*NURSING > STUDY GUIDE > NR507 / NR 507 / NURS 507/ NURS507 FINAL EXAM STUDY GUIDE. (All)
NR507 / NR 507 / NURS 507/ NURS507 FINAL EXAM STUDY GUIDE.
Document Content and Description Below
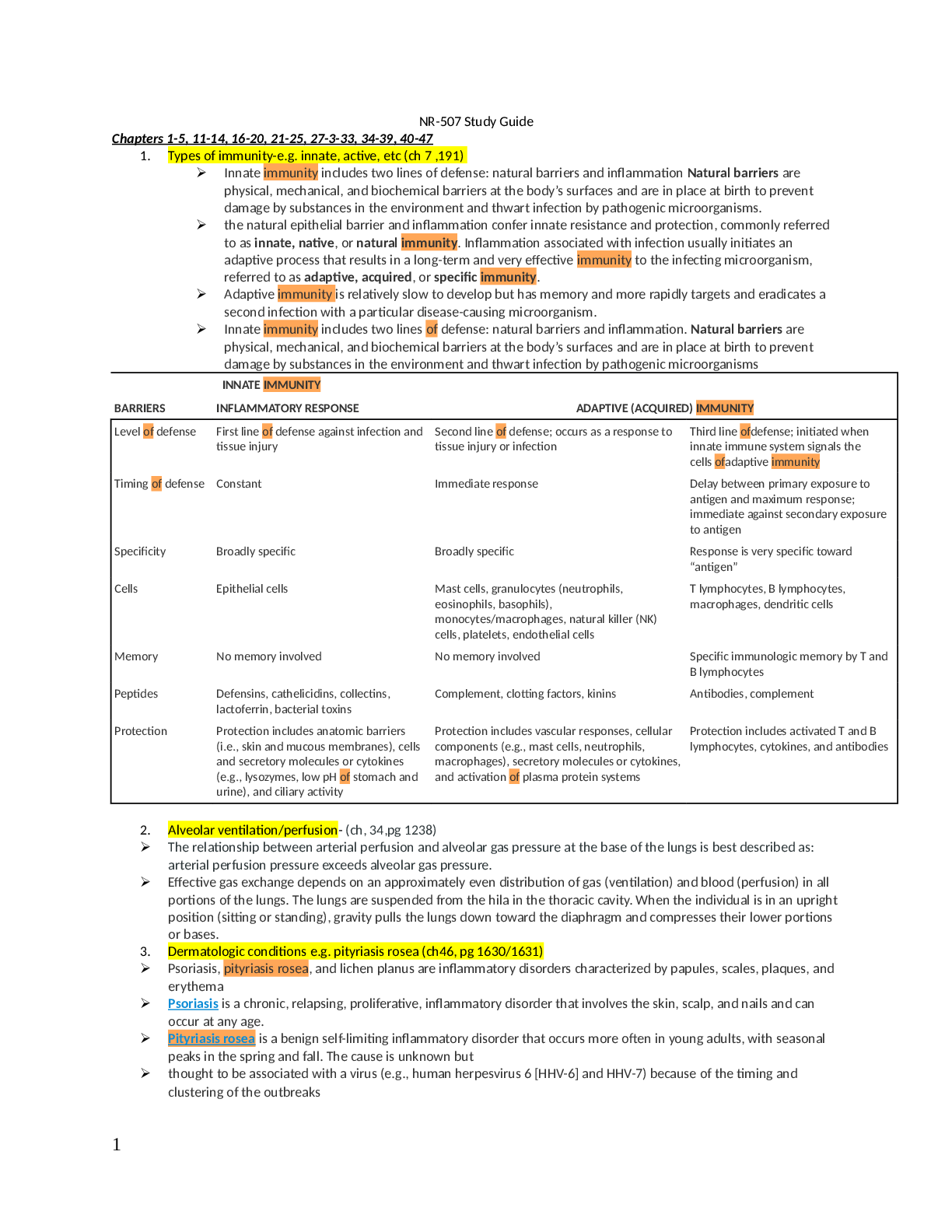
NR-507 Study Guide Chapters 1-5, 11-14, 16-20, 21-25, 27-3-33, 34-39, 40-47 1. Types of immunity-e.g. innate, active, etc (ch 7 ,191) ➢ Innate immunity includes two lines of defense: natural barr... iers and inflammation Natural barriers are physical, mechanical, and biochemical barriers at the body’s surfaces and are in place at birth to prevent damage by substances in the environment and thwart infection by pathogenic microorganisms. ➢ the natural epithelial barrier and inflammation confer innate resistance and protection, commonly referred to as innate, native, or natural immunity. Inflammation associated with infection usually initiates an adaptive process that results in a long-term and very effective immunity to the infecting microorganism, referred to as adaptive, acquired, or specific immunity. ➢ Adaptive immunity is relatively slow to develop but has memory and more rapidly targets and eradicates a second infection with a particular disease-causing microorganism. ➢ Innate immunity includes two lines of defense: natural barriers and inflammation. Natural barriers are physical, mechanical, and biochemical barriers at the body’s surfaces and are in place at birth to prevent damage by substances in the environment and thwart infection by pathogenic microorganisms BARRIERS INNATE IMMUNITY INFLAMMATORY RESPONSE ADAPTIVE (ACQUIRED) IMMUNITY Level of defense First line of defense against infection and tissue injury Second line of defense; occurs as a response to tissue injury or infection Third line ofdefense; initiated when innate immune system signals the cells ofadaptive immunity Timing of defense Constant Immediate response Delay between primary exposure to antigen and maximum response; immediate against secondary exposure to antigen Specificity Broadly specific Broadly specific Response is very specific toward “antigen” Cells Epithelial cells Mast cells, granulocytes (neutrophils, eosinophils, basophils), monocytes/macrophages, natural killer (NK) cells, platelets, endothelial cells T lymphocytes, B lymphocytes, macrophages, dendritic cells Memory No memory involved No memory involved Specific immunologic memory by T and B lymphocytes Peptides Defensins, cathelicidins, collectins, lactoferrin, bacterial toxins Complement, clotting factors, kinins Antibodies, complement Protection Protection includes anatomic barriers (i.e., skin and mucous membranes), cells and secretory molecules or cytokines (e.g., lysozymes, low pH of stomach and urine), and ciliary activity Protection includes vascular responses, cellular components (e.g., mast cells, neutrophils, macrophages), secretory molecules or cytokines, and activation of plasma protein systems Protection includes activated T and B lymphocytes, cytokines, and antibodies 2. Alveolar ventilation/perfusion- (ch, 34,pg 1238) ➢ The relationship between arterial perfusion and alveolar gas pressure at the base of the lungs is best described as: arterial perfusion pressure exceeds alveolar gas pressure. ➢ Effective gas exchange depends on an approximately even distribution of gas (ventilation) and blood (perfusion) in all portions of the lungs. The lungs are suspended from the hila in the thoracic cavity. When the individual is in an upright position (sitting or standing), gravity pulls the lungs down toward the diaphragm and compresses their lower portions or bases. 3. Dermatologic conditions e.g. pityriasis rosea (ch46, pg 1630/1631) ➢ Psoriasis, pityriasis rosea, and lichen planus are inflammatory disorders characterized by papules, scales, plaques, and erythema ➢ Psoriasis is a chronic, relapsing, proliferative, inflammatory disorder that involves the skin, scalp, and nails and can occur at any age. ➢ Pityriasis rosea is a benign self-limiting inflammatory disorder that occurs more often in young adults, with seasonal peaks in the spring and fall. The cause is unknown but ➢ thought to be associated with a virus (e.g., human herpesvirus 6 [HHV-6] and HHV-7) because of the timing and clustering of the outbreaks ➢ Pityriasis rosea begins as a single lesion known as a herald patch that is circular, demarcated, and salmon-pink; is approximately 3 to 4 cm in diameter; and is usually located on the trunk ➢ Lichen planus (LP) is a benign, autoimmune inflammatory disorder of the skin and mucous membranes with multiple clinical variations. The cause is unknown, but T cells, adhesion molecules, inflammatory cytokines, perforin, and antigen-presenting cells are involved.The infiltrate of T cells mediates immunoreactivity against basal layer keratinocytes, which have altered surface antigens and adhesion molecules ➢ LP is also linked to hepatitis C virus. Some individuals develop lichenoid lesions after exposure to drugs or film- processing chemicals. The age of onset is usually between 30 and 70 years. The disorder begins with flat purple, polygonal, pruritic, nonscaling papules 2 to 4 mm in size, usually located on the wrists, ankles, lower legs, and genitalia ➢ New lesions are pale pink and evolve into a dark violet. Persistent lesions may be thickened and red, forming hypertrophic LP. Oral lesions (oral lichen planus) appear as lacy white rings that must be differentiated from leukoplakia or oral candidiasis and they may be precancerous lesions 4. Croup (C 36,pg 1294)- ➢ Croup illnesses can be divided into two categories: (1) acute laryngotracheobronchitis (croup) and (2) spasmodic croup. Diphtheria can be considered a croup illness but is now rare because of vaccinations. Croup illnesses are all characterized by infection and obstruction of the upper airways. ➢ Croup is an acute laryngotracheobronchitis and most commonly occurs in children from 6 months to 3 years of age, with peak incidence at 2 years of age ➢ The incidence of croup is highest in late autumn and winter, corresponding to the parainfluenza and RSV seasons, respectively. Croup is more common in boys than girls. In a significant portion of affected children, croup is a recurrent problem during childhood, and there is a family history of croup in about 15% of cases ➢ Chickenpox (varicella) and herpes zoster (shingles) are produced by the varicella-zoster virus (VZV). VZV is a complex herpes group deoxyribonucleic acid (DNA) virus. The incubation period is 10 to 27 days, averaging 14 days. Productive infection occurs within keratinocytes such that the vesicular lesions occur in the epidermis, and an inflammatory infiltrate is often present 5. Types of anemia (ch 28,pg 987-1002) ➢ anemia is a reduction in the total number of erythrocytes in the circulating blood or a decrease in the quality or quantity of hemoglobin. Anemias commonly result from (1) impaired erythrocyte production, (2) blood loss (acute or chronic), (3) increased erythrocyte destruction, or (4) a combination of these three factors. ➢ Pernicious anemia (PA), the most common type of megaloblastic anemia, is caused by vitamin B12deficiency, which is often associated with the end stage of type A chronic atrophic (congenital or autoimmune) gastritis. PA results from inadequate vitamin B12 absorption because of autoantibodies against the B12transporter IF ➢ Folate (folic acid) is an essential vitamin for RNA and DNA synthesis within the maturing erythrocyte. Folates are coenzymes required for the synthesis of thymine and purines (adenine and guanine) and the conversion of homocysteine to methionine. Deficient production of thymine, in particular, affects cells undergoing