sinus tachycardia is a manifestation of aortic regurgitation due to a decrease in cardiac output. 1. A nurse is assessing a client with left-sided heart failure. For which clinical manifestations should the nurse assess? (Select all that apply.) a. Pulmonary crackles b. Confusion, restlessness c. Pulmonary hypertension d. Dependent edema e. Cough that worsens at night Left-sided heart failure occurs with a decrease in contractility of the heart or an increase in afterload. Most of the signs will be noted in the respiratory system. Right-sided heart failure occurs with problems from the pulmonary vasculature onward including pulmonary hypertension. Signs will be noted before the right atrium or ventricle including dependent edema. 2. A nurse evaluates laboratory results for a client with heart failure. Which results should the nurse expect? (Select all that apply.) a. Hematocrit: 32.8% b. Serum sodium: 130 mEq/L c. Serum potassium: 4.0 mEq/L d. Serum creatinine: 1.0 mg/dL e. Proteinuria f. Microalbuminuria A hematocrit of 32.8% is low (should be 42.6%), indicating a dilutional ratio of red blood cells to fluid. A serum sodium of 130 mEq/L is low because of hemodilution. Microalbuminuria and proteinuria are present, indicating a decrease in renal filtration. These are early warning signs of decreased compliance of the heart. The potassium level is on the high side of normal and the serum creatinine level is normal. 3. A nurse assesses clients on a cardiac unit. Which clients should the nurse identify as at greatest risk for the development of acute pericarditis? (Select all that apply.) a. A 36-year-old woman with systemic lupus erythematosus (SLE) b. A 42-year-old man recovering from coronary artery bypass graft surgery c. A 59-year-old woman recovering from a hysterectomy d. An 80-year-old man with a bacterial infection of the respiratory tract e. An 88-year-old woman with a stage III sacral ulcer Acute pericarditis is most commonly associated acute exacerbations of systemic connective tissue disease, including SLE; with Dressler’s syndrome, or inflammation of the cardiac sac after cardiac surgery or a myocardial infarction; and with infective organisms, including bacterial, viral, and fungal infections. Abdominal and reproductive surgeries and pressure ulcers do not increase clients’ risk for acute pericarditis. 4. After teaching a client with congestive heart failure (CHF), the nurse assesses the client’s understanding. Which client statements indicate a correct understanding of the teaching related to nutritional intake? (Select all that apply.) a. “I’ll read the nutritional labels on food items for salt content.” b. “I will drink at least 3 liters of water each day.” c. “Using salt in moderation will reduce the workload of my heart.” d. “I will eat oatmeal for breakfast instead of ham and eggs.” e. “Substituting fresh vegetables for canned ones will lower my salt intake.” Nutritional therapy for a client with CHF is focused on decreasing sodium and water retention to decrease the workload of the heart. The client should be taught to read nutritional labels on all food items, omit table salt and foods high in sodium (e.g., ham and canned foods), and limit water intake to a normal 2 L/day. 5. A nurse collaborates with an unlicensed assistive personnel (UAP) to provide care for a client with congestive heart failure. Which instructions should the nurse provide to the UAP when delegating care for this client? (Select all that apply.) a. “Reposition the client every 2 hours.” b. “Teach the client to perform deep-breathing exercises.” c. “Accurately record intake and output.” d. “Use the same scale to weigh the client each morning.” e. “Place the client on oxygen if the client becomes short of breath.” The UAP should reposition the client every 2 hours to improve oxygenation and prevent atelectasis. The UAP can also accurately record intake and output, and use the same scale to weigh the client each morning before breakfast. UAPs are not qualified to teach clients or assess the need for and provide oxygen therapy. 6. A nurse prepares to discharge a client who has heart failure. Based on the Heart Failure Core Measure Set, which actions should the nurse complete prior to discharging this client? (Select all that apply.) a. Teach the client about dietary restrictions. b. Ensure the client is prescribed an angiotensin-converting enzyme (ACE) inhibitor. c. Encourage the client to take a baby aspirin each day. d. Confirm that an echocardiogram has been completed. e. Consult a social worker for additional resources. The Heart Failure Core Measure Set includes discharge instructions on diet, activity, medications, weight monitoring and plan for worsening symptoms, evaluation of left ventricular systolic function (usually with an echocardiogram), and prescribing an ACE inhibitor or angiotensin receptor blocker. Aspirin is not part of the Heart Failure Core Measure Set and is usually prescribed for clients who experience a myocardial infarction. Although the nurse may consult the social worker or case manager for additional resources, this is not part of the Core Measures. 7. A nurse prepares to discharge a client who has heart failure. Which questions should the nurse ask to ensure this client’s safety prior to discharging home? (Select all that apply.) a. “Are your bedroom and bathroom on the first floor?” b. “What social support do you have at home?” c. “Will you be able to afford your oxygen therapy?” d. “What spiritual beliefs may impact your recovery?” e. “Are you able to accurately weigh yourself at home?” To ensure safety upon discharge, the nurse should assess for structural barriers to functional ability, such as stairs. The nurse should also assess the client’s available social support, which may include family, friends, and home health services. The client’s ability to adhere to medication and treatments, including daily weights, should also be reviewed. The other questions do not address the client’s safety upon discharge. 8. A nurse assesses a client who is recovering from a heart transplant. Which assessment findings should alert the nurse to the possibility of heart transplant rejection? (Select all that apply.) a. Shortness of breath b. Abdominal bloating c. New-onset bradycardia d. Increased ejection fraction e. Hypertension Clinical manifestations of heart transplant rejection include shortness of breath, fatigue, fluid gain, abdominal bloating, new-onset bradycardia, hypotension, atrial fibrillation or flutter, decreased activity tolerance, and decreased ejection fraction. 9. A nurse assesses a client who is diagnosed with infective endocarditis. Which assessment findings should the nurse expect? (Select all that apply.) a. Weight gain b. Night sweats c. Cardiac murmur d. Abdominal bloating e. Osler’s nodes Clinical manifestations of infective endocarditis include fever with chills, night sweats, malaise and fatigue, anorexia and weight loss, cardiac murmur, and Osler’s nodes on palms of the hands and soles of the feet. Abdominal bloating is a manifestation of heart transplantation rejection. Chapter 37: Care of Patients with Shock 1. A student is caring for a client who suffered massive blood loss after trauma. How does the student correlate the blood loss with the client’s mean arterial pressure (MAP)? a. It causes vasoconstriction and increased MAP. b. Lower blood volume lowers MAP. c. There is no direct correlation to MAP. d. It raises cardiac output and MAP. Lower blood volume will decrease MAP. The other answers are not accurate. 2. A nurse is caring for a client after surgery. The client’s respiratory rate has increased from 12 to 18 breaths/min and the pulse rate increased from 86 to 98 beats/min since they were last assessed 4 hours ago. What action by the nurse is best? a. Ask if the client needs pain medication. b. Assess the client’s tissue perfusion further. c. Document the findings in the client’s chart. d. Increase the rate of the client’s IV infusion. Signs of the earliest stage of shock are subtle and may manifest in slight increases in heart rate, respiratory rate, or blood pressure. Even though these readings are not out of the normal range, the nurse should conduct a thorough assessment of the client, focusing on indicators of perfusion. The client may need pain medication, but this is not the priority at this time. Documentation should be done thoroughly but is not the priority either. The nurse should not increase the rate of the IV infusion without an order. 3. The nurse gets the hand-off report on four clients. Which client should the nurse assess first? a. Client with a blood pressure change of 128/74 to 110/88 mm Hg b. Client with oxygen saturation unchanged at 94% c. Client with a pulse change of 100 to 88 beats/min d. Client with urine output of 40 mL/hr for the last 2 hours This client has a falling systolic blood pressure, rising diastolic blood pressure, and narrowing pulse pressure, all of which may be indications of the progressive stage of shock. The nurse should assess this client first. The client with the unchanged oxygen saturation is stable at this point. Although the client with a change in pulse has a slower rate, it is not an indicator of shock since the pulse is still within the normal range; it may indicate the client’s pain or anxiety has been relieved, or he or she is sleeping or relaxing. A urine output of 40 mL/hr is only slightly above the normal range, which is 30 mL/hr. 4. A nurse is caring for a client after surgery who is restless and apprehensive. The unlicensed assistive personnel (UAP) reports the vital signs and the nurse sees they are only slightly different from previous readings. What action does the nurse delegate next to the UAP? a. Assess the client for pain or discomfort. b. Measure urine output from the catheter. c. Reposition the client to the unaffected side. d. Stay with the client and reassure him or her. Urine output changes are a sensitive early indicator of shock. The nurse should delegate emptying the urinary catheter and measuring output to the UAP as a baseline for hourly urine output measurements. The UAP cannot assess for pain. Repositioning may or may not be effective for decreasing restlessness, but does not take priority over physical assessments. Reassurance is a therapeutic nursing action, but the nurse needs to do more in this situation. 5. A client is in shock and the nurse prepares to administer insulin for a blood glucose reading of 208 mg/dL. The spouse asks why the client needs insulin as the client is not a diabetic. What response by the nurse is best? a. “High glucose is common in shock and needs to be treated.” b. “Some of the medications we are giving are to raise blood sugar.” c. “The IV solution has lots of glucose, which raises blood sugar.” d. “The stress of this illness has made your spouse a diabetic.” High glucose readings are common in shock, and best outcomes are the result of treating them and maintaining glucose readings in the normal range. Medications and IV solutions may raise blood glucose levels, but this is not the most accurate answer. The stress of the illness has not “made” the client diabetic. 6. A nurse caring for a client notes the following assessments: white blood cell count 3800/mm3, blood glucose level 198 mg/dL, and temperature 96.2° F (35.6° C). What action by the nurse takes priority? a. Document the findings in the client’s chart. b. Give the client warmed blankets for comfort. c. Notify the health care provider immediately. d. Prepare to administer insulin per sliding scale. This client has several indicators of sepsis with systemic inflammatory response. The nurse should notify the health care provider immediately. Documentation needs to be thorough but does not take priority. The client may appreciate warm blankets, but comfort measures do not take priority. The client may or may not need insulin. 7. A nurse works at a community center for older adults. What self-management measure can the nurse teach the clients to prevent shock? a. Do not get dehydrated in warm weather. b. Drink fluids on a regular schedule. c. Seek attention for any lacerations. d. Take medications as prescribed. Preventing dehydration in older adults is important because the age-related decrease in the thirst mechanism makes them prone to dehydration. Having older adults drink fluids on a regular schedule will help keep them hydrated without the influence of thirst (or lack of thirst). Telling clients not to get dehydrated is important, but not the best answer because it doesn’t give them the tools to prevent it from occurring. Older adults should seek attention for lacerations, but this is not as important an issue as staying hydrated. Taking medications as prescribed may or may not be related to hydration. 