Health Care > STUDY GUIDE > Health Assessment Exam 2 Study Guide latest 100%(2021/2022 graded A) (All)
Health Assessment Exam 2 Study Guide latest 100%(2021/2022 graded A)
Document Content and Description Below
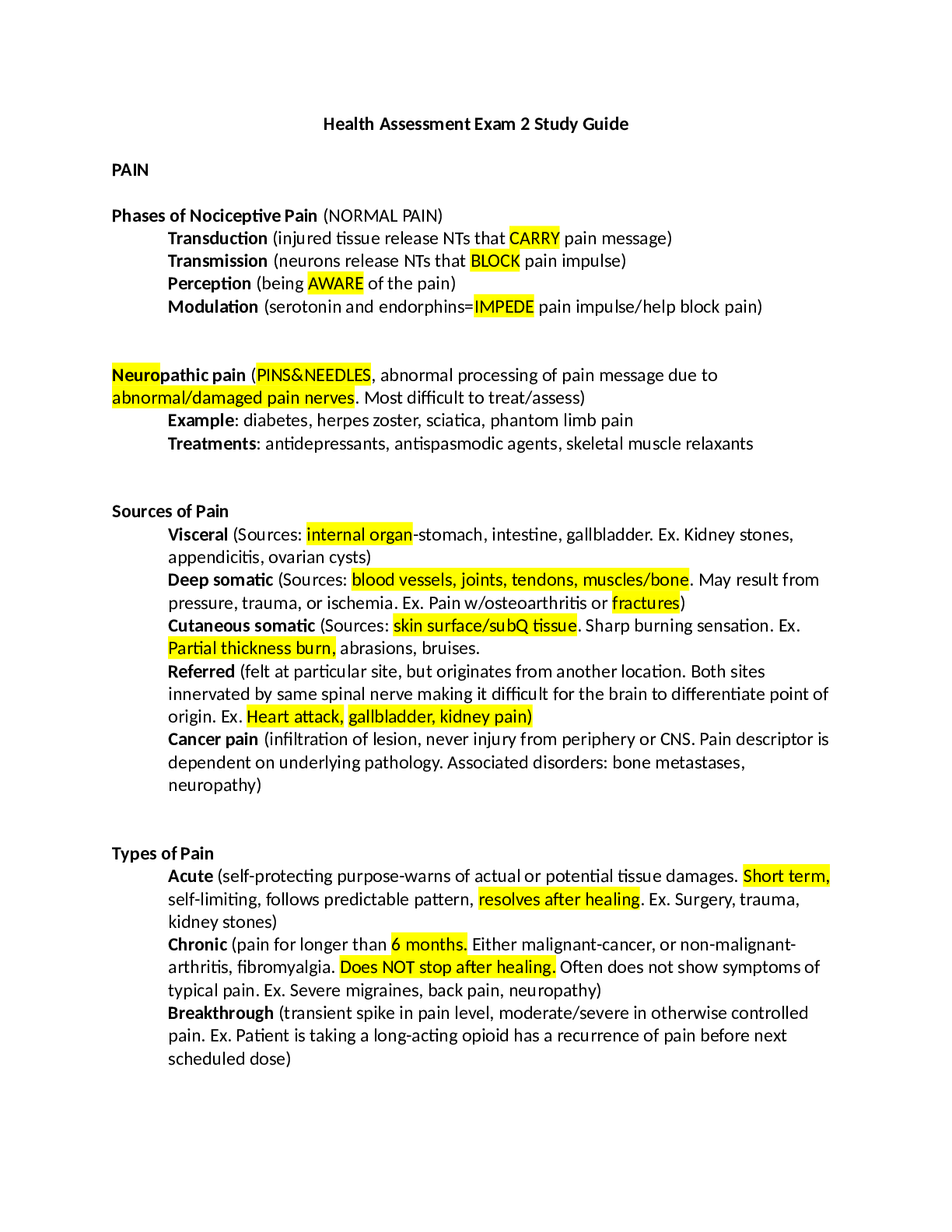
PAIN Phases of Nociceptive Pain (NORMAL PAIN) Transduction (injured tissue release NTs that CARRY pain message) Transmission (neurons release NTs that BLOCK pain impulse) Perception (being AWARE o... f the pain) Modulation (serotonin and endorphins=IMPEDE pain impulse/help block pain) Neuropathic pain (PINS&NEEDLES, abnormal processing of pain message due to abnormal/damaged pain nerves. Most difficult to treat/assess) Example: diabetes, herpes zoster, sciatica, phantom limb pain Treatments: antidepressants, antispasmodic agents, skeletal muscle relaxants Sources of Pain Visceral (Sources: internal organ-stomach, intestine, gallbladder. Ex. Kidney stones, appendicitis, ovarian cysts) Deep somatic (Sources: blood vessels, joints, tendons, muscles/bone. May result from pressure, trauma, or ischemia. Ex. Pain w/osteoarthritis or fractures) Cutaneous somatic (Sources: skin surface/subQ tissue. Sharp burning sensation. Ex. Partial thickness burn, abrasions, bruises. Referred (felt at particular site, but originates from another location. Both sites innervated by same spinal nerve making it difficult for the brain to differentiate point of origin. Ex. Heart attack, gallbladder, kidney pain) Cancer pain (infiltration of lesion, never injury from periphery or CNS. Pain descriptor is dependent on underlying pathology. Associated disorders: bone metastases, neuropathy) Types of Pain Acute (self-protecting purpose-warns of actual or potential tissue damages. Short term, self-limiting, follows predictable pattern, resolves after healing. Ex. Surgery, trauma, kidney stones) Chronic (pain for longer than 6 months. Either malignant-cancer, or non-malignantarthritis, fibromyalgia. Does NOT stop after healing. Often does not show symptoms of typical pain. Ex. Severe migraines, back pain, neuropathy) Breakthrough (transient spike in pain level, moderate/severe in otherwise controlled pain. Ex. Patient is taking a long-acting opioid has a recurrence of pain before next scheduled dose) Pain and Aging Adult (pain is a common experience for those 65+, but is NOT a normal aging process. Pain should not be tolerated or accepted) Cues: changes in