rapid division (e.g., bone marrow cells undergoing erythropoiesis). Humans are totally dependent on dietary intake to meet the daily requirement of 50 to 200 mcg/day. Folate deficiency anemia is caused by inadequate dietary intake of folate. Both anemias respond to replacement therapy. ➢ The microcytic-hypochromic anemias are characterized by abnormally small erythrocytes that contain abnormally reduced amounts of hemoglobin ➢ Microcytic-hypochromic anemia can result from (1) disorders of iron metabolism, (2) disorders ofporphyrin and heme synthesis, or (3) disorders of globin synthesis. Specific disorders include iron deficiency anemia, side roblastic anemia, and thalassemia ➢ Iron deficiency anemia (IDA) is the most common type of anemia worldwide, occurring in both developing and developed countries and affecting as many as one fifth of the world population. Certain populations are at high risk for developing hypoferremia and IDA and include individuals living in poverty, women of childbearing age, and children. Iron deficiency in children is associated with numerous adverse health-related manifestations, especially cognitive impairment, which may be irreversible ➢ Sideroblastic anemias (SAs) are a heterogeneous group of disorders characterized by anemia of varying severity caused by a defect in mitochondrial heme synthesis.SA is characterized by the presence of ringed side roblasts within the bone marrow. SA results from defects in mitochondrial metabolism leading to ineffective iron uptake and dysfunctional heme synthesis. The characteristic cell in the bone marrow, a ringed sideroblast, is an erythroblast containing iron granules arranged around the nucleus. SAs may be hereditary or acquired, and treatment varies depending on the cause. ➢ Normocytic-normochromic anemias (NNAs) are characterized by erythrocytes that are relatively normal in size and hemoglobin content but insufficient in number. These anemias have no common etiology, pathologic mechanisms, or morphologic characteristics. They are less frequent than macrocytic-normochromic and microcytic-hypochromic anemias. ➢ NNAs include five distinct groups: aplastic (damage to bone marrow erythropoiesis); posthemorrhagic (acute blood loss); acquired hemolytic (immune destruction of erythrocytes); hereditary hemolytic, such as sickle cell (destruction by eryptosis); and anemia of chronic inflammation (multiple causes) ➢ Macrocytic-normochromic, or megaloblastic-normochromic, anemias are characterized by larger than normal erythrocytes with normal levels of hemoglobin. They most commonly are caused by deficiency of vitamin B12 (PA) or folate. ➢ Aplastic anemia (AA) is a critical condition characterized by pancytopenia, a reduction or absence of all three blood cell types, resulting from failure or suppression of bone marrow to produce adequate amounts of blood cells ➢ Posthemorrhagic anemia is a normocytic-normochromic anemia caused by acute blood loss. Initial manifestations of this event depend on the severity of blood loss. If blood loss is severe, the significant manifestations are related to loss of blood volume rather than loss of hemoglobin. ➢ The predominant event in hemolytic anemias is premature accelerated destruction of erythrocytes, either episodically or continuously. The consequences of the anemia are elevated levels of erythropoietin to induce accelerated production of erythrocytes and an increase in the products of hemoglobin catabolism. ➢ Anemia of chronic disease (ACD) is a mild to moderate anemia resulting from decreased erythropoiesis in individuals with conditions of chronic systemic disease or inflammation (e.g., infections, cancer, and chronic inflammatory or autoimmune diseases). These conditions include acquired immunodeficiency disease (AIDS), malaria (particularly that caused by Plasmodium falciparum), rheumatoid arthritis, systemic lupus erythematosus (SLE), acute and chronic hepatitis, and chronic renal failure (a condition in which almost all affected individuals are anemic) ➢ This form of anemia also is commonly noted in the presence of congestive heart failure (CHF). The anemia develops after 1 to 2 months of disease activity. The initial severity is related to that of the underlying disorder but, although persistent, it usually does not progress. Individuals may be asymptomatic, or the anemia may be a coincidental clinical finding. 6. The inflammatory process upon injury ( ch 7) ➢ The inflammatory response is initiated upon tissue injury or when PAMPs are recognized by PRRs on cells of the innate immune system. ➢ There are two types of human defense mechanisms: innate resistance or immunity conferred by natural barriers and the inflammatory response; and the adaptive (acquired) immune system. ➢ Many different types of cells are involved in the inflammatory process including mast cells, granulocytes (neutrophils, eosinophils, basophils), monocytes/macrophages, NK cells and lymphocytes, and cellular fragments (platelets). ➢ The cells of the innate immune system secrete many biochemical mediators that are responsible for the vascular changes associated with inflammation and for modulating the localization and activities of other inflammatory cells. The mediators include histamine, chemotactic factors, leukotrienes, prostaglandins, and platelet-activating factor. 7. GI symptoms resulting in heart burn( ch 41, pg 1429- 1466) ➢ The clinical manifestations of (GERD) reflux esophagitis are heartburn from acid regurgitation, chronic cough, asthma attacks and laryngitis. ➢ Heartburn also may be experienced as chest pain, which requires ruling out cardiac ischemia. ➢ Hiatal hernias are often asymptomatic. Generally, a wide variety of symptoms develop later in life and are associated with other gastrointestinal disorders, including GERD. Manifestations of the various types of hiatal hernia are difficult to distinguish. Symptoms include heartburn, regurgitation, dysphagia, and epigastric pain ➢ Early stages of esophageal carcinoma are asymptomatic. The two main manifestations of esophageal carcinoma are chest pain and dysphagia. The most common type of pain is heartburn (pyrosis). It is initiated by eating spicy or highly seasoned foods and by lying down. 8. Pulmonary terminology such as dyspnea, orthopnea, etc ( ch 35, pg 1249) ➢ Dyspnea is a feeling of breathlessness and increased respiratory effort. ➢ Orthopnea is dyspnea when a person lies flat ➢ Paroxysmal nocturnal dyspnea occurs at night and requires the person to sit or stand for relief. 9. Complications of gastric resection surgery (c 41, pg 1439) ➢ Weight loss often follows gastric resection but stabilizes within 3 months. Inadequate food intake is a common cause because many individuals cannot tolerate the osmotic effect of carbohydrates or a normal-size meal. Foods may be poorly absorbed because the stomach is less able to mix, churn, and break down food particles. Abdominal pain, vomiting, diarrhea, and malabsorption of fats also contribute to weight loss. In the case of bariatric surgery for extreme obesity, weight loss is the intended outcome. 