WEEK 4 EDAPT NR 327 NOTES
Document Content and Description Below
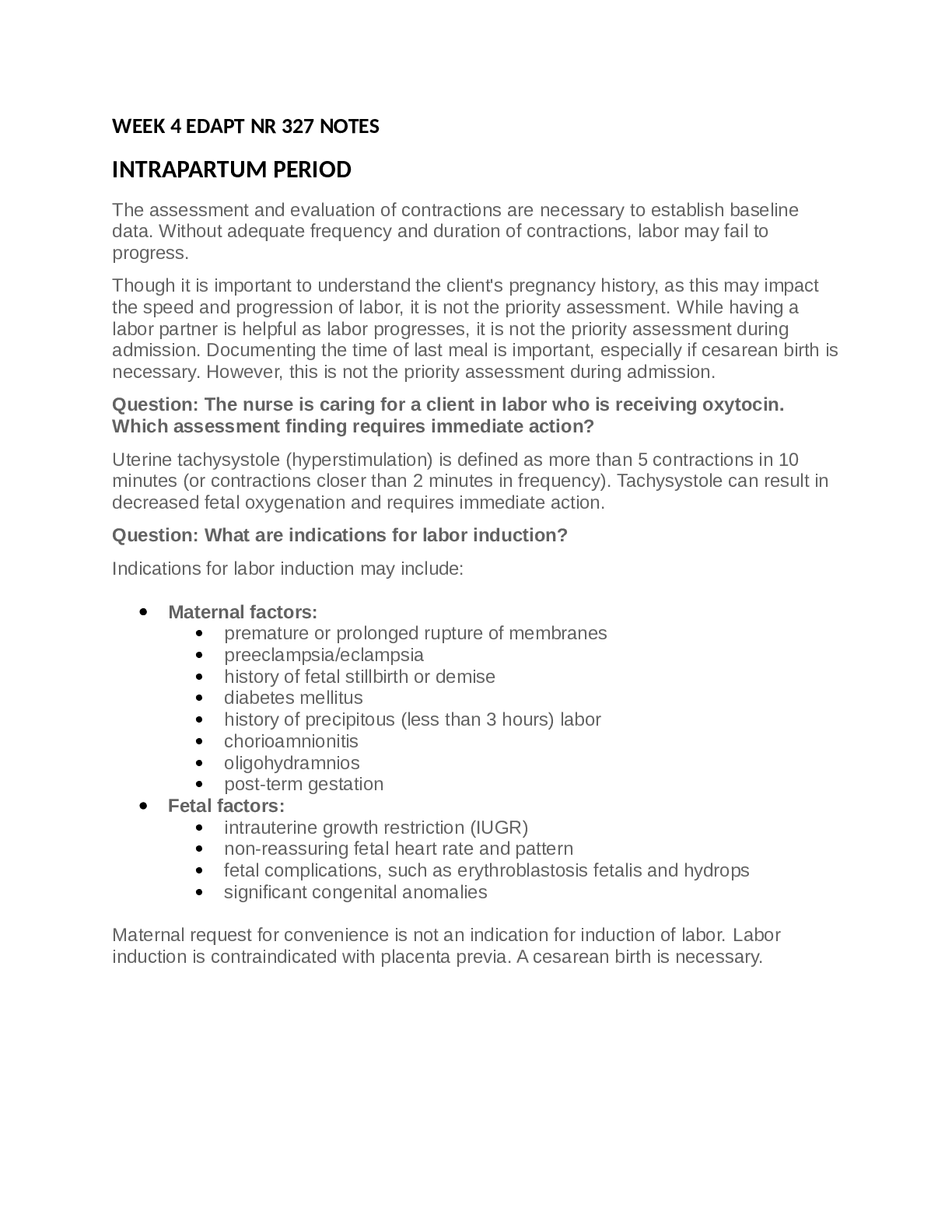
WEEK 4 EDAPT NR 327 NOTES INTRAPARTUM PERIOD The assessment and evaluation of contractions are necessary to establish baseline data. Without adequate frequency and duration of contractions, labor m... ay fail to progress. Though it is important to understand the client's pregnancy history, as this may impact the speed and progression of labor, it is not the priority assessment. While having a labor partner is helpful as labor progresses, it is not the priority assessment during admission. Documenting the time of last meal is important, especially if cesarean birth is necessary. However, this is not the priority assessment during admission. Question: The nurse is caring for a client in labor who is receiving oxytocin. Which assessment finding requires immediate action? Uterine tachysystole (hyperstimulation) is defined as more than 5 contractions in 10 minutes (or contractions closer than 2 minutes in frequency). Tachysystole can result in decreased fetal oxygenation and requires immediate action. Question: What are indications for labor induction? Indications for labor induction may include: Maternal factors: premature or prolonged rupture of membranes preeclampsia/eclampsia history of fetal stillbirth or demise diabetes mellitus history of precipitous (less than 3 hours) labor chorioamnionitis oligohydramnios post-term gestation Fetal factors: intrauterine growth restriction (IUGR) non-reassuring fetal heart rate and pattern fetal complications, such as erythroblastosis fetalis and hydrops significant congenital anomalies Maternal request for convenience is not an indication for induction of labor. Labor induction is contraindicated with placenta previa. A cesarean birth is necessary. INTRAPARTUM TERMINOLOGY: SVE - Sterile vaginal examination is an assessment performed by RN to determine cervical dilation, effacement, and fetal station. PROM - Premature rupture of membranes is the spontaneous rupture of the membranes before the onset of labor at any gestational age. Effacement - Effacement is the shortening and thinning of the cervix during the first stage of labor - the drawing up of the internal os and the cervical canal into the uterine side walls. Measured as a percentage: 0% is approximately 1 cm thick; 100% is paper thin. Engagement - The ischial spines are the narrowest diameter through which the fetus must pass; designated as 0 station. When the presenting part reaches 0 station, the fetus is said to be engaged in the pelvis. NST - NST stands for nonstress test. Reactive (normal) NST = In 20 minutes, at least 2 accelerations in fetal heart rate >15 bpm above baseline for >15 seconds AROM: Augmented (also called artificial) rupture of membranes Cephalic Presentation: Fetus positioned head down; most common fetal presentation Dilation: Progressive opening of cervix caused by uterine contractions; 0–10 cm Effacement: Shortening and thinning of the cervix within stage one of labor EFM: Electronic fetal monitoring Engagement: Fetal presenting part reaches true pelvis FHR: Fetal heart rate Fundus: Upper aspect of the uterus Intrapartum: Onset of labor to birth Lightening: Descent of fetal presenting part into the pelvic cavity, often 38 weeks gestation (or 2 weeks before labor onset in primiparas) NST: