HESI EXAM 20 POINTS
Document Content and Description Below
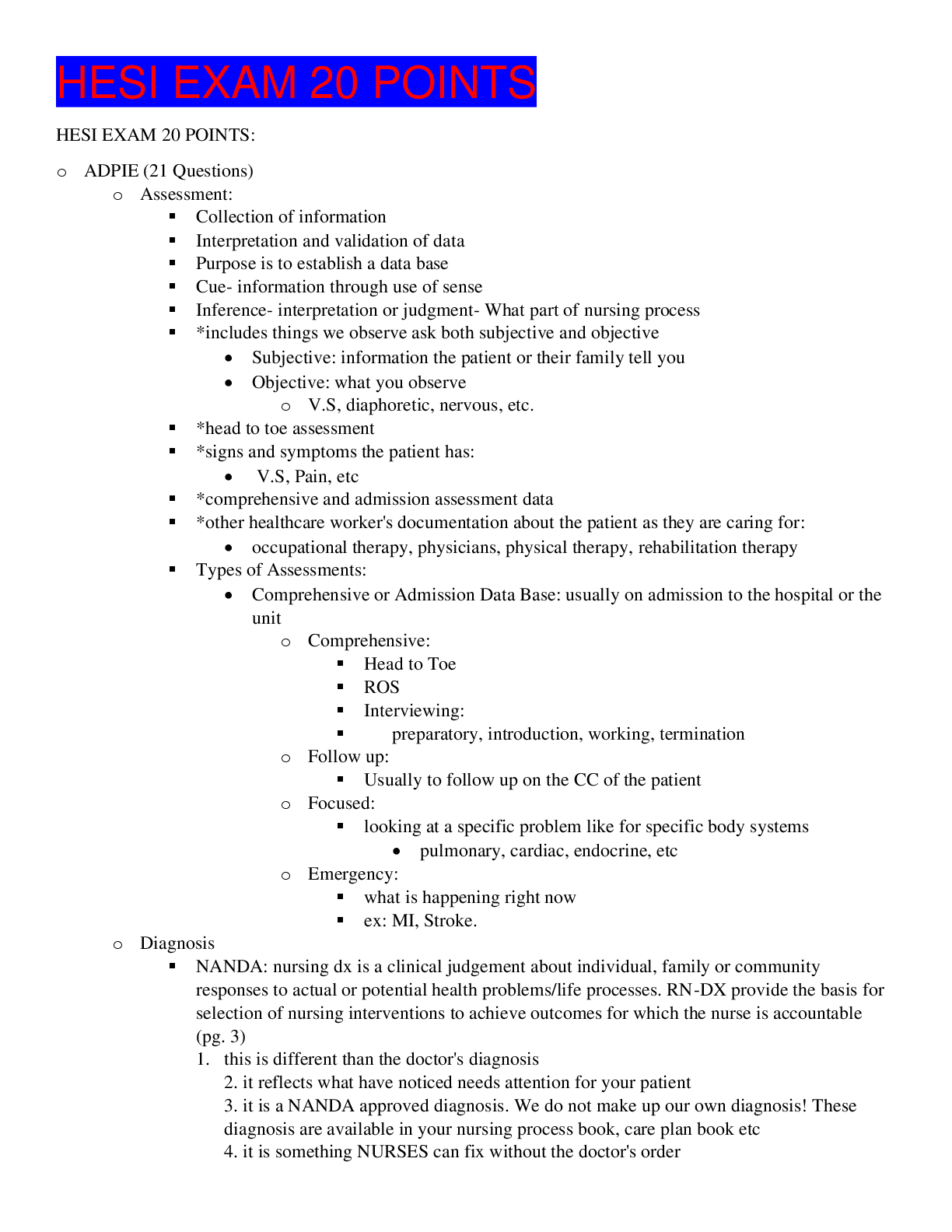
HESI EXAM 20 POINTS HESI EXAM 20 POINTS: o ADPIE (21 Questions) o Assessment: Collection of information Interpretation and validation of data Purpose is to establish a data base �... � Cue- information through use of sense Inference- interpretation or judgment- What part of nursing process *includes things we observe ask both subjective and objective • Subjective: information the patient or their family tell you • Objective: what you observe o V.S, diaphoretic, nervous, etc. *head to toe assessment *signs and symptoms the patient has: • V.S, Pain, etc *comprehensive and admission assessment data *other healthcare worker's documentation about the patient as they are caring for: • occupational therapy, physicians, physical therapy, rehabilitation therapy Types of Assessments: • Comprehensive or Admission Data Base: usually on admission to the hospital or the unit o Comprehensive: Head to Toe ROS Interviewing: preparatory, introduction, working, termination o Follow up: Usually to follow up on the CC of the patient o Focused: looking at a specific problem like for specific body systems • pulmonary, cardiac, endocrine, etc o Emergency: what is happening right now ex: MI, Stroke. o Diagnosis NANDA: nursing dx is a clinical judgement about individual, family or community responses to actual or potential health problems/life processes. RN-DX provide the basis for selection of nursing interventions to achieve outcomes for which the nurse is accountable (pg. 3) 1. this is different than the doctor's diagnosis 2. it reflects what have noticed needs attention for your patient 3. it is a NANDA approved diagnosis. We do not make up our own diagnosis! These diagnosis are available in your nursing process book, care plan book etc 4. it is something NURSES can fix without the doctor's order 5. we think about our patient's strengths and weaknesses 6. we do take into account the doctor's diagnosis as well as what treatment orders the doctor has given us in the patient chart. We look at information collaboratively from other health care workers taking care of our patient 2. Problem 3. Etiology 4. Signs and Symptoms 5. Critical thinking 6. PROBLEM R/T ETIOLOGY/CAUSE AEB S/SX 7. How to form a basis for the DX: a. Data clustering- defining characteristics b. Diagnosis is based on certain clinical criteria c. Consider the patient’s health patterns and interpret the information d. Apply to more than one diagnosis 8. Types a. Actual- three parts i. PROBLEM R/T ETIOLOGY/CAUSE AEB S/SX ii. EX: alteration of bowel movements related to food poisoning as evidence by 5 watery and loose stools. b. Risk for i. Ex: pt could be elderly and have cognitive issues. Because of this, they are AT RISK for falling and hitting their head, etc. ii. Ex: Risk for falls related to cognitive impairment as evidence by unable to perform ADL’s. c. Health promotion i. Health-Promotion Nursing Diagnosis. A clinical judgment concerning motivation and desire to increase well-being and to actualize human health potential. These responses are expressed by a readiness to enhance specific health behaviors, and can be used in any health state. ii. Ex: readiness to enhance nutrition or readiness to perform ADL’s with minimal supervision. 