10. Dermatology terminology-macules, nevi, etc ( ch 46, pg 1620) ➢ Macule- A flat, circumscribed area that is a change in the color of the skin; less than 1 cm in diameter. Freckles, flat moles (nevi), petechiae, measles, scarlet fever ➢ Papule - An elevated, firm, circumscribed area less than 1 cm in diameter, Wart (verruca), elevated moles, lichen planus, fibroma, insect bite ➢ Patch - A flat, nonpalpable, irregular-shaped macule more than 1 cm in diameter, Vitiligo, port-wine stains, mongolian spots, café-au-lait spots ➢ Plaque- Elevated, firm, and rough lesion with flat top surface greater than 1 cm in diameter, Psoriasis, seborrheic and actinic keratosis ➢ Wheal - Elevated, irregular-shaped area of cutaneous edema; solid, transient; variable diameter, Insect bites, urticaria, allergic reaction ➢ Nodule- Elevated, firm, circumscribed lesion; deeper in dermis than a papule; 1-2 cm in diameter, Erythema nodosum, lipomas ➢ Tumor- Elevated, solid lesion; may be clearly demarcated; deeper in dermis; greater than 2 cm in diameter, Neoplasms, benign tumor, lipoma, neurofibroma, hemangioma ➢ Vesicle- Elevated, circumscribed, superficial, does not extend into dermis; filled with serous fluid; less than 1 cm in diameter, Varicella (chickenpox), herpes zoster (shingles), herpes simplex ➢ Bulla - Vesicle greater than 1 cm in diameter, Blister, pemphigus vulgaris ➢ Pustule- Elevated, superficial lesion; similar to a vesicle but filled with purulent fluid, Impetigo, acne ➢ Cyst - Elevated, circumscribed, encapsulated lesion; in dermis or subcutaneous layer; filled with liquid or semisolid material, Sebaceous cyst, cystic acne ➢ Telangiectasia - Fine (0.5-1.0 mm), irregular red lines produced by capillary dilation; can be associated with acne rosacea (face), venous hypertension (spider veins in legs), systemic sclerosis, or developmental abnormalities (port- wine birthmarks), Telangiectasia in rosacea 11. Chicken pox ( c 46,pg 1659) ➢ an infectious viral disease that is spread by direct contact or through the air by coughing or sneezing; it causes a blister-like rash that first affects the face and trunk and then can spread over the rest of the body; symptoms include severe itching, fatigue, and fever. 12. Maternal immune system- (ch 8 & 9, pg 259-276) ➢ The human neonate has a poorly developed immune response, particularly in the production of IgG. The fetus and neonate are protected in utero and during the first few postnatal months by maternalantibody that was actively transported across the placenta ➢ The maternal antibodies are slowly catabolized after birth until they disappear altogether by about 10 months of age. The neonate begins producing IgG at birth, and the child’s antibodies reach protective levels after about 6 months of age. ➢ The mother’s immune system produces the antibody, but because her cells do not express the target antigen, she has no symptoms of the disease. ➢ Neonatal alloimmune disease may be secondary to maternal autoimmune diseases in which the mother produces an maternal self-antigens that are found on fetal cells as well. Therefore, symptoms of the same autoimmune disease may affect mother and child, even though the autoantibody is being produced only by the mother’s immune system 13. Candidiasis exacerbation ( ch 10,313) ➢ Candidiasis is a yeastlike fungal infection caused by C. albicans occurring on skin, on mucous membranes, and in the gastrointestinal tract. ➢ Candida overgrowth may occur resulting in vaginitis or oropharyngeal infection (thrush). In those with an intact immune system the infection remains localized. ➢ In immunocompromised individuals, particularly those with diminished levels of neutrophils (neutropenia), disseminated infection may occur. Candida is the most common fungal infection in people with cancer (particularly acute leukemia and other hematologic cancers), transplantation (bone marrow and solid organ), and HIV/AIDS. 14. Carbuncles (ch 46, pg 1635 ➢ a condition in which a bacterial infection of the hair follicle or sebaceous gland ducts becomes painful and discharges pus through various openings. ➢ Furuncles and carbuncles are treated with warm compresses to provide comfort and promote localization and spontaneous drainage. Abscess formation requires incision and drainage and recurrent infections, extensive lesions, or those associated with cellulitis or systemic symptoms are treated with systemic antibiotics. ➢ A carbuncle is a collection of infected hair follicles occurring most often on the back of the neck, the upper back, and the lateral thighs. The lesion begins in the subcutaneous tissue and lower dermis as a firm mass that evolves into an erythematous, painful, swollen mass that drains through many openings. Abscesses may develop. Chills, fever, and malaise are systemic symptoms that can occur during the early stages of lesion development. ➢ Furuncles and carbuncles are treated with warm compresses to provide comfort and promote localization and spontaneous drainage. Abscess formation requires incision and drainage and recurrent infections, extensive lesions, or those associated with cellulitis or systemic symptoms are treated with systemic antibiotics. 15. Terms such as hypochromic, macrocytic, microcytic, etc ( ch 28 pg 983 ) see chart above also it will not move for me ERYTHROCYTE VOLUME HEMOGLOBIN CONTENT Normal Normocytic Normochromic Increased Macrocytic (higher mean corpuscular volume [MCV]) Hyperchromic (higher mean corpuscular hemoglobin concentration [MCHC]) Decreased Microcytic (lower MCV) Hypochromic (lower MCHC) MORPHOLOGY OF REMAINING ERYTHROCYTES NAME AND MECHANISM OF ANEMIA PRIMARY CAUSE Macrocytic-normochromic anemia: large, Pernicious anemia: lack of vitamin B12(cobalamin) for Congenital or acquired deficiency of abnormally shaped erythrocytes but erythropoiesis; abnormal deoxyribonucleic acid (DNA) intrinsic factor (IF); genetic disorder of normal hemoglobin concentrations and ribonucleic acid (RNA) synthesis in the DNA synthesis erythroblast; premature cell death Folate deficiency anemia: lack of folate for Dietary folate deficiency erythropoiesis; premature cell death Microcytic-hypochromic anemia: small, Iron deficiency anemia: lack of iron for hemoglobin Chronic blood loss; dietary iron abnormally shaped erythrocytes and production; insufficient hemoglobin deficiency; disruption of iron metabolism reduced hemoglobin concentration or iron cycle Sideroblastic anemia: dysfunctional iron uptake by Congenital dysfunction of iron erythroblasts and defective porphyrin and heme metabolism in erythroblasts; acquired synthesis dysfunction of iron metabolism as a result of drugs or toxins Thalassemia: impaired synthesis of α- or β-chain of Congenital genetic defect of globin hemoglobin A; phagocytosis of abnormal erythroblasts synthesis in the marrow Normocytic-normochromic anemia: Aplastic anemia: insufficient erythropoiesis Depressed stem cell proliferation normal size, normal hemoglobin resulting in bone marrow aplasia concentration Posthemorrhagic anemia: blood loss Acute or chronic hemorrhage that stimulates increased erythropoiesis, which eventually depletes body iron Hemolytic anemia: premature destruction (lysis) of Increased fragility of erythrocytes mature erythrocytes in the circulation Sickle cell anemia: abnormal hemoglobin synthesis, Congenital dysfunction of hemoglobin abnormal cell shape with susceptibility to damage, synthesis lysis, and phagocytosis Anemia of chronic disease: abnormally increased Chronic infection or inflammation; demand for new erythrocytes malignancy 16. Antibodies, IgG, IgA, etc- (ch 8, pg 229) ➢ There are five molecular classes of immunoglobulins (IgG, IgA, IgM, IgE, and IgD) that are characterized by antigenic, structural, and functional differences. Within two of the immunoglobulin classes are several distinct subclasses including four subclasses of IgG and two subclasses of IgA. ➢ IgG is the most abundant class of immunoglobulins; they constitute 80% to 85% of those circulating in the body and account for most of the protective activity against infections. As a result of selective transport across the placenta, maternal IgG is also the major class of antibody found in blood of the fetus and newborn. Four subclasses of IgG have been described: IgG1, IgG2, IgG3, and IgG4. ➢ IgA can be divided into two subclasses, IgA1 and IgA2. IgA1 molecules are found predominantly in the blood, whereas IgA2 is the predominant class of antibody found in normal body secretions. The IgA molecules found in bodily secretions are dimers anchored together through a J chain and “secretory piece.” This secretory piece is attached to the IgAs inside mucosal epithelial cells and may function to protect these immunoglobulins against degradation by enzymes also found in the secretions. ➢ IgM is the largest of the immunoglobulins and usually exists as a pentamer that is stabilized by a J(joining) chain. It is the first antibody produced during the initial, or primary, response to antigen. IgM is synthesized early in neonatal life, and its synthesis may be increased as a response to infection in utero. 