Nonstress test; fetal assessment for well-being, (2) accelerations documented with 15 bpm above baseline × 15 seconds in length minimum = (+) NST PROM: Premature rupture of membranes; no contraction or no dilation noted, but SROM occurred SROM: Spontaneous rupture of membranes Station: Relation of the presenting part to the ischial spines of maternal pelvis SVE: Assessment performed by RN to determine cervical dilation, station, and effacement. Childbirth and associated intimate medical interventions may trigger feelings of anxiety and fear in women who are survivors of sexual abuse. Nurses should provide emotional support, helping the client to associate uncomfortable experiences with the birth of a child, instead of past abuse. Providing information and privacy while allowing client control may reduce anxiety and fear. Laboring women who are survivors of sexual abuse need to be kept continually informed of labor progress in order to avoid stress and anxiety. Childbirth preparation classes: There are many different types of childbirth preparation techniques taught to clients. Though all methods provide instruction on pain management techniques, each has unique aspects. Some of the common classes offered are: Dick-Read Childbirth Education focuses on alleviating the fear of childbirth through education and the pain through relaxation and breathing techniques. Bradley Childbirth Education teaches abdominal breathing to increase relaxation and emphasizes the avoidance of medications and interventions. Lamaze Childbirth Education teaches concentration and relaxation to decrease contraction pain. FETAL HEART RATE AND PATTERN: The primary and most reliable way to assess the status of a fetus is to monitor the fetal heart rate and pattern. This can be done using continuous electronic fetal monitoring (EFM) or intermittently using an electronic doppler. Assessing the fetal heart rate and pattern is a priority during admission. The normal range for fetal heart rate is between 110 and 160 bpm. The pattern may include accelerations and early decelerations. However, variable and late decelerations are ominous and should be evaluated further. The frequency of fetal monitoring during labor is determined by the client’s level of risk. During active labor, the nurse should plan to monitor at least every 30 minutes. When assessing the fetal heart rate and pattern, consider these questions: What is the baseline fetal heart rate (FHR)? What is the FHR variability? Are accelerations in the FHR present? Does the FHR meet reactive non-stress test criteria? Are any decelerations present? If yes, what type of deceleration is occurring? Are interventions needed? NOTE: Nurses who care for women during childbirth are legally responsible for correctly interpreting the fetal heart rate pattern, implementing appropriate nursing actions based on that pattern, and documenting the outcome of those actions. Contraction pattern: External electronic fetal monitoring (EFM) does not measure uterine tone unless an internal monitor is in place, so the nurse palpates the abdomen to assess uterine contraction strength manually. The palpable tone (strength) of contractions is described as mild, moderate, or strong. When palpating the fundus, consider these questions: What is the intensity (strength) of the contraction? What is the intensity of the