dressing, walking, toileting, or involvement in activities. Slowness and rigidity may develop, fatigue may occur. Look for sudden onset of acute confusion, which may indicate poorly controlled pain. (you’ll need to rule out infection/adverse med reactions) Initial Pain Assessment (Where? When did pain start? What does your pain feel like-burning, stabbing, throbbing, aching? How much pain do you have now? What makes your pain better/worse? How does the pain limit functions/activities? What does this pain mean to you? PQRST method of Pain Assessment P-Provocation (cause of pain) Q-Quality (dull, ache, sharp, numb) R-Radiates or Refers S-Severity T-Time Pain Assessment Tools for Adults Pain rating scales (one-dimensional, rate pain 1-10) Verbal descriptor scales (use patient’s words to describe pain) Horizontal line scale (mark from “no pain” to “worst pain”) Nonverbal Behaviors of Pain Acute (guarding, grimacing, vocalization-moaning, agitation, diaphoresis-sweating, change in vital signs-tachycardia) Chronic (adapts over time, little indications that they’re in pain, bracing, rubbing, diminished activity, sighing, change in appetite) Assessing Pain in Patient with Dementia (communicate pain through their behavior: agitation, pacing, repetitive yelling) PAINAD scale (Pain Assessment IN Advanced Dementia: breathing independent of vocalization, negative vocalization, facial expression, body language, consolability) OLDER ADULT Changes of Aging Physiological (physical changes, reduced abilities, review notes on different body systems) Functional factors (ability to function day to day, change in function with ADLs, fear of becoming dependent) Cognitive factors (reduction in number of brain cells, cognitive impairments are NOT normal age-related changes; look for underlying causes) Psychosocial changes (retirement, social isolation, death, sexuality, housing and environment) Cognitive Disorders Delirium: ACUTE confused state Dementia: generalized impairment of intellectual functioning Depression: mood disturbance characterized by feeling of sadness and despair [Show More]
Last updated: 1 year ago
Preview 1 out of 12 pages
Reviews( 0 )
Document information
Connected school, study & course
About the document
Uploaded On
Apr 30, 2022
Number of pages
12
Written in

Additional information
This document has been written for:
Uploaded
Apr 30, 2022
Downloads
0
Views
47



.png)
.png)



.png)