17. Skin cancer ( ch 46 pg, 1641) ➢ Basal cell carcinoma and squamous cell carcinoma are the most prevalent forms of cancer. Malignant melanoma is the most serious and the most common cause of death from skin cancer ➢ Chronic ultraviolet (UV) radiation causes most skin cancers. Protection from UV radiation from the sun and artificial sources (e.g., tanning beds), particularly during the childhood years, significantly reduces the risk of skin cancer in later years. Areas commonly exposed to the sun’s rays—face, neck, and hands—are highly vulnerable for such lesions. Dark-skinned persons and those avoiding sunlight are significantly less likely to develop these malignant tumors. In dark-skinned persons, basal cells contain the pigment melanin, a protective factor against sun exposure ➢ Basal cell carcinoma ( most common) is a surface epithelial tumor of the skin originating from undifferentiated basal or germinative cells. The tumors grow upward and laterally or downward to the dermal-epidermal junction. They usually have depressed centers and rolled borders. Early tumors are so small that they are not clinically apparent. ➢ Squamous cell carcinoma (SCC) is a tumor of the epidermis and the second most common human cancer. characterized: in situ (Bowen disease [BD]) and invasive. Areas affected are the head and neck (75%) and the hands (15%), with 10% of squamous cell carcinomas occurring elsewhere on the body. 18. Parts of the heart in terms of function, such as pericardium ( ch 31, p 1085) ➢ The heart wall has three layers—the epicardium, myocardium, and endocardium—and is enclosed in a double-walled membranous sac, the pericardium ➢ The pericardial sac has several functions. It (1) prevents displacement of the heart during gravitational acceleration or deceleration, (2) acts as a physical barrier that protects the heart against infection and inflammation from the lungs and pleural space, and (3) contains pain receptors and mechanoreceptors that can elicit reflex changes in blood pressure and heart rate. ➢ the outer layer of the pericardium, the parietal pericardium, is composed of a surface layer of mesothelium over a thin layer of connective tissue. The visceral pericardium, or epicardium, is the inner layer of the pericardium ➢ At one point the visceral pericardium folds back and becomes continuous with the parietal pericardium, allowing the large vessels to enter and leave the heart without breaching the pericardial layer ➢ The outer layer of the heart, the epicardium, provides a smooth surface that allows the heart to contract and relax within the pericardium with a minimal amount of friction. ➢ the internal lining of the myocardium is composed of connective tissue and a layer of squamous cells called the endocardium ➢ The endocardial lining of the heart is continuous with the endothelium that lines all the arteries, veins, and capillaries of the body, creating a continuous, closed circulatory system 19. Congenital heart defects (ch 33pg 1200) ➢ Congenital heart disease is the leading cause of death, excluding prematurity, during the first year of life.5It is estimated that as many as 35% of deaths caused by congenital heart defects occur in the first year of life and that one third of children born with congenital heart disease will die as a result of their cardiac disease ➢ The etiology of most congenital heart disease is unknown. ➢ As many as 50% of infants with trisomy 21 have a congenital heart defect, either an AV canal defect or a VSD. Extra cardiac defects are noted in as many as 35% of infants with cardiac lesions. Prospective studies using chromosomal analysis have suggested that congenital cardiac malformations may be the result of a single gene defect 20. Urinary tract obstruction (ch 37, pg 1340) ➢ Urinary tract obstruction is an interference with the flow of urine at any site along the urinary tract. An obstruction may be anatomic or functional. It impedes flow proximal to the obstruction, dilates structures distal to the obstruction, increases risk for infection, and compromises renal function. Anatomic changes in the urinary system caused by obstruction are referred to as obstructive uropathy. The severity of an obstructive uropathy is determined by: (1) the location of the obstructive lesion, (2) the involvement of one or both upper urinary tracts (ureters and renal pelvis), (3) the completeness of the obstruction, (4) the duration of the obstruction, and (5) the nature of the obstructive lesion. Obstructions may be relieved or partially alleviated by correction of the obstruction, although permanent impairments occur if a complete or partial obstruction persists over weeks to months or longer. 21. GI symptoms of conditions such as pyloric stenosis, hiatal hernia, ulcerative colitis- (ch 41 pg 148,1429,1440) ➢ Hiatal hernia is the protrusion of the upper part of the stomach through the hiatus (esophageal opening in the diaphragm) at the gastroesophageal junction. Hiatal hernia can be sliding, paraesophageal, or mixed. ➢ Ulcerative colitis is an inflammatory bowel disease that causes ulceration, abscess formation, and necrosis of the colonic and rectal mucosa. Cramping pain, bleeding, frequent diarrhea, dehydration, and weight loss accompany severe forms of the disease. A course of frequent remissions and exacerbations is common ➢ Pyloric stenosis is an obstruction of the pyloric sphincter caused by hypertrophy of the sphincter muscle. It is one of the most common disorders of early infancy and affects infants between the ages of either 1 and 2 weeks or 3 and 4 months 22. Skin cancer lesions ( ch 46, pg 1641) ➢ Basal cell carcinoma and squamous cell carcinoma are the most prevalent forms of cancer. Malignant melanoma is the most serious and the most common cause of death from skin cancer ➢ Basal cell carcinoma is a surface epithelial tumor of the skin originating from undifferentiated basal or germinative cells. The tumors grow upward and laterally or downward to the dermal-epidermal junction. They usually have depressed centers and rolled borders. Early tumors are so small that they are not clinically apparent. ➢ Basal cell carcinoma is the most common type of skin cancer in whites and is thought to be caused by UV radiation exposure ➢ Squamous cell carcinoma (SCC) is a tumor of the epidermis and the second most common human cancer. ➢ Two types are characterized: in situ (Bowen disease [BD]) and invasive. Areas affected are the head and neck (75%) and the hands (15%), with 10% of squamous cell carcinomas occurring elsewhere on the body. These tumors are more predominant in countries where arsenic is found in higher rates in drinking water. ➢ Cutaneous melanoma is a malignant tumor of the skin originating from melanocytes, or cells that synthesize the pigment melanin. The