8. A client arrives in the emergency department after being in a car crash with fatalities. The client has a nearly amputated leg that is bleeding profusely. What action by the nurse takes priority? a. Apply direct pressure to the bleeding. b. Ensure the client has a patent airway. c. Obtain consent for emergency surgery. d. Start two large-bore IV catheters. Airway is the priority, followed by breathing and circulation (IVs and direct pressure). Obtaining consent is done by the physician. 9. A client is receiving norepinephrine (Levophed) for shock. What assessment finding best indicates a therapeutic effect from this drug? a. Alert and oriented, answering questions b. Client denial of chest pain or chest pressure c. IV site without redness or swelling d. Urine output of 30 mL/hr for 2 hours Normal cognitive function is a good indicator that the client is receiving the benefits of norepinephrine. The brain is very sensitive to changes in oxygenation and perfusion. Norepinephrine can cause chest pain as an adverse reaction, so the absence of chest pain does not indicate therapeutic effect. The IV site is normal. The urine output is normal, but only minimally so. 10. A student nurse is caring for a client who will be receiving sodium nitroprusside (Nipride) via IV infusion. What action by the student causes the registered nurse to intervene? a. Assessing the IV site before giving the drug b. Obtaining a programmable (“smart”) IV pump c. Removing the IV bag from the brown plastic cover d. Taking and recording a baseline set of vital signs Nitroprusside degrades in the presence of light, so it must be protected by leaving it in the original brown plastic bag when infusing. The other actions are correct, although a “smart” pump is not necessarily required if the facility does not have them available. The drug must be administered via an IV pump, although the programmable pump is preferred for safety. 11. A client has been brought to the emergency department after being shot multiple times. What action should the nurse perform first? a. Apply personal protective equipment. b. Notify local law enforcement officials. c. Obtain “universal” donor blood. d. Prepare the client for emergency surgery. The nurse’s priority is to care for the client. Since the client has gunshot wounds and is bleeding, the nurse applies personal protective equipment (i.e., gloves) prior to care. This takes priority over calling law enforcement. Requesting blood bank products can be delegated. The nurse may or may not have to prepare the client for emergency surgery. 12. A nurse is caring for several clients at risk for shock. Which laboratory value requires the nurse to communicate with the health care provider? a. Creatinine: 0.9 mg/dL b. Lactate: 6 mmol/L c. Sodium: 150 mEq/L d. White blood cell count: 11,000/mm3 A lactate level of 6 mmol/L is high and is indicative of possible shock. A creatinine level of 0.9 mg/dL is normal. A sodium level of 150 mEq/L is high, but that is not related directly to shock. A white blood cell count of 11,000/mm3 is slightly high but is not as critical as the lactate level. 13. A client in shock is apprehensive and slightly confused. What action by the nurse is best? a. Offer to remain with the client for awhile. b. Prepare to administer antianxiety medication. c. Raise all four siderails on the client’s bed. d. Tell the client everything possible is being done. The nurse’s presence will be best to reassure this client. Antianxiety medication is not warranted as this will lower the client’s blood pressure. Using all four siderails on a hospital bed is considered a restraint in most facilities, although the nurse should ensure the client’s safety. Telling a confused client that everything is being done is not the most helpful response. 14. A client is being discharged home after a large myocardial infarction and subsequent coronary artery bypass grafting surgery. The client’s sternal wound has not yet healed. What statement by the client most indicates a higher risk of developing sepsis after discharge? a. “All my friends and neighbors are planning a party for me.” b. “I hope I can get my water turned back on when I get home.” c. “I am going to have my daughter scoop the cat litter box.” d. “My grandkids are so excited to have me coming home!” All these statements indicate a potential for leading to infection once the client gets back home. A large party might include individuals who are themselves ill and contagious. Having litter boxes in the home can expose the client to microbes that can lead to infection. Small children often have upper respiratory infections and poor hand hygiene that spread germs. However, the most worrisome statement is the lack of running water for handwashing and general hygiene and cleaning purposes. 15. A client in shock has been started on dopamine. What assessment finding requires the nurse to communicate with the provider immediately? a. Blood pressure of 98/68 mm Hg b. Pedal pulses 1+/4+ bilaterally c. Report of chest heaviness d. Urine output of 32 mL/hr Chest heaviness or pain indicates myocardial ischemia, a possible adverse effect of dopamine. While taking dopamine, the oxygen requirements of the heart are increased due to increased myocardial workload, and may cause ischemia. Without knowing the client’s previous blood pressure or pedal pulses, there is not enough information to determine if these are an improvement or not. A urine output of 32 mL/hr is acceptable. 1. The student nurse studying shock understands that the common manifestations of this condition are directly related to which problems? (Select all that apply.) a. Anaerobic metabolism b. Hyperglycemia c. Hypotension d. Impaired renal perfusion e. Increased perfusion The common manifestations of shock, no matter the cause, are directly related to the effects of anaerobic metabolism and hypotension. Hyperglycemia, impaired renal function, and increased perfusion are not manifestations of shock. 2. The nurse caring for hospitalized clients includes which actions on their care plans to reduce the possibility of the clients developing shock? (Select all that apply.) a. Assessing and identifying clients at risk b. Monitoring the daily white blood cell count c. Performing proper hand hygiene d. Removing invasive lines as soon as possible e. Using aseptic technique during procedures Assessing and identifying clients at risk for shock is probably the most critical action the nurse can take to prevent shock from occurring. Proper hand hygiene, using aseptic technique, and removing IV lines and catheters are also important actions to prevent shock. Monitoring laboratory values does not prevent shock but can indicate a change. 3. The nurse caring frequently for older adults in the hospital is aware of risk factors that place them at a higher risk for shock. For what factors would the nurse assess? (Select all that apply.) a. Altered mobility/immobility b. Decreased thirst response c. Diminished immune response d. Malnutrition e. Overhydration Immobility, decreased thirst response, diminished immune response, and malnutrition can place the older adult at higher risk of developing shock. Overhydration is not a common risk factor for shock. 4. A client is in the early stages of shock and is restless. What comfort measures does the nurse delegate to the nursing student? (Select all that apply.) a. Bringing the client warm blankets b. Giving the client hot tea to drink c. Massaging the client’s painful legs d. Reorienting the client as needed e. Sitting with the client for reassurance The student can bring the client warm blankets, reorient the client as needed to decrease anxiety, and sit with the client for reassurance. The client should be NPO at this point, so hot tea is prohibited. Massaging the legs is not recommended as this can dislodge any clots present, which may lead to pulmonary embolism. 5. The nurse is caring for a client with suspected severe sepsis. What does the nurse prepare to do within 3 hours of the client being identified as being at risk? (Select all that apply.) a. Administer antibiotics. b. Draw serum lactate levels. c. Infuse vasopressors. d. Measure central venous pressure. e. Obtain blood cultures. Within the first 3 hours of suspecting severe sepsis, the nurse should draw (or facilitate) serum lactate levels, obtain blood cultures (or other cultures), and administer antibiotics (after the cultures have been obtained). Infusing vasopressors and measuring central venous pressure are actions that should occur within the first 6 hours. 1. A client with severe sepsis has a serum lactate level of 6.2 mmol/L. The client weighs 250 pounds. To infuse the amount of fluid this client requires in 24 hours, at what rate does the nurse set the IV pump? (Record your answer using a whole number.) mL/hr 142 mL/hr The client weighs 250 pounds = 113.63636 kg. The fluid requirement for this client is 30 mL/kg = 3409 mL. To infuse this amount over 24 hours, set the pump at 142 mL/hr (3409/24 = 142). Chapter 38: Care of Patients with Acute Coronary Syndromes 1. A client is receiving an infusion of tissue plasminogen activator (t-PA). The nurse assesses the client to be disoriented to person, place, and time. What action by the nurse is best? a. Assess the client’s pupillary responses. b. Request a neurologic consultation. c. Stop the infusion and call the provider. d. Take and document a full set of vital signs. A change in neurologic status in a client receiving t-PA could indicate intracranial hemorrhage. The nurse should stop the infusion and notify the provider immediately. A full assessment, including pupillary responses and vital signs, occurs next. The nurse may or may not need to call a neurologist. 2. A client received tissue plasminogen activator (t-PA) after a myocardial infarction and now is on an intravenous infusion of heparin. The client’s spouse asks why the client needs this medication. What response by the nurse is best? a. “The t-PA didn’t dissolve the entire coronary clot.” b. “The heparin keeps that artery from getting blocked again.” c. “Heparin keeps the blood as thin as possible for a longer time.” d. “The heparin prevents a stroke from occurring as the t-PA wears off.” After the original intracoronary clot has dissolved, large amounts of thrombin are released into the bloodstream, increasing the chance of the vessel reoccluding. The other statements are not accurate. Heparin is not a “blood thinner,” although laypeople may refer to it as such. 3. A client is in the hospital after suffering a myocardial infarction and has bathroom privileges. The nurse assists the client to the bathroom and notes the client’s O2 saturation to be 95%, pulse 88 beats/min, and respiratory rate 16 breaths/min after returning to bed. What action by the nurse is best? a. Administer oxygen at 2 L/min. b. Allow continued bathroom privileges. c. Obtain a bedside commode. d. Suggest the client use a bedpan. This client’s physiologic parameters did not exceed normal during and after activity, so it is safe for the client to continue using the bathroom. There is no indication that the client needs oxygen, a commode, or a bedpan. 4. A nursing student is caring for a client who had a myocardial infarction. The student is confused because the client states nothing is wrong and yet listens attentively while the student provides education on lifestyle changes and healthy menu choices. What response by the faculty member is best? a. “Continue to educate the client on possible healthy changes.” b. “Emphasize complications that can occur with noncompliance.” c. “Tell the client that denial is normal and will soon go away.” d. “You need to make sure the client understands this illness.” Clients are often in denial after a coronary event. The client who seems to be in denial but is compliant with treatment may be using a healthy form of coping that allows time to process the event and start to use problem- focused coping. The student should not discourage this type of denial and coping, but rather continue providing education in a positive manner. Emphasizing complications may make the client defensive and more anxious. Telling the client that denial is normal is placing too much attention on the process. Forcing the client to verbalize understanding of the illness is also potentially threatening to the client. 