9. o Planning: determines and prioritize outcomes of care. Includes client, SO, and health care team in setting outcomes. Develop and modify plan for delivery of pt care. EX: • what is going to kill your patient first! (ABC’s) That is the FIRST PRIORITY! • Second priority is risks/safety can they harm themselves or others? Are they at risk for falls, aspirations etc? Is there a carpet on the ground that they can trip on? Prioritization: • Maslows Hierarchy of Needs: Need Definition Nursing Implication Physiological Biological need for food, shelter, water, sleep, oxygen and sexual expression The priority in biological need is breathing! Pt needs are associated with physiologic integrity. If you were asked to ID the MOST IMPORTANT action you would identify needs associated with physiologic integrity as the most important nursing action. (breathing for example) Safety Avoiding harm: attaining security, order and physical safety. Ensuring that the pts environment is safe is a priority. (ex: getting rid of throw rugs so the pt doesn’t trip and fall). The first priority is safety then coping! Love and Belonging & Esteem and Recognition - Giving and receiving affection, companionship and identification c/ a group - Self-esteem and respect of others, success in work prestige. These needs are important but NOT AS IMPORTANT as physiologic and safety! More important for a patient to be breathing than to it is to have them part of a support group. Assisting a patient in being part of a support group is more important than the patient developing self-esteem. KEY the sense of belonging would come first and such a sense might help in developing self-esteem. Self-Actualization & Aesthetic - Fulfillment of unique potential - Search for beauty and spiritual goals It is important to understand these last two concepts in that they can help with health promotion and maintenance such as continued growth and development and self-care. This can involve psychosocial integrity. Usually we are not asked about this on NCLEX because this doesn’t involve the first two concepts. - Planning involves: o Patient centered o Short-term goals The pt will be stabilized with his blood pressure o Long-term goals The pt will have readiness to maintain HTN with medication and diet. o Role of the patient Involve them in their care! o Outcomes: SMART goals, which is an acronym that stands for specific, measurable, attainable, realistic and timely short-and long-term goals for the patient Nursing-sensitive patient outcomes Patient-centered Singular goal or outcome Observable Measurable Time-limited Mutual factors Realistic Bases of interventions and evaluation o Implementation: Begin doing what I said I would do I will state that I am doing it in my plan of care or care plan Independent Dependent Collaborative • As a team with doctors, nurses, MA, pharmacy, etc. ………………………………CONTINUED…………………………………. [Show More]
Last updated: 1 year ago
Preview 1 out of 91 pages
Instant download
Buy this document to get the full access instantly
Instant Download Access after purchase
Add to cartInstant download
Reviews( 0 )
Document information
Connected school, study & course
About the document
Uploaded On
Feb 07, 2021
Number of pages
91
Written in

Additional information
This document has been written for:
Uploaded
Feb 07, 2021
Downloads
0
Views
39