incidence of melanoma is increasing, and young to middle-age adults are at highest risk. CHARACTERISTIC DESCRIPTION Lentigo Malignant Melanoma Frequency 4% to 15% of cutaneous melanomas Age at diagnosis 50 to 80 years old, mean age 65 years Primary location Head, neck, dorsum of hands (sun-exposed areas) Pigmentation according to thickness <1.5 mm (levels I and II) Tan and brown >1.5 mm (level III) Tan, brown, and blue-black >1.5 mm (levels IV and V) Nodule formation Superficial Spreading Melanomas Frequency 57% to 70% of cutaneous melanomas Age at diagnosis 20 to 60 years old Primary location Legs of females; upper back of both genders Pigmentation according to thickness <1.5 mm (levels I and II) Tan and brown >1.5 mm (level III) Tan, brown, and blue-black >1.5 mm (levels IV and V) Nodule formation Primary Nodular Melanoma Frequency 12% to 21% of cutaneous melanomas Age at diagnosis 20 to 60 years old, mean age 53 years Primary location Trunk, head, or neck Pigmentation according to thickness >1.5 mm (level III) Small nodule (any hue) >1.5 mm (levels IV and V) Large nodule (any hue) Acral-Lentiginous Melanoma Frequency 2% to 8% in whites; 30% to 75% in blacks, Hispanics, Asians Age at diagnosis 20 to 60 years old Primary location Palms, soles of feet, mucous membranes Pigmentation at any thickness Blue-black irregular macules, papules, or nodules 23. Gastroesophageal reflux disease- (c 41, p 1439) ➢ Gastroesophageal reflux disease is the regurgitation of chyme from the stomach into the esophagus, causing esophagitis from repeated exposure to acids and enzymes in the regurgitated gastric contents. 24. Hypersensitivity reaction ( ch 9 ,p262)- ➢ Hypersensitivity is an altered immunologic response to an antigen that results in disease or damage to the host. Hypersensitivity reactions can be classified in two ways: by the source of the antigen that the immune system is attacking MECHANISM TYPE I (IMMUNOGLOBULIN E–[IgE] MEDIATED) TYPE II (TISSUE SPECIFIC) TYPE III (IMMUNE COMPLEX) TYPE IV (CELL MEDIATED) Allergy ++++ + + ++ Environmental antigens Hay fever Hemolysis in drug allergies Gluten (wheat) allergy Poison ivy allergy Autoimmunity ± ++ +++ + Self-antigens May contribute to some type III reactions Autoimmune thrombocytopenia Systemic lupus erythematosus Hashimoto thyroiditis Alloimmunity ± ++ + ++ Another person’s antigens May contribute to some type III reactions Hemolytic disease of the newborn Anaphylaxis to IgA in IV gamma globulin Graft rejection 25. Congenital intrinsic factor deficiency( ch 28, 988) ➢ Deficiency in IF secretion may be congenital or, more often, an autoimmune process directed against gastric parietal cells. Congenital IF deficiency is a genetic disorder that demonstrates an autosomal recessive inheritance pattern. The autoimmune form of the disease also has a genetic component, as do most autoimmune diseases ➢ The principal disorder in PA is an absence of intrinsic factor (IF), a transporter required for absorption of dietary vitamin B12, which is essential for nuclear maturation and DNA synthesis in erythrocytes. IF is secreted by gastric parietal cells and complexes with dietary vitamin B12 in the small intestine. The B12-IF complex binds to cell surface receptors in the ileum and is transported across the intestinal mucosa. 26. Acid base imbalance – (ch 3 p 1236) ➢ Pathophysiologic changes in the concentration of hydrogen ion or base in the blood lead to acid-base imbalances. ➢ An abnormal increase or decrease in bicarbonate concentration causes metabolic acidosis or metabolic alkalosis; changes in the rate of alveolar ventilation produce respiratory acidosis or respiratory alkalosis. ➢ Metabolic acidosis is caused by an increase in the concentrations of non-carbonic acids or by loss of bicarbonate from the extracellular fluid. ➢ Metabolic alkalosis occurs with an increase in bicarbonate concentration usually caused by loss of metabolic acids from conditions such as vomiting, gastrointestinal suctioning, excessive bicarbonate intake, hyperaldosteronism, and diuretic therapy. ➢ Respiratory acidosis occurs with a decrease of alveolar ventilation and an increase in levels of carbon dioxide, or hypercapnia. ➢ Respiratory alkalosis occurs with alveolar hyperventilation and excessive reduction of carbon dioxide concentration, or hypocapnia. 27. Acute epiglottitis(ch 36,pg 1296) ➢ Historically, acute epiglottitis was caused by Haemophilus influenzae type B (Hib). Since the advent of Hib immunization, the overall incidence of acute epiglottitis in children has decreased significantly, although Hib still accounts for approximately 25% of the cases seen in children. Infants less than 1 year of age are at greater risk.Current pediatric cases usually represent Hib vaccine failures or are caused by alternative pathogens, such as groups A, B, C, F, and G streptococci, Streptococcus pneumoniae, Candidaspecies, Staphylococcus aureus, and viral pathogens. Thermal injuries, trauma, and posttransplant lymphoproliferative disorder also have been reported as causes of epiglottitis. ➢ Acute epiglottitis is a life-threatening emergency. The essentials are early recognition, avoidance of disturbing the child (which could worsen the obstruction), and securing the airway. 28. Types of gastric ulcers-signs and symptoms, characteristics ( ch 41, pg 1437-1438) ➢ The clinical manifestations of gastric ulcers are similar to those of duodenal ulcers . The pattern of pain, food, and relief is common, but the pain of gastric ulcers also occurs immediately after eating. ➢ Gastric ulcers also tend to be chronic rather than alternate between periods of remission and exacerbation and cause more anorexia, vomiting, and weight loss than duodenal ulcers. ➢ On set age 50 to 70 years of age, family history- usually negative, gender – equal in men and women, stress factors- increased , ulcerogenic drugs- normal use, cancer risk – increased, Pahtophysiology- Helicobacter pylori incfection – often present (6o% to 80%) abnormal mucus- may be present, parietal call mass – normal or decreased, acid production- normal or decreased, serum gastrin – increased, serum pepsiogen – normal , associated gastritis – more common , clinical manifestations - pain – located in upper abdomen, inttermittent, pain antacid-relief pattern, food pain pattern, clinical course- chronic ulcer without pattern of remissionn and exacerbation 29. Lupus (ch 9,p277) ➢ Systemic lupus erythematosus (SLE) is a chronic, multisystem, inflammatory disease and is one of the most common, complex, and serious of the autoimmune disorders. SLE is characterized by the production of a large variety of autoantibodies against nucleic acids, erythrocytes, coagulation proteins, phospholipids, lymphocytes, platelets, and many other self-components. The most characteristic autoantibodies produced in SLE are against nucleic acids (e.g., single-stranded deoxyribonucleic acid [DNA], double-stranded DNA), histones, ribonucleoproteins, and other nuclear materials. 30. General adaptation syndrome (ch 11,p 339) ➢ Selye concluded that this triad or syndrome of manifestations represented a nonspecific response to noxious stimuli, naming it the general adaptation syndrome (GAS). He identified three successive stages of the GAS: (1) the alarm stage or reaction, in which the central nervous system (CNS) is aroused and the body’s defenses are mobilized (e.g., “fight or flight”); (2) the stage of resistance or adaptation, during which mobilization contributes to “fight or flight”; and (3) the stage of exhaustion, where continuous stress causes the progressive breakdown of compensatory mechanisms (acquired adaptations) and homeostasis. Exhaustion marks the onset of certain diseases (diseases of adaptation). 