5. A client undergoing hemodynamic monitoring after a myocardial infarction has a right atrial pressure of 0.5 mm Hg. What action by the nurse is most appropriate? a. Level the transducer at the phlebostatic axis. b. Lay the client in the supine position. c. Prepare to administer diuretics. d. Prepare to administer a fluid bolus. Normal right atrial pressures are from 1 to 8 mm Hg. Lower pressures usually indicate hypovolemia, so the nurse should prepare to administer a fluid bolus. The transducer should remain leveled at the phlebostatic axis. Positioning may or may not influence readings. Diuretics would be contraindicated. 6. A client has hemodynamic monitoring after a myocardial infarction. What safety precaution does the nurse implement for this client? a. Document pulmonary artery wedge pressure (PAWP) readings and assess their trends. b. Ensure the balloon does not remain wedged. c. Keep the client on strict NPO status. d. Maintain the client in a semi-Fowler’s position. If the balloon remains inflated, it can cause pulmonary infarction or rupture. The nurse should ensure the balloon remains deflated between PAWP readings. Documenting PAWP readings and assessing trends is an important nursing action related to hemodynamic monitoring, but is not specifically related to safety. The client does not have to be NPO while undergoing hemodynamic monitoring. Positioning may or may not affect readings. 7. A client has intra-arterial blood pressure monitoring after a myocardial infarction. The nurse notes the client’s heart rate has increased from 88 to 110 beats/min, and the blood pressure dropped from 120/82 to 100/60 mm Hg. What action by the nurse is most appropriate? a. Allow the client to rest quietly. b. Assess the client for bleeding. c. Document the findings in the chart. d. Medicate the client for pain. A major complication related to intra-arterial blood pressure monitoring is hemorrhage from the insertion site. Since these vital signs are out of the normal range, are a change, and are consistent with blood loss, the nurse should assess the client for any bleeding associated with the arterial line. The nurse should document the findings after a full assessment. The client may or may not need pain medication and rest; the nurse first needs to rule out any emergent bleeding. 8. A client is in the preoperative holding area prior to an emergency coronary artery bypass graft (CABG). The client is yelling at family members and tells the doctor to “just get this over with” when asked to sign the consent form. What action by the nurse is best? a. Ask the family members to wait in the waiting area. b. Inform the client that this behavior is unacceptable. c. Stay out of the room to decrease the client’s stress levels. d. Tell the client that anxiety is common and that you can help. Preoperative fear and anxiety are common prior to cardiac surgery, especially in emergent situations. The client is exhibiting anxiety, and the nurse should reassure the client that fear is common and offer to help. The other actions will not reduce the client’s anxiety. 9. A client is in the clinic a month after having a myocardial infarction. The client reports sleeping well since moving into the guest bedroom. What response by the nurse is best? a. “Do you have any concerns about sexuality?” b. “I’m glad to hear you are sleeping well now.” c. “Sleep near your spouse in case of emergency.” d. “Why would you move into the guest room?” Concerns about resuming sexual activity are common after cardiac events. The nurse should gently inquire if this is the issue. While it is good that the client is sleeping well, the nurse should investigate the reason for the move. The other two responses are likely to cause the client to be defensive. 10. A client in the cardiac stepdown unit reports severe, crushing chest pain accompanied by nausea and vomiting. What action by the nurse takes priority? a. Administer an aspirin. b. Call for an electrocardiogram (ECG). c. Maintain airway patency. d. Notify the provider. Airway always is the priority. The other actions are important in this situation as well, but the nurse should stay with the client and ensure the airway remains patent (especially if vomiting occurs) while another person calls the provider (or Rapid Response Team) and facilitates getting an ECG done. Aspirin will probably be administered, depending on the provider’s prescription and the client’s current medications. 11. An older adult is on cardiac monitoring after a myocardial infarction. The client shows frequent dysrhythmias. What action by the nurse is most appropriate? a. Assess for any hemodynamic effects of the rhythm. b. Prepare to administer antidysrhythmic medication. c. Notify the provider or call the Rapid Response Team. d. Turn the alarms off on the cardiac monitor. Older clients may have dysrhythmias due to age-related changes in the cardiac conduction system. They may have no significant hemodynamic effects from these changes. The nurse should first assess for the effects of the dysrhythmia before proceeding further. The alarms on a cardiac monitor should never be shut off. The other two actions may or may not be needed. 12. The nurse is preparing to change a client’s sternal dressing. What action by the nurse is most important? a. Assess vital signs. b. Don a mask and gown. c. Gather needed supplies. d. Perform hand hygiene. To prevent a sternal wound infection, the nurse washes hands or performs hand hygiene as a priority. Vital signs do not necessarily need to be assessed beforehand. A mask and gown are not needed. The nurse should gather needed supplies, but this is not the priority. 13. A client has an intra-arterial blood pressure monitoring line. The nurse notes bright red blood on the client’s sheets. What action should the nurse perform first? a. Assess the insertion site. b. Change the client’s sheets. c. Put on a pair of gloves. d. Assess blood pressure. For the nurse’s safety, he or she should put on a pair of gloves to prevent blood exposure. The other actions are appropriate as well, but first the nurse must don a pair of gloves. 14. A nurse is in charge of the coronary intensive care unit. Which client should the nurse see first? a. Client on a nitroglycerin infusion at 5 mcg/min, not titrated in the last 4 hours b. Client who is 1 day post coronary artery bypass graft, blood pressure 180/100 mm Hg c. Client who is 1 day post percutaneous coronary intervention, going home this morning d. Client who is 2 days post coronary artery bypass graft, became dizzy this a.m. while walking Hypertension after coronary artery bypass graft surgery can be dangerous because it puts too much pressure on the suture lines and can cause bleeding. The charge nurse should see this client first. The client who became dizzy earlier should be seen next. The client on the nitroglycerin drip is stable. The client going home can wait until the other clients are cared for. 15. A client with coronary artery disease (CAD) asks the nurse about taking fish oil supplements. What response by the nurse is best? a. “Fish oil is contraindicated with most drugs for CAD.” b. “The best source is fish, but pills have benefits too.” c. “There is no evidence to support fish oil use with CAD.” d. “You can reverse CAD totally with diet and supplements.” Omega-3 fatty acids have shown benefit in reducing lipid levels, in reducing the incidence of sudden cardiac death, and for stabilizing atherosclerotic plaque. The best source is fish three times a week or some fish oil supplements. The other options are not accurate. 16. A client has presented to the emergency department with an acute myocardial infarction (MI). What action by the nurse is best to meet The Joint Commission’s Core Measures outcomes? a. Obtain an electrocardiogram (ECG) now and in the morning. b. Give the client an aspirin. c. Notify the Rapid Response Team. d. Prepare to administer thrombolytics. The Joint Commission’s Core Measures set for acute MI require that aspirin is administered when a client with MI presents to the emergency department or when an MI occurs in the hospital. A rapid ECG is vital, but getting another one in the morning is not part of the Core Measures set. The Rapid Response Team is not needed if an emergency department provider is available. Thrombolytics may or may not be needed. 17. A nurse is caring for four clients. Which client should the nurse assess first? a. Client with an acute myocardial infarction, pulse 102 beats/min b. Client who is 1 hour post angioplasty, has tongue swelling and anxiety c. Client who is post coronary artery bypass, chest tube drained 100 mL/hr d. Client who is post coronary artery bypass, potassium 4.2 mEq/L The post-angioplasty client with tongue swelling and anxiety is exhibiting manifestations of an allergic reaction that could progress to anaphylaxis. The nurse should assess this client first. 18. A nurse is caring for a client who is intubated and has an intra-aortic balloon pump. The client is restless and agitated. What action should the nurse perform first for comfort? a. Allow family members to remain at the bedside. b. Ask the family if the client would like a fan in the room. c. Keep the television tuned to the client’s favorite channel. d. Speak loudly to the client in case of hearing problems. Allowing the family to remain at the bedside can help calm the client with familiar voices (and faces if the client wakes up). A fan might be helpful but may also spread germs through air movement. The TV should not be kept on all the time to allow for rest. Speaking loudly may agitate the client more. 19. The nurse is caring for a client with a chest tube after a coronary artery bypass graft. The drainage slows significantly. What action by the nurse is most important? a. Increase the setting on the suction. b. Notify the provider immediately. c. Re-position the chest tube. d. Take the tubing apart to assess for clots. If the drainage in the chest tube decreases significantly and dramatically, the tube may be blocked by a clot. This could lead to cardiac tamponade. The nurse should notify the provider immediately. The nurse should not independently increase the suction, re-position the chest tube, or take the tubing apart. 20. A home health care nurse is visiting an older client who lives alone after being discharged from the hospital after a coronary artery bypass graft. What finding in the home most causes the nurse to consider additional referrals? a. Dirty carpets in need of vacuuming b. Expired food in the refrigerator c. Old medications in the kitchen d. Several cats present in the home Expired food in the refrigerator demonstrates a safety concern for the client and a possible lack of money to buy food. The nurse can consider a referral to Meals on Wheels or another home-based food program. Dirty carpets may indicate the client has no household help and is waiting for clearance to vacuum. Old medications can be managed by the home health care nurse and the client working collaboratively. Having pets is not a cause for concern. 21. A client is on a dopamine infusion via a peripheral line. What action by the nurse takes priority for safety? a. Assess the IV site hourly. b. Monitor the pedal pulses. c. Monitor the client’s vital signs. d. Obtain consent for a central line. Dopamine should be infused through a central line to prevent extravasation and necrosis of tissue. If it needs to be run peripherally, the nurse assesses the site hourly for problems. When the client is getting the central line, ensuring informed consent is on the chart is a priority. But at this point, the client has only a peripheral line, so caution must be taken to preserve the integrity of the client’s integumentary system. Monitoring pedal pulses and vital signs give indications as to how well the drug is working. 22. A client had an acute myocardial infarction. What assessment finding indicates to the nurse that a significant complication has occurred? a. Blood pressure that is 20 mm Hg below baseline b. Oxygen saturation of 94% on room air c. Poor peripheral pulses and cool skin d. Urine output of 1.2 mL/kg/hr for 4 hours Poor peripheral pulses and cool skin may be signs of impending cardiogenic shock and should be reported immediately. A blood pressure drop of 20 mm Hg is not worrisome. An oxygen saturation of 94% is just slightly below normal. A urine output of 1.2 mL/kg/hr for 4 hours is normal. 