resting period after the contraction ends? The tone of the resting period should feel soft, like the upper lip. Frequency, duration, onset, and regularity of contractions are assessed as part of the intrapartum admission nursing assessment. When assessing contractions, the nurse should consider these questions: What is the frequency of the contractions? Frequency is the time between the beginning of one contraction and the beginning of the next contraction. What is the duration of the contractions? Duration is the time from the beginning of the contraction to the end of the same contraction. While evaluating contractions, the nurse should ask the client: What is the pain level of the contractions? What is a tolerable level of pain for the client? Vital signs: Vital signs should be monitored frequently during labor. The nurse should plan on hourly assessments for blood pressure, pulse, and respirations unless complications or analgesia warrant increased frequency. Temperature will be monitored every 4 hours until the membranes are ruptured, then hourly. Abnormal parameters compared to the client's baseline should be reported to the healthcare provider and may change the frequency of evaluations. Pain level should be monitored continuously as increased pain can elevate both blood pressure and pulse rate. AMNIOTIC MEMRANES: Amniotic membranes are assessed before the initial cervical examination to accurately determine if amniotic fluid is leaking. Yellow nitrazine paper may be used to detect amniotic fluid, which has a basic pH. A blue color change is indicative of the presence of amniotic fluid. No color change indicates lack of amniotic fluid (so no membrane rupture). Ask the client these questions: Has your water broken? What time did it break? What did the fluid look like? About how much fluid did you lose? Was it a big gush or a small trickle? If the amniotic membranes are ruptured, assess, and document the time of rupture, amount, color, and odor of fluid (think of TACO). T = Time that the amniotic membrane ruptured A = Amount of amniotic fluid that came out C = Color of the leaked amniotic fluid clear—normal greenish meconium yellow/cloudy—potential infection, called chorioamnionitis O = Odor of the leaked amniotic fluid odorless—normal foul/strong odor—potential infection CERVICAL EXAMINATION AND DILATATION: Cervical dilation is a key nursing assessment for determining if the woman is in true labor. If the facility’s policy permits, a sterile vaginal exam (SVE) is often performed by the nurse as part of the intrapartum admission and ongoing assessment, which is to determine: cervical dilation (the widening of the cervical opening) cervical effacement (shortening and thinning of the cervix) fetal station (the relationship of the presenting part to the ischial spines in the maternal pelvis) A baseline sterile cervical exam, in conjunction with other assessment f [Show More]
Last updated: 1 year ago
Preview 1 out of 42 pages
Instant download
Buy this document to get the full access instantly
Instant Download Access after purchase
Add to cartInstant download
Reviews( 0 )
Document information
Connected school, study & course
About the document
Uploaded On
Aug 23, 2022
Number of pages
42
Written in

Additional information
This document has been written for:
Uploaded
Aug 23, 2022
Downloads
0
Views
36
.png)
.png)