31. Ventilation/perfusion ratio ( ch 34, pg 1238-1239) ➢ The relationship between ventilation and perfusion is expressed as a ratio called the ventilation-perfusion ratio, or ˙V/˙Q.The normal ˙V/˙Q ratio is 0.8. This is the amount by which perfusion exceeds ventilation under normal conditions. 32. Bile salt deficiencies ( ch 41,pg 1440) ➢ Conjugated bile acids (bile salts) are necessary for the digestion and absorption of fats. Bile salts are conjugated in the bile that is synthesized from cholesterol and secreted from the liver. When bile enters the duodenum, the bile salts aggregate with fatty acids and monoglycerides to form micelles. Micelle formation makes fat molecules more soluble and allows them to pass through the unstirred layer at the brush border of the small intestinal villi ➢ Clinical manifestations of bile salt deficiency are related to poor intestinal absorption of fat and fat-soluble vitamins (A, D, E, and K). Increased fat in the stools (steatorrhea) leads to diarrhea and decreased plasma proteins. The losses of fat-soluble vitamins and their effects include the following: 1. Vitamin A deficiency results in night blindness. 2. Vitamin D deficiency results in decreased calcium absorption with bone demineralization (osteoporosis), bone pain, and fractures. 3. Vitamin K deficiency prolongs prothrombin time, leading to spontaneous development of purpura (bruising) and petechiae. 4. Vitamin E deficiency has uncertain effects but may cause testicular atrophy and neurologic defects in children. The most effective treatment for fat-soluble vitamin deficiency is to increase the amount of medium-chain triglycerides in the diet, for example, by using coconut oil for cooking. Vitamins A, D, and K are given parenterally. 33. Clonal selection (ch 12, pg373) ➢ This is referred to as clonal proliferation or clonal expansion . As a clone with a mutation proliferates, it may become an early stage tumor, for example, a carcinoma in situ or a benign colonic polyp. Additional heritable changes can occur in these early lesions that permit progression to more advanced tumors. The process of tumor development is a form of darwinian evolution; cells with a genetic change that confers a survival advantage out-compete their neighbors. The progressive accumulation of distinct advantageous (from the point of view of the cancer cell, not the individual!) mutations leads from normal cells to fully malignant cancers. 34. Obstructive sleep apnea (ch 16,pg 504) ➢ Obstructive sleep apnea syndrome (OSAS) is a disorder of breathing during sleep related to upper airway obstruction that is associated with reduced blood oxygen saturation and hypercapnia. The typical classification of the severity of this disease uses the Apnea Hypopnea Index (AHI). This index represents how many apnea (total airway closure) or hypopnea (partial airway closure) episodes occur per night—the number of which is then divided by the night’s total sleep time to give an average number of apnea or hypopnea episodes per hour. 35. Large bowel obstruction (ch 41,pg 1431) ➢ Chronic or partial obstructions are more often associated with tumors or inflammatory disorders, particularly of the large intestine. Intussusception is rare in adults compared with the more frequent occurrence in infants. The most common causes of large bowel obstruction are colorectal cancer, volvulus (twisting), and strictures related to diverticulitis. 36. Vaginal candidiasis (ch 24,pg 874) ➢ Vaginitis, or vaginal infection, is usually caused by sexually transmitted pathogens or C. albicans, which causes candidiasis. Development is related to the overall health of a woman and local defense mechanisms, particularly vaginal pH. Variables such as antibiotics, douching, soaps, feminine hygiene sprays, and pregnancy alter vaginal pH or the bactericidal nature of secretions and predispose a woman to infection. 37. Folate deficiency (ch 2,pg 67) ➢ Folic acid deficiency is a common problem in chronic alcoholic populations. Ethanol alters folic acid (folate) homeostasis by decreasing intestinal absorption of folate, increases liver retention of folate, and increases the loss of folate through urinary and fecal excretion.Folic acid deficiency becomes especially serious in pregnant women who consume alcohol and may contribute to fetal alcohol syndrome ➢ A deficiency of folate also is implicated in the development of cancers, specifically colorectal cancers. ➢ Folate deficiency is more common than vitamin B12 deficiency and occurs more rapidly. 38. Pancreatic insufficiency (ch 41 pg 1439) ➢ Pancreatic insufficiency is the deficient production of these enzymes by the pancreas. Causes of pancreatic insufficiency include chronic pancreatitis, pancreatic carcinoma, pancreatic resection, and cystic fibrosis. Significant damage to or loss of pancreatic tissue must occur before enzyme levels decrease sufficiently to cause maldigestion. Although pancreatic insufficiencycauses poor digestion of all nutrients, fat maldigestion is the chief problem. 39. Types of fractures- ( ch 44,pg 1541-1542) 40. Genetic disorders such as Down Syndrome, Turner Syndrome, etc ( ch 4 pg 146-150) ➢ The most well-known example of aneuploidy in an autosome is trisomy of the twenty-first chromosome, which causes Down syndrome (named after J. Langdon Down, who first described the disease in 1866). Down syndrome was formerly called mongolism, but this inappropriate term is no longer used. Down syndrome is seen in 1 in 800 live births ➢ The facial appearance is distinctive, with a low nasal bridge, epicanthal folds, protruding tongue, and flat, low-set ears. Poor muscle tone (hypotonia) and short stature are both characteristic. Congenital heart defects affect about one third to one half of live-born children with Down syndrome; a reduced ability to fight respiratory tract infections and an increased susceptibility to leukemia also contribute to reduced survival rate. By 40 years of age, individuals with Down syndrome virtually always develop symptoms that are nearly identical to those of Alzheimer disease because one of the genes that can cause Alzheimer disease is located on chromosome 21. ➢ The karyotype is designated 45,X, and it causes a set of symptoms known as Turner syndrome they are usually sterile, however, and have gonadal streaks rather than ovaries. These streaks of connective tissue are susceptible to cancer in mosaics who have some cells containing a Y chromosome. ➢ Other features of the disorder include short stature, webbing of the neck in about half of cases, widely spaced nipples, coarctation (narrowing) of the aorta (in 15% to 20% of cases), edema of the feet in newborns, and sparse body hair. Their IQs are typically in the normal range, although they often have some impairment of spatial and mathematical reasoning ability. About three fourths of recognized 45,X conceptions inherit their X chromosome from the mother. Thus most cases are caused by a loss of the paternal X chromosome. ➢ Individuals with at least two X chromosomes and a Y chromosome in each cell (47,XXY karyotype) have a disorder known as Klinefelter syndrome ➢ Because of the presence of a Y chromosome, these individuals have a male appearance, but they are usually sterile, and about half develop female-like breasts (a condition called gynecomastia). The testes are small, body hair is sparse, the voice is often somewhat high pitched, stature is elevated, and a moderate degree of mental impairment may be present. Klinefelter syndrome is found in about 1 in 1000 male births 41. Vitamin B-12 therapy (ch ch 28,pg 988) ➢ Replacement of vitamin B12 (cobalamin) is the treatment of choice. Initial injections of vitamin B12 are administered weekly until the deficiency is corrected, followed by monthly injections for the remainder of the individual’s life. The effectiveness of cobalamin replacement therapy is determined by a rising reticulocyte count. Within 5 to 6 weeks, blood counts return to normal. PA cannot be cured so maintenance therapy is lifelong. Conventional wisdom and practice assumed that oral preparations were ineffective because there was no IF to facilitate absorption of vitamin B12. However, recent experience has shown that higher doses of orally administered vitamin B12 will be absorbed across the small bowel and is beneficial. 