23. A client presents to the emergency department with an acute myocardial infarction (MI) at 1500 (3:00 PM). The facility has 24-hour catheterization laboratory abilities. To meet The Joint Commission’s Core Measures set, by what time should the client have a percutaneous coronary intervention performed? a. 1530 (3:30 PM) b. 1600 (4:00 PM) c. 1630 (4:30 PM) d. 1700 (5:00 PM) The Joint Commission’s Core Measures set for MI includes percutaneous coronary intervention within 90 minutes of diagnosis of myocardial infarction. Therefore, the client should have a percutaneous coronary intervention performed no later than 1630 (4:30 PM). 24. The provider requests the nurse start an infusion of an inotropic agent on a client. How does the nurse explain the action of these drugs to the client and spouse? a. “It constricts vessels, improving blood flow.” b. “It dilates vessels, which lessens the work of the heart.” c. “It increases the force of the heart’s contractions.” d. “It slows the heart rate down for better filling.” A positive inotrope is a medication that increases the strength of the heart’s contractions. The other options are not correct. 25. A nurse is assessing a client who had a myocardial infarction. Upon auscultating heart sounds, the nurse hears the following sound. What action by the nurse is most appropriate? a. Assess for further chest pain. b. Call the Rapid Response Team. c. Have the client sit upright. d. Listen to the client’s lung sounds. The sound the nurse hears is an S3 heart sound, an abnormal sound that may indicate heart failure. The nurse should next assess the client’s lung sounds. Assessing for chest pain is not directly related. There is no indication that the Rapid Response Team is needed. Having the client sit up will not change the heart sound. 26. A client had an inferior wall myocardial infarction (MI). The nurse notes the client’s cardiac rhythm as shown below: What action by the nurse is most important? a. Assess the client’s blood pressure and level of consciousness. b. Call the health care provider or the Rapid Response Team. c. Obtain a permit for an emergency temporary pacemaker insertion. d. Prepare to administer antidysrhythmic medication. Clients with an inferior wall MI often have bradycardia and blocks that lead to decreased perfusion, as seen in this ECG strip showing sinus bradycardia. The nurse should first assess the client’s hemodynamic status, including vital signs and level of consciousness. The client may or may not need the Rapid Response Team, a temporary pacemaker, or medication; there is no indication of this in the question. 1. A nursing student learns about modifiable risk factors for coronary artery disease. Which factors does this include? (Select all that apply.) a. Age b. Hypertension c. Obesity d. Smoking e. Stress Hypertension, obesity, smoking, and excessive stress are all modifiable risk factors for coronary artery disease. Age is a nonmodifiable risk factor. 2. A nurse is caring for a client who had coronary artery bypass grafting yesterday. What actions does the nurse delegate to the unlicensed assistive personnel (UAP)? (Select all that apply.) a. Assist the client to the chair for meals and to the bathroom. b. Encourage the client to use the spirometer every 4 hours. c. Ensure the client wears TED hose or sequential compression devices. d. Have the client rate pain on a 0-to-10 scale and report to the nurse. e. Take and record a full set of vital signs per hospital protocol. The nurse can delegate assisting the client to get up in the chair or ambulate to the bathroom, applying TEDs or sequential compression devices, and taking/recording vital signs. The spirometer should be used every hour the day after surgery. Assessing pain using a 0-to-10 scale is a nursing assessment, although if the client reports pain, the UAP should inform the nurse so a more detailed assessment is done. 3. A nursing student studying acute coronary syndromes learns that the pain of a myocardial infarction (MI) differs from stable angina in what ways? (Select all that apply.) a. Accompanied by shortness of breath b. Feelings of fear or anxiety c. Lasts less than 15 minutes d. No relief from taking nitroglycerin e. Pain occurs without known cause The pain from an MI is often accompanied by shortness of breath and fear or anxiety. It lasts longer than 15 minutes and is not relieved by nitroglycerin. It occurs without a known cause such as exertion. 4. A client is 1 day postoperative after a coronary artery bypass graft. What nonpharmacologic comfort measures does the nurse include when caring for this client? (Select all that apply.) a. Administer pain medication before ambulating. b. Assist the client into a position of comfort in bed. c. Encourage high-protein diet selections. d. Provide complementary therapies such as music. e. Remind the client to splint the incision when coughing. Nonpharmacologic comfort measures can include positioning, complementary therapies, and splinting the chest incision. Medications are not nonpharmacologic. Food choices are not comfort measures. 5. A nursing student planning to teach clients about risk factors for coronary artery disease (CAD) would include which topics? (Select all that apply.) a. Advanced age b. Diabetes c. Ethnic background d. Medication use e. Smoking Age, diabetes, ethnic background, and smoking are all risk factors for developing CAD; medication use is not. Chapter 45: Care of Critically Ill Patients with Neurologic Problems 1. A client is in the emergency department reporting a brief episode during which he was dizzy, unable to speak, and felt like his legs were very heavy. Currently the client’s neurologic examination is normal. About what drug should the nurse plan to teach the client? a. Alteplase (Activase) b. Clopidogrel (Plavix) c. Heparin sodium d. Mannitol (Osmitrol) This client’s manifestations are consistent with a transient ischemic attack, and the client would be prescribed aspirin or clopidogrel on discharge. Alteplase is used for ischemic stroke. Heparin and mannitol are not used for this condition. 2. A client had an embolic stroke and is having an echocardiogram. When the client asks why the provider ordered “a test on my heart,” how should the nurse respond? a. “Most of these types of blood clots come from the heart.” b. “Some of the blood clots may have gone to your heart too.” c. “We need to see if your heart is strong enough for therapy.” d. “Your heart may have been damaged in the stroke too.” An embolic stroke is caused when blood clots travel from one area of the body to the brain. The most common source of the clots is the heart. The other statements are inaccurate. 3. A nurse receives a report on a client who had a left-sided stroke and has homonymous hemianopsia. What action by the nurse is most appropriate for this client? a. Assess for bladder retention and/or incontinence. b. Listen to the client’s lungs after eating or drinking. c. Prop the client’s right side up when sitting in a chair. d. Rotate the client’s meal tray when the client stops eating. This condition is blindness on the same side of both eyes. The client must turn his or her head to see the entire visual field. The client may not see all the food on the tray, so the nurse rotates it so uneaten food is now within the visual field. This condition is not related to bladder function, difficulty swallowing, or lack of trunk control. 4. A client with a stroke is being evaluated for fibrinolytic therapy. What information from the client or family is most important for the nurse to obtain? a. Loss of bladder control b. Other medical conditions c. Progression of symptoms d. Time of symptom onset The time limit for initiating fibrinolytic therapy for a stroke is 3 to 4.5 hours, so the exact time of symptom onset is the most important information for this client. The other information is not as critical. 5. A client is being prepared for a mechanical embolectomy. What action by the nurse takes priority? a. Assess for contraindications to fibrinolytics. b. Ensure that informed consent is on the chart. c. Perform a full neurologic assessment. d. Review the client’s medication lists. For this invasive procedure, the client needs to give informed consent. The nurse ensures that this is on the chart prior to the procedure beginning. Fibrinolytics are not used. A neurologic assessment and medication review are important, but the consent is the priority. 6. A client had an embolectomy for an arteriovenous malformation (AVM). The client is now reporting a severe headache and has vomited. What action by the nurse takes priority? a. Administer pain medication. b. Assess the client’s vital signs. c. Notify the Rapid Response Team. d. Raise the head of the bed. This client may be experiencing a rebleed from the AVM. The most important action is to call the Rapid Response Team as this is an emergency. The nurse can assess vital signs while someone else notifies the Team, but getting immediate medical attention is the priority. Administering pain medication may not be warranted if the client must return to surgery. The optimal position for the client with an AVM has not been determined, but calling the Rapid Response Team takes priority over positioning. 7. A student nurse is preparing morning medications for a client who had a stroke. The student plans to hold the docusate sodium (Colace) because the client had a large stool earlier. What action by the supervising nurse is best? a. Have the student ask the client if it is desired or not. b. Inform the student that the docusate should be given. c. Tell the student to document the rationale. d. Tell the student to give it unless the client refuses. Stool softeners should be given to clients with neurologic disorders in order to prevent an elevation in intracranial pressure that accompanies the Valsalva maneuver when constipated. The supervising nurse should instruct the student to administer the docusate. The other options are not appropriate. The medication could be held for diarrhea. 8. A client experiences impaired swallowing after a stroke and has worked with speech-language pathology on eating. What nursing assessment best indicates that a priority goal for this problem has been met? a. Chooses preferred items from the menu b. Eats 75% to 100% of all meals and snacks c. Has clear lung sounds on auscultation d. Gains 2 pounds after 1 week Impaired swallowing can lead to aspiration, so the priority goal for this problem is no aspiration. Clear lung sounds is the best indicator that aspiration has not occurred. Choosing menu items is not related to this problem. Eating meals does not indicate the client is not still aspirating. A weight gain indicates improved nutrition but still does not show a lack of aspiration. 9. A client with a stroke has damage to Broca’s area. What intervention to promote communication is best for this client? a. Assess whether or not the client can write. b. Communicate using “yes-or-no” questions. c. Reinforce speech therapy exercises. d. Remind the client not to use neologisms. Damage to Broca’s area often leads to expressive aphasia, wherein the client can understand what is said but cannot express thoughts verbally. In some instances the client can write. The nurse should assess to see if that ability is intact. “Yes-or-no” questions are not good for this type of client because he or she will often answer automatically but incorrectly. Reinforcing speech therapy exercises is good for all clients with communication difficulties. Neologisms are made-up “words” often used by clients with sensory aphasia. 10. A client’s mean arterial pressure is 60 mm Hg and intracranial pressure is 20 mm Hg. Based on the client’s cerebral perfusion pressure, what should the nurse anticipate for this client? a. Impending brain herniation b. Poor prognosis and cognitive function c. Probable complete recovery d. Unable to tell from this information The cerebral perfusion pressure (CPP) is the intracranial pressure subtracted from the mean arterial pressure: in this case, 60 – 20 = 40. For optimal outcomes, CPP should be at least 70 mm Hg. This client has very low CPP, which will probably lead to a poorer prognosis with significant cognitive dysfunction should the client survive. This data does not indicate impending brain herniation or complete recovery. 11. A client has a traumatic brain injury. The nurse assesses the following: pulse change from 82 to 60 beats/min, pulse pressure increase from 26 to 40 mm Hg, and respiratory irregularities. What action by the nurse takes priority? a. Call the provider or Rapid Response Team. b. Increase the rate of the IV fluid administration. c. Notify respiratory therapy for a breathing treatment. d. Prepare to give IV pain medication. These manifestations indicate Cushing’s syndrome, a potentially life-threatening increase in intracranial pressure (ICP), which is an emergency. Immediate medical attention is necessary, so the nurse notifies the provider or the Rapid Response Team. Increasing fluids would increase the ICP. The client does not need a breathing treatment or pain medication. 12. A nurse is caring for four clients in the neurologic intensive care unit. After receiving the hand-off report, which client should the nurse see first? a. Client with a Glasgow Coma Scale score that was 10 and is now is 8 b. Client with a Glasgow Coma Scale score that was 9 and is now is 12 c. Client with a moderate brain injury who is amnesic for the event d. Client who is requesting pain medication for a headache A 2-point decrease in the Glasgow Coma Scale score is clinically significant and the nurse needs to see this client first. An improvement in the score is a good sign. Amnesia is an expected finding with brain injuries, so this client is lower priority. The client requesting pain medication should be seen after the one with the declining Glasgow Coma Scale score. 13. A client is in the clinic for a follow-up visit after a moderate traumatic brain injury. The client’s spouse is very frustrated, stating that the client’s personality has changed and the situation is intolerable. What action by the nurse is best? a. Explain that personality changes are common following brain injuries. b. Ask the client why he or she is acting out and behaving differently. c. Refer the client and spouse to a head injury support group. d. Tell the spouse this is expected and he or she will have to learn to cope. Personality and behavior often change permanently after head injury. The nurse should explain this to the spouse. Asking the client about his or her behavior isn’t useful because the client probably cannot help it. A referral might be a good idea, but the nurse needs to do something in addition to just referring the couple. Telling the spouse to learn to cope belittles the spouse’s concerns and feelings. 14. The nurse is caring for four clients with traumatic brain injuries. Which client should the nurse assess first? a. Client with cerebral perfusion pressure of 72 mm Hg b. Client who has a Glasgow Coma Scale score of 12 c. Client with a PaCO2 of 36 mm Hg who is on a ventilator d. Client who has a temperature of 102° F (38.9° C) A fever is a poor prognostic indicator in clients with brain injuries. The nurse should see this client first. A Glasgow Coma Scale score of 12, a PaCO2 of 36, and cerebral perfusion pressure of 72 mm Hg are all desired outcomes. 15. A nurse is caring for four clients who might be brain dead. Which client would best meet the criteria to allow assessment of brain death? a. Client with a core temperature of 95° F (35° C) for 2 days b. Client in a coma for 2 weeks from a motor vehicle crash c. Client who is found unresponsive in a remote area of a field by a hunter d. Client with a systolic blood pressure of 92 mm Hg since admission In order to determine brain death, clients must meet four criteria: 1) coma from a known cause, 2) normal or near-normal core temperature, 3) normal systolic blood pressure, and 4) at least one neurologic examination. The client who was in the car crash meets two of these criteria. The clients with the lower temperature and lower blood pressure have only one of these criteria. There is no data to support assessment of brain death in the client found by the hunter. 16. A client with a traumatic brain injury is agitated and fighting the ventilator. What drug should the nurse prepare to administer? a. Carbamazepine (Tegretol) b. Dexmedetomidine (Precedex) c. Diazepam (Valium) d. Mannitol (Osmitrol) Dexmedetomidine is often used to manage agitation in the client with traumatic brain injury. Carbamazepine is an antiseizure drug. Diazepam is a benzodiazepine. Mannitol is an osmotic diuretic. 17. A client who had a severe traumatic brain injury is being discharged home, where the spouse will be a full-time caregiver. What statement by the spouse would lead the nurse to provide further education on home care? a. “I know I can take care of all these needs by myself.” b. “I need to seek counseling because I am very angry.” c. “Hopefully things will improve gradually over time.” d. “With respite care and support, I think I can do this.” This caregiver has unrealistic expectations about being able to do everything without help. Acknowledging anger and seeking counseling show a realistic outlook and plans for accomplishing goals. Hoping for improvement over time is also realistic, especially with the inclusion of the word “hopefully.” Realizing the importance of respite care and support also is a realistic outlook. 18. A client in the intensive care unit is scheduled for a lumbar puncture (LP) today. On assessment, the nurse finds the client breathing irregularly with one pupil fixed and dilated. What action by the nurse is best? a. Ensure that informed consent is on the chart. b. Document these findings in the client’s record. c. Give the prescribed preprocedure sedation. d. Notify the provider of the findings immediately. This client is exhibiting signs of increased intracranial pressure. The nurse should notify the provider immediately because performing the LP now could lead to herniation. Informed consent is needed for an LP, but this is not the priority. Documentation should be thorough, but again this is not the priority. The preprocedure sedation (or other preprocedure medications) should not be given as the LP will most likely be canceled. 19. After a craniotomy, the nurse assesses the client and finds dry, sticky mucous membranes and restlessness. The client has IV fluids running at 75 mL/hr. What action by the nurse is best? a. Assess the client’s magnesium level. b. Assess the client’s sodium level. c. Increase the rate of the IV infusion. d. Provide oral care every hour. This client has manifestations of hypernatremia, which is a possible complication after craniotomy. The nurse should assess the client’s serum sodium level. Magnesium level is not related. The nurse does not independently increase the rate of the IV infusion. Providing oral care is also a good option but does not take priority over assessing laboratory results. 20. A nurse assesses a client with the National Institutes of Health (NIH) Stroke Scale and determines the client’s score to be 36. How should the nurse plan care for this client? a. The client will need near-total care. b. The client will need cuing only. c. The client will need safety precautions. d. The client will be discharged home. This client has severe neurologic deficits and will need near-total care. Safety precautions are important but do not give a full picture of the client’s dependence. The client will need more than cuing to complete tasks. A home discharge may be possible, but this does not help the nurse plan care for a very dependent client. 21. A client has a brain abscess and is receiving phenytoin (Dilantin). The spouse questions the use of the drug, saying the client does not have a seizure disorder. What response by the nurse is best? a. “Increased pressure from the abscess can cause seizures.” b. “Preventing febrile seizures with an abscess is important.” c. “Seizures always occur in clients with brain abscesses.” d. “This drug is used to sedate the client with an abscess.” Brain abscesses can lead to seizures as a complication. The nurse should explain this to the spouse. Phenytoin is not used to prevent febrile seizures. Seizures are possible but do not always occur in clients with brain abscesses. This drug is not used for sedation. 22. A client has an intraventricular catheter. What action by the nurse takes priority? a. Document intracranial pressure readings. b. Perform hand hygiene before client care. c. Measure intracranial pressure per hospital policy. d. Teach the client and family about the device. All of the actions are appropriate for this client. However, performing hand hygiene takes priority because it prevents infection, which is a possibly devastating complication. 23. A client has a subarachnoid bolt. What action by the nurse is most important? a. Balancing and recalibrating the device b. Documenting intracranial pressure readings c. Handling the fiberoptic cable with care to avoid breakage d. Monitoring the client’s phlebostatic axis This device needs frequent balancing and recalibration in order to read correctly. Documenting readings is important, but it is more important to ensure the device’s accuracy. The fiberoptic transducer-tipped catheter has a cable that must be handled carefully to avoid breaking it, but ensuring the device’s accuracy is most important. The phlebostatic axis is not related to neurologic monitoring. 24. A nurse is providing community screening for risk factors associated with stroke. Which client would the nurse identify as being at highest risk for a stroke? a. A 27-year-old heavy cocaine user b. A 30-year-old who drinks a beer a day c. A 40-year-old who uses seasonal antihistamines d. A 65-year-old who is active and on no medications Heavy drug use, particularly cocaine, is a risk factor for stroke. Heavy alcohol use is also a risk factor, but one beer a day is not considered heavy drinking. Antihistamines may contain phenylpropanolamine, which also increases the risk for stroke, but this client uses them seasonally and there is no information that they are abused or used heavily. The 65-year-old has only age as a risk factor. 25. A client has a shoulder injury and is scheduled for a magnetic resonance imaging (MRI). The nurse notes the presence of an aneurysm clip in the client’s record. What action by the nurse is best? a. Ask the client how long ago the clip was placed. b. Have the client sign an informed consent form. c. Inform the provider about the aneurysm clip. d. Reschedule the client for computed tomography. Some older clips are metal, which would preclude the use of MRI. The nurse should determine how old the clip is and relay that information to the MRI staff. 26. A nurse is caring for four clients in the neurologic/neurosurgical intensive care unit. Which client should the nurse assess first? a. Client who has been diagnosed with meningitis with a fever of 101° F (38.3° C) b. Client who had a transient ischemic attack and is waiting for teaching on clopidogrel (Plavix) c. Client receiving tissue plasminogen activator (t-PA) who has a change in respiratory pattern and rate d. Client who is waiting for subarachnoid bolt insertion with the consent form already signed The client receiving t-PA has a change in neurologic status while receiving this fibrinolytic therapy. The nurse assesses this client first as he or she may have an intracerebral bleed. The client with meningitis has expected manifestations. The client waiting for discharge teaching is a lower priority. The client waiting for surgery can be assessed quickly after the nurse sees the client who is receiving t-PA, or the nurse could delegate checking on this client to another nurse. 27. The nurse assesses a client’s Glasgow Coma Scale (GCS) score and determines it to be 12 (a 4 in each category). What care should the nurse anticipate for this client? a. Can ambulate independently b. May have trouble swallowing c. Needs frequent re-orientation d. Will need near-total care This client will most likely be confused and need frequent re-orientation. The client may not be able to ambulate at all but should do so independently, not because of mental status. Swallowing is not assessed with the GCS. The client will not need near-total care. 28. After a stroke, a client has ataxia. What intervention is most appropriate to include on the client’s plan of care? a. Ambulate only with a gait belt. b. Encourage double swallowing. c. Monitor lung sounds after eating. d. Perform post-void residuals. Ataxia is a gait disturbance. For the client’s safety, he or she should have assistance and use a gait belt when ambulating. Ataxia is not related to swallowing, aspiration, or voiding. 