42. Glaucoma- ( ch 16, pg 510) ➢ Glaucoma is a leading cause of visual impairment and blindness. It is characterized by intraocular pressures greater than the normal pressures of 12 to 20 mmHg maintained by the aqueous fluid. Family history is a risk factor, and glaucoma can be inherited 43. Cervical immunoglobulin- (ch 23, pg 775) ➢ The external cervical os is a very small opening that contains thick, sticky mucus (the mucous plug) during the luteal phase of the menstrual cycle and all of pregnancy. During ovulation the mucus changes under the influence of estrogen and forms watery strands, or spinnbarkeit mucus, to facilitate the transport of sperm into the uterus ➢ the downward flow of cervical secretions moves microorganisms away from the cervix and uterus. In women of reproductive age, the pH of these secretions is inhospitable to most bacteria. Furthermore, mucosal secretions contain enzymes and antibodies (mostly immunoglobulin A) of the secretory (humoral) immune system ➢ These defenses do not always prevent infection, even if they are intact. Besides infection, uterine pathophysiology includes displacement of the uterus within the pelvis, benign growths (fibroids) of the uterine wall, hyperplasia of the endometrium, endometriosis, and cancer. 44. Concept of pain ( ch 16 p 485) ➢ Pain is one of the body’s most important adaptive and protective mechanisms and all definitions suggest it is a complex phenomenon and cannot be characterized as only a response to injury ➢ Waddell defines pain as “…a symptom, not a clinical sign, diagnosis or disease.…”2 A clear understanding of the complexities of the pain experience—specifically one that encompasses an individual’s emotions, cognition, motivation, prior history, and even issues of secondary gain—is needed to manage pain and to further understand the pain processes. “The inability to communicate verbally does not negate the possibility that an individual is experiencing pain and is in need of appropriate pain-relieving treatment. Pain is always subjective. 45. Autosomal dominant diseases ( ch 4 pg 153) ➢ Parents at risk for producing children with a genetic disease nearly always ask the question, “What is the chance that our child will have this disease?” The probability that a family member will have a genetic disease is termed the recurrence risk. When one parent is affected by an autosomal dominant disease (and is a heterozygote) and the other is normal, the recurrence risks for each child are one half. ➢ Huntington disease is another well-known autosomal dominant condition and its main features are progressive dementia and increasingly uncontrollable movements of the limbs ➢ One of the key features of this disease is that symptoms are not usually seen until age 40 years or later, a pattern known as age-dependent penetrance. 46. Congenital murmurs ( ch 32 pg 1168-1170) ➢ Aortic stenosis – congenital bicuspid valve, degenerative (calcification) changes with aging, rheumatic fever, left ventricular hypertrophy followed by left heart failure; decreased blood flow with myocardial ischemia, pulmonary edema: dyspnea on exertion, syncope especially on exertion, pain- angina pectoris, systolic murmur heard best at the right parasternal second intercostal space and radiating to the neck. ➢ Tricuspid regurgitation – congenital, right heart failure, dyspnea, palpitations, murmur throughout systole heard best at the left lower sternal border. 47. Lactose intolerance (CH 42,PG 1500)- ➢ Lactose intolerance is the inability to digest lactose (milk sugar). It is caused by inadequate production of lactase and is a common cause of diarrhea in children, particularly nonwhite children younger than 7 years of age. The malabsorption of lactose results in osmotic diarrhea, in which fluids move by osmosis from the vascular compartment into the intestinal lumen. The undigested sugar is processed by the colonic bacteria, and intestinal gas is produced. ➢ The diarrhea is accompanied by abdominal pain, bloating, and flatulence. Diagnosis includes elimination of dietary lactose or hydrogen breath testing. Treatment consists of using lactase-treated dairy products or lactase supplements or reducing dairy product consumption. Other sources of dietary calcium or supplements need to be provided if dairy products are eliminated. Some children can tolerate lactose in fermented forms, such as cheese and yogurt ➢ a condition caused by lactase deficiency in which lactose is not metabolized, making it impossible for the small intestine to absorb it and causing excessive gas production and diarrhea when exposed to lactose-containing foods. 48. Angiotensin-renin system ( ch 5, ch 37 pg 1327) ➢ Aldosterone synthesis and secretion are regulated primarily by the renin-angiotensin-aldosterone system ➢ A major hormonal regulator of renal blood flow is the renin-angiotensin-aldosterone system (RAAS), which can increase systemic arterial pressure and increase sodium reabsorption. Renin is an enzyme formed and stored in granular cells of the afferent arterioles of the JGA ➢ The release of renin is principally triggered by decreased blood pressure in the afferent arterioles, which reduces stretch of the juxtaglomerular cells; decreased sodium chloride concentrations in the distal convoluted tubule; sympathetic nerve stimulation of β-adrenergic receptors on the juxtaglomerular cells; and release of prostaglandins 49. AIDS (ch 10pg 322) ➢ AIDS is a viral disease caused by the human immunodeficiency virus (HIV). HIV infects and depletes a portion of the immune system (Th cells), making individuals extremely susceptible to life-threatening infections and malignancies ➢ HIV is a blood-borne pathogen present in body fluids (e.g., blood, vaginal fluid, semen, breast milk) with the typical routes of transmission: blood or blood products, intravenous drug abuse, heterosexual and homosexual activity, and maternal-child transmission before or during birth. 50. Carcinoma ( ch 12 pg 363 ) BENIGN TUMORS MALIGNANT TUMORS Grow slowly Grow rapidly Have a well-defined capsule Are not encapsulated Are not invasive Invade local structures and tissues Are well differentiated; look like the tissue from which they arose Are poorly differentiated; may not be able to determine tissue of origin Have a low mitotic index; dividing cells are rare High mitotic index; many dividing cells Do not metastasize Can spread distantly, often through blood vessels and lymphatics 51. Hormonal regulation of calcium ( ch 3 pg 119) ➢ Calcium (Ca++) is a necessary ion for many fundamental metabolic processes. It is the major cation associated with the structure of bones and teeth. It serves as an enzymatic cofactor for blood clotting and is required for hormone secretion and the function of cell receptors. Plasma membrane stability and permeability are directly related to calcium ions, as is the transmission of nerve impulses and the contraction of muscles. Intracellular calcium is located primarily in the mitochondria. ➢ Calcium and phosphate balance is regulated by three hormones: parathyroid hormone (PTH), vitamin D, and calcitonin ➢ The parathyroid glands secrete PTH in response to low levels of serum calcium ➢ As calcium levels increase, an opposite adaptation occurs, leading to suppression of PTH secretion, decreased renal vitamin D activation, decreased intestinal calcium absorption, and increased renal phosphate reabsorption. 