29. A client in the emergency department is having a stroke and needs a carotid artery angioplasty with stenting. The client’s mental status is deteriorating. What action by the nurse is most appropriate? a. Attempt to find the family to sign a consent. b. Inform the provider that the procedure cannot occur. c. Nothing; no consent is needed in an emergency. d. Sign the consent form for the client. The nurse should attempt to find the family to give consent. If no family is present or can be found, under the principle of emergency consent, a life-saving procedure can be performed without formal consent. The nurse should not just sign the consent form. 30. A client has a traumatic brain injury and a positive halo sign. The client is in the intensive care unit, sedated and on a ventilator, and is in critical but stable condition. What collaborative problem takes priority at this time? a. Inability to communicate b. Nutritional deficit c. Risk for acquiring an infection d. Risk for skin breakdown The positive halo sign indicates a leak of cerebrospinal fluid. This places the client at high risk of acquiring an infection. Communication and nutrition are not priorities compared with preventing a brain infection. The client has a definite risk for a skin breakdown, but it is not the immediate danger a brain infection would be. 1. A nursing student studying the neurologic system learns which information? (Select all that apply.) a. An aneurysm is a ballooning in a weakened part of an arterial wall. b. An arteriovenous malformation is the usual cause of strokes. c. Intracerebral hemorrhage is bleeding directly into the brain. d. Reduced perfusion from vasospasm often makes stroke worse. e. Subarachnoid hemorrhage is caused by high blood pressure. An aneurysm is a ballooning of the weakened part of an arterial wall. Intracerebral hemorrhage is bleeding directly into the brain. Vasospasm often makes the damage from the initial stroke worse because it causes decreased perfusion. An arteriovenous malformation (AVM) is unusual. Subarachnoid hemorrhage is usually caused by a ruptured aneurysm or AVM. 2. The nurse working in the emergency department assesses a client who has symptoms of stroke. For what modifiable risk factors should the nurse assess? (Select all that apply.) a. Alcohol intake b. Diabetes c. High-fat diet d. Obesity e. Smoking Alcohol intake, a high-fat diet, obesity, and smoking are all modifiable risk factors for stroke. Diabetes is not modifiable but is a risk factor that can be controlled with medical intervention. 3. A nurse is caring for a client after a stroke. What actions may the nurse delegate to the unlicensed assistive personnel (UAP)? (Select all that apply.) a. Assess neurologic status with the Glasgow Coma Scale. b. Check and document oxygen saturation every 1 to 2 hours. c. Cluster client care to allow periods of uninterrupted rest. d. Elevate the head of the bed to 45 degrees to prevent aspiration. e. Position the client supine with the head in a neutral midline position. The UAP can take and document vital signs, including oxygen saturation, and keep the client’s head in a neutral, midline position with correct direction from the nurse. The nurse assesses the Glasgow Coma Scale score. The nursing staff should not cluster care because this can cause an increase in the intracranial pressure. The head of the bed should be minimally elevated, up to 30 degrees. 4. A nurse has applied to work at a hospital that has National Stroke Center designation. The nurse realizes the hospital adheres to eight Core Measures for ischemic stroke care. What do these Core Measures include? (Select all that apply.) a. Discharging the client on a statin medication b. Providing the client with comprehensive therapies c. Meeting goals for nutrition within 1 week d. Providing and charting stroke education e. Preventing venous thromboembolism Core Measures established by The Joint Commission include discharging stroke clients on statins, providing and recording stroke education, and taking measures to prevent venous thromboembolism. The client must be assessed for therapies but may go elsewhere for them. Nutrition goals are not part of the Core Measures. 5. A nursing student studying traumatic brain injuries (TBIs) should recognize which facts about these disorders? (Select all that apply.) a. A client with a moderate trauma may need hospitalization. b. A Glasgow Coma Scale score of 10 indicates a mild brain injury. c. Only open head injuries can cause a severe TBI. d. A client with a Glasgow Coma Scale score of 3 has severe TBI. e. The terms “mild TBI” and “concussion” have similar meanings. “Mild TBI” is a term used synonymously with the term “concussion.” A moderate TBI has a Glasgow Coma Scale (GCS) score of 9 to 12, and these clients may need to be hospitalized. Both open and closed head injuries can cause a severe TBI, which is characterized by a GCS score of 3 to 8. 6. A nurse cares for older clients who have traumatic brain injury. What should the nurse understand about this population? (Select all that apply.) a. Admission can overwhelm the coping mechanisms for older clients. b. Alcohol is typically involved in most traumatic brain injuries for this age group. c. These clients are more susceptible to systemic and wound infections. d. Other medical conditions can complicate treatment for these clients. e. Very few traumatic brain injuries occur in this age group. Older clients often tolerate stress poorly, which includes being admitted to a hospital that is unfamiliar and noisy. Because of decreased protective mechanisms, they are more susceptible to both local and systemic infections. Other medical conditions can complicate their treatment and recovery. Alcohol is typically not related to traumatic brain injury in this population; such injury is most often from falls and motor vehicle crashes. The 65- to 76-year-old age group has the second highest rate of brain injuries compared to other age groups. 7. A client has meningitis following brain surgery. What comfort measures may the nurse delegate to the unlicensed assistive personnel (UAP)? (Select all that apply.) a. Applying a cool washcloth to the head b. Assisting the client to a position of comfort c. Keeping voices soft and soothing d. Maintaining low lighting in the room e. Providing antipyretics for fever The client with meningitis often has high fever, pain, and some degree of confusion. Cool washcloths to the forehead are comforting and help with pain. Allowing the client to assume a position of comfort also helps manage pain. Keeping voices low and lights dimmed also helps convey caring in a nonthreatening manner. The nurse provides antipyretics for fever. 8. A nurse is working with many stroke clients. Which clients would the nurse consider referring to a mental health provider on discharge? (Select all that apply.) a. Client who exhibits extreme emotional lability b. Client with an initial National Institutes of Health (NIH) Stroke Scale score of 38 c. Client with mild forgetfulness and a slight limp d. Client who has a past hospitalization for a suicide attempt e. Client who is unable to walk or eat 3 weeks post-stroke Clients most at risk for post-stroke depression are those with a previous history of depression, severe stroke (NIH Stroke Scale score of 38 is severe), and post-stroke physical or cognitive impairment. The client with mild forgetfulness and a slight limp would be a low priority for this referral. 9. A client has a small-bore feeding tube (Dobhoff tube) inserted for continuous enteral feedings while recovering from a traumatic brain injury. What actions should the nurse include in the client’s care? (Select all that apply.) a. Assess tube placement per agency policy. b. Keep the head of the bed elevated at least 30 degrees. c. Listen to lung sounds at least every 4 hours. d. Run continuous feedings on a feeding pump. e. Use blue dye to determine proper placement. All of these options are important for client safety when continuous enteral feedings are in use. Blue dye is not used because it can cause lung injury if aspirated. 10. A nurse is seeing many clients in the neurosurgical clinic. With which clients should the nurse plan to do more teaching? (Select all that apply.) a. Client with an aneurysm coil placed 2 months ago who is taking ibuprofen (Motrin) for sinus headaches b. Client with an aneurysm clip who states that his family is happy there is no chance of recurrence c. Client who had a coil procedure who says that there will be no problem following up for 1 year d. Client who underwent a flow diversion procedure 3 months ago who is taking docusate sodium (Colace) for constipation e. Client who underwent surgical aneurysm ligation 3 months ago who is planning to take a Caribbean cruise After a coil procedure, up to 20% of clients experience re-bleeding in the first year. The client with this coil should not be taking drugs that interfere with clotting. An aneurysm clip can move up to 5 years after placement, so this client and family need to be watchful for changing neurologic status. The other statements show good understanding. 11. A nurse is dismissing a client from the emergency department who has a mild traumatic brain injury. What information obtained from the client represents a possible barrier to self-management? (Select all that apply.) a. Does not want to purchase a thermometer b. Is allergic to acetaminophen (Tylenol) c. Laughing, says “Strenuous? What’s that?” d. Lives alone and is new in town with no friends e. Plans to have a beer and go to bed once home Clients should take acetaminophen for headache. An allergy to this drug may mean the client takes aspirin or ibuprofen (Motrin), which should be avoided. The client needs neurologic checks every 1 to 2 hours, and this client does not seem to have anyone available who can do that. Alcohol needs to be avoided for at least 24 hours. 1. A client in the emergency department is having a stroke and the provider has prescribed the tissue plasminogen activator (t-PA) alteplase (Activase). The client weighs 146 pounds. How much medication will this client receive? (Record your answer using a whole number.) mg 60 mg The dose of t-PA is 0.9 mg/kg with a maximum dose of 90 mg. The client weighs 66.4 kg. 0.9 mg ´ 66.4 = 59.76 mg, which rounds to 60 mg. 2. A client in the emergency department is having a stroke. The client weighs 225 pounds. After the initial bolus of t-Pa, at what rate should the nurse set the IV pump? (Record your answer using a decimal rounded to the nearest tenth.) mL/hr 1.4 mL/hr The client weighs 102 kg. The dose of t-PA is 0.9 mg/kg with a maximum of 90 mg, so the client’s dose is 90 mg. 10% of the dose is given as a bolus IV over the first minute (9 mg). That leaves 81 mg to run in over 59 minutes. which rounds to 1.4 mL/hr. Chapter 68: Care of Patients with Acute Kidney Injury and Chronic Kidney Disease 1. The nurse is assessing a client with a diagnosis of pre-renal acute kidney injury (AKI). Which condition would the nurse expect to find in the client’s recent history? a. Pyelonephritis b. Myocardial infarction c. Bladder cancer d. Kidney stones Pre-renal causes of AKI are related to a decrease in perfusion, such as with a myocardial infarction. Pyelonephritis is an intrinsic or intrarenal cause of AKI related to kidney damage. Bladder cancer and kidney stones are post-renal causes of AKI related to urine flow obstruction. 2. A marathon runner comes into the clinic and states “I have not urinated very much in the last few days.” The nurse notes a heart rate of 110 beats/min and a blood pressure of 86/58 mm Hg. Which action by the nurse is the priority? a. Give the client a bottle of water immediately. b. Start an intravenous line for fluids. c. Teach the client to drink 2 to 3 liters of water daily. d. Perform an electrocardiogram. This athlete is mildly dehydrated as evidenced by the higher heart rate and lower blood pressure. The nurse can start hydrating the client with a bottle of water first, followed by teaching the client to drink 2 to 3 liters of water each day. An intravenous line may be ordered later, after the client’s degree of dehydration is assessed. An electrocardiogram is not necessary at this time. 3. A male client comes into the emergency department with a serum creatinine of 2.2 mg/dL and a blood urea nitrogen (BUN) of 24 mL/dL. What question should the nurse ask first when taking this client’s history? a. “Have you been taking any aspirin, ibuprofen, or naproxen recently?” b. “Do you have anyone in your family with renal failure?” c. “Have you had a diet that is low in protein recently?” d. “Has a relative had a kidney transplant lately?” There are some medications that are nephrotoxic, such as the nonsteroidal anti-inflammatory drugs ibuprofen, aspirin, and naproxen. This would be a good question to initially ask the client since both the serum creatinine and BUN are elevated, indicating some renal problems. A family history of renal failure and kidney transplantation would not be part of the questioning and could cause anxiety in the client. A diet high in protein could be a factor in an increased BUN. 4. A client is admitted with acute kidney injury (AKI) and a urine output of 2000 mL/day. What is the major concern of the nurse regarding this client’s care? a. Edema and pain b. Electrolyte and fluid imbalance c. Cardiac and respiratory status d. Mental health status This client may have an inflammatory cause of AKI with proteins entering the glomerulus and holding the fluid in the filtrate, causing polyuria. Electrolyte loss and fluid balance is essential. Edema and pain are not usually a problem with fluid loss. There could be changes in the client’s cardiac, respiratory, and mental health status if the electrolyte imbalance is not treated. 5. A client with acute kidney injury has a blood pressure of 76/55 mm Hg. The health care provider ordered 1000 mL of normal saline to be infused over 1 hour to maintain perfusion. The client is starting to develop shortness of breath. What is the nurse’s priority action? a. Calculate the mean arterial pressure (MAP). b. Ask for insertion of a pulmonary artery catheter. c. Take the client’s pulse. d. Slow down the normal saline infusion. ANS: D The nurse should assess that the client could be developing fluid overload and respiratory distress and slow down the normal saline infusion. The calculation of the MAP also reflects perfusion. The insertion of a pulmonary artery catheter would evaluate the client’s hemodynamic status, but this should not be the initial action by the nurse. Vital signs are also important after adjusting the intravenous infusion. 6. A client has a serum potassium level of 6.5 mmol/L, a serum creatinine level of 2 mg/dL, and a urine output of 350 mL/day. What is the best action by the nurse? a. Place the client on a cardiac monitor immediately. b. Teach the client to limit high-potassium foods. c. Continue to monitor the client’s intake and output. d. Ask to have the laboratory redraw the blood specimen. The priority action by the nurse should be to check the cardiac status with a monitor. High potassium levels can lead to dysrhythmias. The other choices are logical nursing interventions for acute kidney injury but not the best immediate action. 7. A client has just had a central line catheter placed that is specific for hemodialysis. What is the most appropriate action by the nurse? a. Use the catheter for the next laboratory blood draw. b. Monitor the central venous pressure through this line. c. Access the line for the next intravenous medication. d. Place a heparin or heparin/saline dwell after hemodialysis. The central line should have a heparin or heparin/saline dwell after hemodialysis treatment. The central line catheter used for dialysis should not be used for blood sampling, monitoring central venous pressures, or giving drugs or fluids. 8. A client in the intensive care unit is started on continuous venovenous hemofiltration (CVVH). Which finding is the cause of immediate action by the nurse? a. Blood pressure of 76/58 mm Hg b. Sodium level of 138 mEq/L c. Potassium level of 5.5 mEq/L d. Pulse rate of 90 beats/min Hypotension can be a problem with CVVH if replacement fluid does not provide enough volume to maintain blood pressure. The specially trained nurse needs to monitor for ongoing fluid and electrolyte replacement. The sodium level is normal and the potassium level is slightly elevated, which could be normal findings for someone with acute kidney injury. A pulse rate of 90 beats/min is normal. 9. The nurse is caring for four clients with chronic kidney disease. Which client should the nurse assess first upon initial rounding? a. Woman with a blood pressure of 158/90 mm Hg b. Client with Kussmaul respirations c. Man with skin itching from head to toe d. Client with halitosis and stomatitis Kussmaul respirations indicate a worsening of chronic kidney disease (CKD). The client is increasing the rate and depth of breathing to excrete carbon dioxide through the lungs. Hypertension is common in most clients with CKD, and skin itching increases with calcium-phosphate imbalances, another common finding in CKD. Uremia from CKD causes ammonia to be formed, resulting in the common findings of halitosis and stomatitis. 10. The charge nurse of the medical-surgical unit is making staff assignments. Which staff member should be assigned to a client with chronic kidney disease who is exhibiting a low-grade fever and a pericardial friction rub? a. Registered nurse who just floated from the surgical unit b. Registered nurse who just floated from the dialysis unit c. Registered nurse who was assigned the same client yesterday d. Licensed practical nurse with 5 years’ experience on this floor The client is exhibiting symptoms of pericarditis, which can occur with chronic kidney disease. Continuity of care is important to assess subtle differences in clients. Therefore, the registered nurse (RN) who was assigned to this client previously should again give care to this client. The float nurses would not be as knowledgeable about the unit and its clients. The licensed practical nurse may not have the education level of the RN to assess for pericarditis. 11. A male client with chronic kidney disease (CKD) is refusing to take his medication and has missed two hemodialysis appointments. What is the best initial action for the nurse? a. Discuss what the treatment regimen means to him. b. Refer the client to a mental health nurse practitioner. c. Reschedule the appointments to another date and time. d. Discuss the option of peritoneal dialysis. The initial action for the nurse is to assess anxiety, coping styles, and the client’s acceptance of the required treatment for CKD. The client may be in denial of the diagnosis. While rescheduling hemodialysis appointments may help, and referral to a mental health practitioner and the possibility of peritoneal dialysis are all viable options, assessment of the client’s acceptance of the treatment should come first. 12. A client is taking furosemide (Lasix) 40 mg/day for management of chronic kidney disease (CKD). To detect the positive effect of the medication, what action of the nurse is best? a. Obtain daily weights of the client. b. Auscultate heart and breath sounds. c. Palpate the client’s abdomen. d. Assess the client’s diet history. Furosemide (Lasix) is a loop diuretic that helps reduce fluid overload and hypertension in clients with early stages of CKD. One kilogram of weight equals about 1 liter of fluid retained in the client, so daily weights are necessary to monitor the response of the client to the medication. Heart and breath sounds should be assessed if there is fluid retention, as in heart failure. Palpation of the client’s abdomen is not necessary, but the nurse should check for edema. The diet history of the client would be helpful to assess electrolyte replacement since potassium is lost with this diuretic, but this does not assess the effect of the medication. 13. A client is diagnosed with chronic kidney disease (CKD). What is an ideal goal of treatment set by the nurse in the care plan to reduce the risk of pulmonary edema? a. Maintaining oxygen saturation of 89% b. Minimal crackles and wheezes in lung sounds c. Maintaining a balanced intake and output d. Limited shortness of breath upon exertion With an optimal fluid balance, the client will be more able to eject blood from the left ventricle without increased pressure in the left ventricle and pulmonary vessels. Other ideal goals are oxygen saturations greater than 92%, no auscultated crackles or wheezes, and no demonstrated shortness of breath. 14. A client has a long history of hypertension. Which category of medications would the nurse expect to be ordered to avoid chronic kidney disease (CKD)? a. Antibiotic b. Histamine blocker c. Bronchodilator d. Angiotensin-converting enzyme (ACE) inhibitor ACE inhibitors stop the conversion of angiotensin I to the vasoconstrictor angiotensin II. This category of medication also blocks bradykinin and prostaglandin, increases renin, and decreases aldosterone, which promotes vasodilation and perfusion to the kidney. Antibiotics fight infection, histamine blockers decrease inflammation, and bronchodilators increase the size of the bronchi; none of these medications helps slow the progression of CKD in clients with hypertension. 15. A 70-kg adult with chronic renal failure is on a 40-g protein diet. The client has a reduced glomerular filtration rate and is not undergoing dialysis. Which result would give the nurse the most concern? a. Albumin level of 2.5 g/dL b. Phosphorus level of 5 mg/dL c. Sodium level of 135 mmol/L d. Potassium level of 5.5 mmol/L Protein restriction is necessary with chronic renal failure due to the buildup of waste products from protein breakdown. The nurse would be concerned with the low albumin level since this indicates that the protein in the diet is not enough for the client’s metabolic needs. The electrolyte values are not related to the protein-restricted diet. 16. The nurse is teaching a client with chronic kidney disease (CKD) about the sodium restriction needed in the diet to prevent edema and hypertension. Which statement by the client indicates more teaching is needed? a. “I am thrilled that I can continue to eat fast food.” b. “I will cut out bacon with my eggs every morning.” c. “My cooking style will change by not adding salt.” d. “I will probably lose weight by cutting out potato chips.” Fast food restaurants usually serve food that is high in sodium. This statement indicates that more teaching needs to occur. The other statements show a correct understanding of the teaching. 17. A client is placed on fluid restrictions because of chronic kidney disease (CKD). Which assessment finding would alert the nurse that the client’s fluid balance is stable at this time? a. Decreased calcium levels b. Increased phosphorus levels c. No adventitious sounds in the lungs d. Increased edema in the legs The absence of adventitious sounds upon auscultation of the lungs indicates a lack of fluid overload and fluid balance in the client’s body. Decreased calcium levels and increased phosphorus levels are common findings with CKD. Edema would indicate a fluid imbalance. 18. A client with chronic kidney disease (CKD) is experiencing nausea, vomiting, visual changes, and anorexia. Which action by the nurse is best? a. Check the client’s digoxin (Lanoxin) level. b. Administer an anti-nausea medication. c. Ask if the client is able to eat crackers. d. Get a referral to a gastrointestinal provider. These signs and symptoms are indications of digoxin (Lanoxin) toxicity. The nurse should check the level of this medication. Administering antiemetics, asking if the client can eat, and obtaining a referral to a specialist all address the client’s symptoms but do not lead to the cause of the symptoms. 19. The nurse is taking the vital signs of a client after hemodialysis. Blood pressure is 110/58 mm Hg, pulse 66 beats/min, and temperature is 99.8° F (37.6° C). What is the most appropriate action by the nurse? a. Administer fluid to increase blood pressure. b. Check the white blood cell count. c. Monitor the client’s temperature. d. Connect the client to an electrocardiographic (ECG) monitor. During hemodialysis, the dialysate is warmed to increase diffusion and prevent hypothermia. The client’s temperature could reflect the temperature of the dialysate. There is no indication to check the white blood cell count or connect the client to an ECG monitor. The other vital signs are within normal limits. 20. The nurse is teaching the main principles of hemodialysis to a client with chronic kidney disease. Which statement by the client indicates a need for further teaching by the nurse? a. “My sodium level changes by movement from the blood into the dialysate.” b. “Dialysis works by movement of wastes from lower to higher concentration.” c. “Extra fluid can be pulled from the blood by osmosis.” d. “The dialysate is similar to blood but without any toxins.” Dialysis works using the passive transfer of toxins by diffusion. Diffusion is the movement of molecules from an area of higher concentration to an area of lower concentration. The other statements show a correct understanding about hemodialysis. 21. The charge nurse is orienting a float nurse to an assigned client with an arteriovenous (AV) fistula for hemodialysis in her left arm. Which action by the float nurse would be considered unsafe? a. Palpating the access site for a bruit or thrill b. Using the right arm for a blood pressure reading c. Administering intravenous fluids through the AV fistula d. Checking distal pulses in the left arm The nurse should not use the arm with the AV fistula for intravenous infusion, blood pressure readings, or venipuncture. Compression and infection can result in the loss of the AV fistula. The AV fistula should be monitored by auscultating or palpating the access site. Checking the distal pulse would be an appropriate assessment. 22. A client is assessed by the nurse after a hemodialysis session. The nurse notes bleeding from the client’s nose and around the intravenous catheter. What action by the nurse is the priority? a. Hold pressure over the client’s nose for 10 minutes. b. Take the client’s pulse, blood pressure, and temperature. c. Assess for a bruit or thrill over the arteriovenous fistula. d. Prepare protamine sulfate for administration. Heparin is used with hemodialysis treatments. The bleeding alerts the nurse that too much anticoagulant is in the client’s system and protamine sulfate should be administered. Pressure, taking vital signs, and assessing for a bruit or thrill are not as important as medication administration. 23. A nurse is caring for a client who is scheduled for a dose of cefazolin and vitamins at this time. Hemodialysis for this client is also scheduled in 60 minutes. Which action by the nurse is best? a. Administer cefazolin since the level of the antibiotic must be maintained. b. Hold the vitamins but administer the cefazolin. c. Hold the cefazolin but administer the vitamins. d. Hold all medications since both cefazolin and vitamins are dialyzable. Both the cefazolin and the vitamins should be held until after the hemodialysis is completed because they would otherwise be removed by the dialysis process. 24. A client is having a peritoneal dialysis treatment. The nurse notes an opaque color to the effluent. What is the priority action by the nurse? a. Warm the dialysate solution in a microwave before instillation. b. Take a sample of the effluent and send to the laboratory. c. Flush the tubing with normal saline to maintain patency of the catheter. d. Check the peritoneal catheter for kinking and curling. An opaque or cloudy effluent is the first sign of peritonitis. A sample of the effluent would need to be sent to the laboratory for culture and sensitivity in order to administer the correct antibiotic. Warming the dialysate in a microwave and flushing the tubing are not safe actions by the nurse. Checking the catheter for obstruction is a viable option but will not treat the peritonitis. 25. The nurse is teaching a client how to increase the flow of dialysate into the peritoneal cavity during dialysis. Which statement by the client demonstrates a correct understanding of the teaching? a. “I should leave the drainage bag above the level of my abdomen.” b. “I could flush the tubing with normal saline if the flow stops.” c. “I should take a stool softener every morning to avoid constipation.” d. “My diet should have low fiber in it to prevent any irritation.” Inflow and outflow problems of the dialysate are best controlled by preventing constipation. A daily stool softener is the best option for the client. The drainage bag should be below the level of the abdomen. Flushing the tubing will not help with the flow. A diet high in fiber will also help with a constipation problem. 26. A client with chronic kidney disease states, “I feel chained to the hemodialysis machine.” What is the nurse’s best response to the client’s statement? a. “That feeling will gradually go away as you get used to the treatment.” b. “You probably need to see a psychiatrist to see if you are depressed.” c. “Do you need help from social services to discuss financial aid?” d. “Tell me more about your feelings regarding hemodialysis treatment.” The nurse needs to explore the client’s feelings in order to help the client cope and enter a phase of acceptance or resignation. It is common for clients to be discouraged because of the dependency of the treatment, especially during the first year. Referrals to a mental health provider or social services are possibilities, but only after exploring the client’s feelings first. Telling the client his or her feelings will go away is dismissive of the client’s concerns. 27. A client is recovering from a kidney transplant. The client’s urine output was 1500 mL over the last 12-hour period since transplantation. What is the priority assessment by the nurse? a. Checking skin turgor b. Taking blood pressure c. Assessing lung sounds d. Weighing the client By taking blood pressure, the nurse is assessing for hypotension that could compromise perfusion to the new kidney. The nurse then should notify the provider immediately. Skin turgor, lung sounds, and weight could give information about the fluid status of the client, but they are not the priority assessment. 28. A nurse reviews these laboratory values of a client who returned from kidney transplantation 12 hours ago: Sodium 136 mEq/L Potassium 5 mEq/L Blood urea nitrogen (BUN) 44 mg/dL Serum creatinine 2.5 mg/dL What initial intervention would the nurse anticipate? a. Start hemodialysis immediately. b. Discuss the need for peritoneal dialysis. c. Increase the dose of immunosuppression. d. Return the client to surgery for exploration. The client may need a higher dose of immunosuppressive medication as evidenced by the elevated BUN and serum creatinine levels. This increased dose may reverse the possible acute rejection of the transplanted kidney. The client does not need hemodialysis, peritoneal dialysis, or further surgery at this point. 1. The nurse is caring for five clients on the medical-surgical unit. Which clients would the nurse consider to be at risk for post-renal acute kidney injury (AKI)? (Select all that apply.) a. Man with prostate cancer b. Woman with blood clots in the urinary tract c. Client with ureterolithiasis d. Firefighter with severe burns e. Young woman with lupus Urine flow obstruction, such as prostate cancer, blood clots in the urinary tract, and kidney stones (ureterolithiasis), causes post-renal AKI. Severe burns would be a pre-renal cause. Lupus would be an intrarenal cause for AKI. 2. A nurse is caring for a postoperative 70-kg client who had major blood loss during surgery. Which findings by the nurse should prompt immediate action to prevent acute kidney injury? (Select all that apply.) a. Urine output of 100 mL in 4 hours b. Urine output of 500 mL in 12 hours c. Large amount of sediment in the urine d. Amber, odorless urine e. Blood pressure of 90/60 mm Hg The low urine output, sediment, and blood pressure should be reported to the provider. Postoperatively, the nurse should measure intake and output, check the characteristics of the urine, and report sediment, hematuria, and urine output of less than 0.5 mL/kg/hour for 3 to 4 hours. A urine output of 100 mL is low, but a urine output of 500 mL in 12 hours should be within normal limits. Perfusion to the kidneys is compromised with low blood pressure. The amber odorless urine is normal. 3. A client is hospitalized in the oliguric phase of acute kidney injury (AKI) and is receiving tube feedings. The nurse is teaching the client’s spouse about the kidney-specific formulation for the enteral solution compared to standard formulas. What components should be discussed in the teaching plan? (Select all that apply.) a. Lower sodium b. Higher calcium c. Lower potassium d. Higher phosphorus e. Higher calories Many clients with AKI are too ill to meet caloric goals and require tube feedings with kidney-specific formulas that are lower in sodium, potassium, and phosphorus, and higher in calories than are standard formulas. 4. The nurse is teaching a client with diabetes mellitus how to prevent or delay chronic kidney disease (CKD). Which client statements indicate a lack of understanding of the teaching? (Select all that apply.) a. “I need to decrease sodium, cholesterol, and protein in my diet.” b. “My weight should be maintained at a body mass index of 30.” c. “Smoking should be stopped as soon as I possibly can.” d. “I can continue to take an aspirin every 4 to 8 hours for my pain.” e. “I really only need to drink a couple of glasses of water each day.” Weight should be maintained at a body mass index (BMI) of 22 to 25. A BMI of 30 indicates obesity. The use of nonsteroidal anti-inflammatory drugs such as aspirin should be limited to the lowest time at the lowest dose due to interference with kidney blood flow. The client should drink at least 2 liters of water daily. 5. A nurse is giving discharge instructions to a client recently diagnosed with chronic kidney disease (CKD). Which statements made by the client indicate a correct understanding of the teaching? (Select all that apply.) a. “I can continue to take antacids to relieve heartburn.” b. “I need to ask for an antibiotic when scheduling a dental appointment.” c. “I’ll need to check my blood sugar often to prevent hypoglycemia.” d. “The dose of my pain medication may have to be adjusted.” e. “I should watch for bleeding when taking my anticoagulants.” In discharge teaching, the nurse must emphasize that the client needs to have an antibiotic prophylactically before dental procedures to prevent infection. There may be a need for dose reduction in medications if the kidney is not excreting them properly (antacids with magnesium, antibiotics, antidiabetic drugs, insulin, opioids, and anticoagulants). 6. A client is undergoing hemodialysis. The client’s blood pressure at the beginning of the procedure was 136/88 mm Hg, and now it is 110/54 mm Hg. What actions should the nurse perform to maintain blood pressure? (Select all that apply.) a. Adjust the rate of extracorporeal blood flow. b. Place the client in the Trendelenburg position. c. Stop the hemodialysis treatment. d. Administer a 250-mL bolus of normal saline. e. Contact the health care provider for orders. Hypotension occurs often during hemodialysis treatments as a result of vasodilation from the warmed dialysate. Modest decreases in blood pressure, as is the case with this client, can be maintained with rate adjustment, Trendelenburg positioning, and a fluid bolus. If the blood pressure drops considerably after two boluses and cooling dialysate, the hemodialysis can be stopped and the health care provider contacted. 7. A client is unsure of the decision to undergo peritoneal dialysis (PD) and wishes to discuss the advantages of this treatment with the nurse. Which statements by the nurse are accurate regarding PD? (Select all that apply.) a. “You will not need vascular access to perform PD.” b. “There is less restriction of protein and fluids.” c. “You will have no risk for infection with PD.” d. “You have flexible scheduling for the exchanges.” e. “It takes less time than hemodialysis treatments.” PD is based on exchanges of waste, fluid, and electrolytes in the peritoneal cavity. There is no need for vascular access. Protein is lost in the exchange, which allows for more protein and fluid in the diet. There is flexibility in the time for exchanges, but the treatment takes a longer period of time compared to hemodialysis. There still is risk for infection with PD, especially peritonitis. 1. A client in the intensive care unit with acute kidney injury (AKI) must maintain a mean arterial pressure (MAP) of 65 mm Hg to promote kidney perfusion. What is the client’s MAP if the blood pressure is 98/50 mm Hg? (Record your answer using a whole number.) mm Hg 66 mm Hg [Show More]
Last updated: 1 year ago
Preview 1 out of 89 pages
 (1).png)
Buy this document to get the full access instantly
Instant Download Access after purchase
Add to cartInstant download
We Accept:

Reviews( 0 )
$17.50
Document information
Connected school, study & course
About the document
Uploaded On
Mar 02, 2022
Number of pages
89
Written in

Additional information
This document has been written for:
Uploaded
Mar 02, 2022
Downloads
0
Views
75

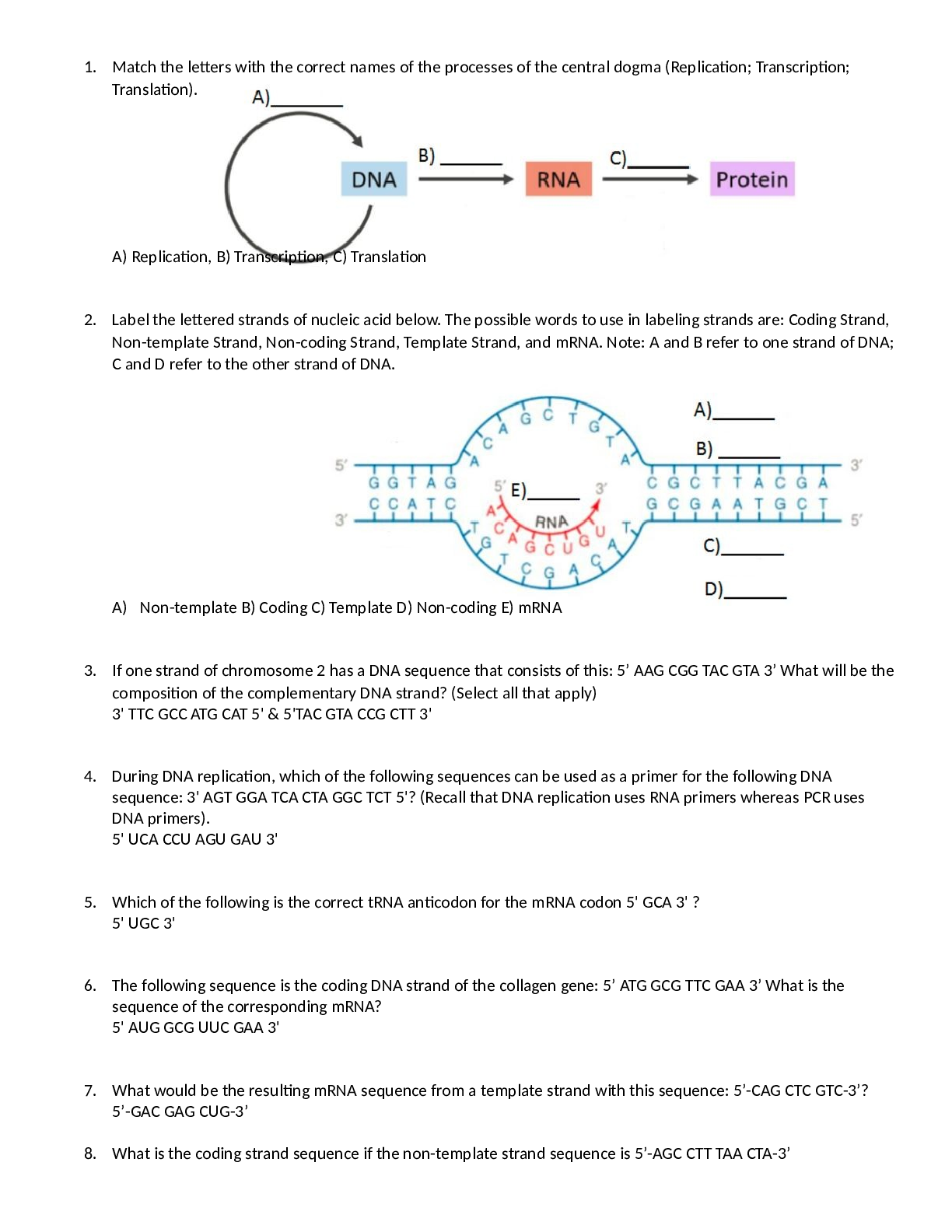

.png)
.png)
.png)
.png)
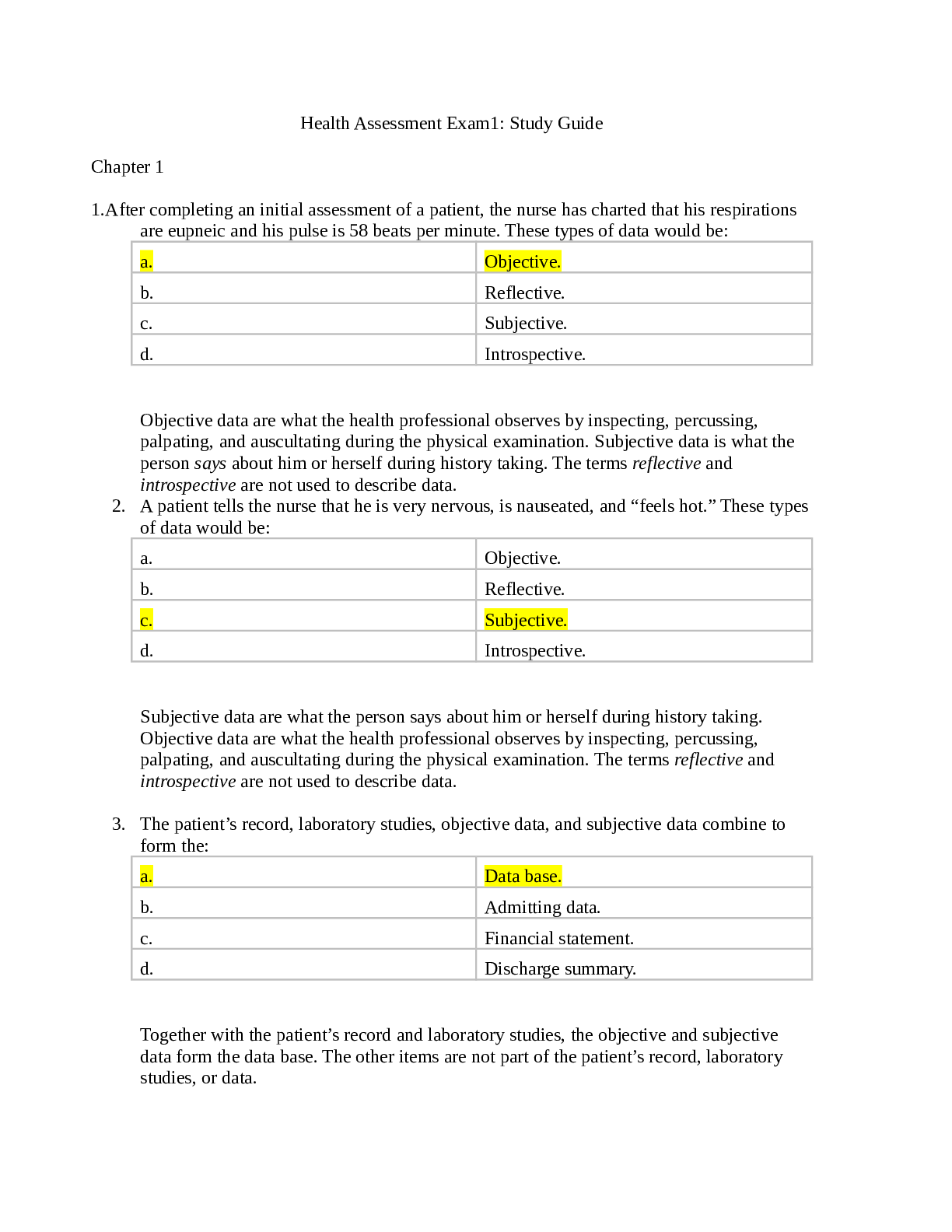

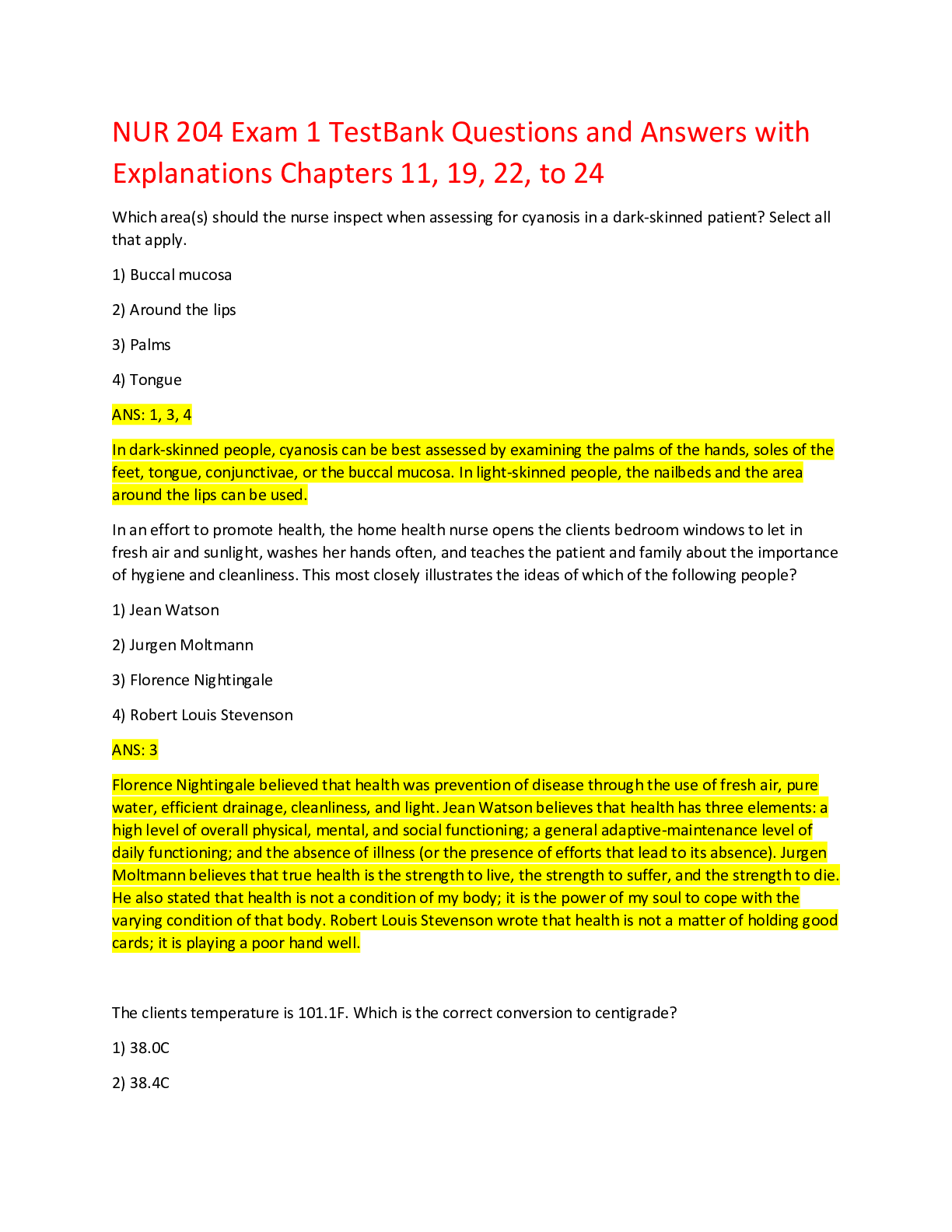
.png)