52. Neural tube defect- (ch 20,pg 663)and )ch 5,pg 167) ➢ lack of closure of the neural groove caused by an arrest of the normal development of the brain and spinal cord during the first month of embryonic development. ➢ Neural tube defects (NTDs), which include anencephaly, spina bifida, and encephalocele (as well as several other less common forms), are one of the most important classes of birth defects, and they are seen in 0.5 to 2 of 1000 pregnancies ➢ Normally the neural reopening of the neural closes at about the fourth week of gestation. A defect in closure, or a subsequent , results in a neural tube defect 53. Types of hormones- ( google) Endocrine gland Hormone Main tissues acted on by hormone Main function of hormones Hypothalamus Thyrotrophin releasing hormone (TRH) Anterior pituitary Stimulates release of thyroid stimulating hormone (TSH) from the anterior pituitary Somatostatin Anterior pituitary Inhibitory hormone that prevents release of hormones such as growth hormone from the anterior pituitary Gonadotrophin releasing hormone (GnRH) Anterior pituitary Stimulates release of follicle stimulating hormone (FSH) and luteinising hormone (LH) from the anterior pituitary Corticotrophin releasing Anterior pituitary Stimulates adrenocorticotrophic hormone (ACTH) release from hormone (CRH) the anterior pituitary Growth Hormone Releasing Hormone (GHRH) Anterior pituitary Stimulates release of growth hormone (GH) form the anterior pituitary Anterior pituitary Thyroid stimulating hormone (TSH) Thyroid gland Stimulates release of thyroxine and tri-iodothyronine from the thyroid gland Luteinising hormone (LH) Ovary/Testis Females: promotes ovulation of the egg and stimulates oestrogen and progesterone production Males: promotes testosterone release from the testis Follicle stimulating hormone (FSH) Ovary/Testis Females: promotes development of eggs and follicles in the ovary prior to ovulation Males: promotes production of testosterone from testis Growth Hormone (GH) Bones, cartilage, muscle, fat, liver, heart Acts to promote growth of bones and organs Prolactin (PRL) Breasts, brain Stimulates milk production in the breasts and plays a role in sexual behavior Adrenocortico-trophic hormone (ACTH) Adrenal glands Stimulates the adrenal glands to produce mainly cortisol Posterior pituitary Vasopressin (anti-diuretic hormone, ADH) Kidney, blood vessels, blood components Acts to maintain blood pressure by causing the kidney to retain fluid and by constricting blood vessels Oxytocin Uterus, milk ducts of breasts Causes ejection of milk from the milk ducts and causes constriction of the uterus during labour Thyroid gland Thyroxine (T4) Most tissues Acts to regulate the body’s metabolic rate Tri-iodothyronine (T3) Most tissues Acts to regulate the body’s metabolic rate Parathyroid glands Parathyroid hormone (PTH) Kidney, Bone cells Increases blood calcium levels in the blood when they are low Calcitonin Kidney, Bone cells Decreases blood calcium levels when they are high Adrenal cortex Cortisol Most tissues Involved in a huge array of physiological functions including blood pressure regulation, immune system functioning and blood glucose regulation Aldosterone Kidney Acts to maintain blood pressure by causing salt and water retention Androgens Most tissues Steroid hormones that promote development of male characteristics. Physiological function unclear Adrenal medulla Adrenaline and noradrenaline (the catecholamines) Most tissues Involved in many physiological systems including blood pressure regulation, gastrointestinal movement and patency of the airways Pancreas Insulin Muscle, fat tissue Acts to lower blood glucose levels Glucagon Liver Acts to raise blood glucose levels Somatostatin Pancreas Acts to inhibit glucagon and insulin release Ovary Oestrogens Breast, Uterus, Internal and external genitalia Acts to promote development of female primary and secondary sexual characteristics. Important role in preparing the uterus for implantation of embryo Progesterone BreastUterus Affects female sexual characteristics and important in the maintenance of pregnancy Testis Testosterone Sexual organs Promotes the development of male sexual characteristics including sperm development Stomach Gastrin Stomach Promotes acid secretion in the stomach Serotonin (5-HT) Stomach Causes constriction of the stomach muscles Duodenum and jejunum Secretin Stomach, Liver Inhibits secretions from the stomach and increases bile production Cholecystokinin (CCK) Liver, Pancreas Stimulates release of bile from the gall bladder and causes the pancreas to release digestive enzymes Kidney Erythropoietin Bone marrow Stimulates red blood cell development in the bone marrow Heart Atrial natiuretic factor (ANF) Kidney Lowers blood pressure by promoting salt and water loss Skin Vitamin D Small intestine, Kidney, Bone cells Stimulates the uptake of calcium in the small intestine, retention of calcium and release of calcium from bone stores 54. Glycoprotein (ch 8 ,pg 229) ➢ An antibody, or immunoglobulin, is a serum glycoprotein produced by plasma cells in response to a challenge by an immunogen. The term immunoglobulin is used to denote all molecules that are known to have specificity for antigen, whereas the term antibody is generally used to denote one particular set of immunoglobulins with specificity against a known antigen 55. Kidney stones (Ch 38, pg 1343) ➢ Calculi, or urinary stones (urolithiasis), are masses of crystals, protein, or other substances that are a common cause of urinary tract obstruction in adults. They can be located in the kidneys, ureters, and urinary bladder. The prevalence of stones in the United States is approximately 6% in women and 15% in men, and is more common in whites ➢ Most kidney stones are unilateral and are a risk factor for chronic kidney disease and an increased risk for myocardial infarction. ➢ Renal calculus formation is complex and related to: (1) supersaturation of one or more salts in the urine, (2) precipitation of the salts from a liquid to a solid state (crystals), (3) growth through crystallization or agglomeration (sometimes called aggregation), and (4) the presence or absence of stone inhibitors 56. Type 2 diabetes ( ch 22, pg 739) ➢ a condition of glucose intolerance that normally appears first in adulthood and is exacerbated by obesity and an inactive lifestyle. ➢ genes have been identified that are associated with type 2 diabetes, including those that code for beta-cell mass, beta-cell function (ability to sense blood glucose levels, insulin synthesis, and insulin secretion), proinsulin and insulin molecular structure, insulin receptors, hepatic synthesis of glucose, glucagon synthesis, and cellular responsiveness to insulin stimulation. ➢ Although many individuals with risk factors for type 2 diabetes (including obesity, metabolic syndrome, and hypertension) are insulin resistant, only those individuals who are genetically predisposed to beta-cell dysfunction (and therefore a relative deficiency in insulin) will develop type 2 diabetes 57. Pituitary hormone secretion- (ch 21 pg 696-698) ➢ Thyroid-stimulating hormone (TSH) secretion from the anterior pituitary is stimulated by thyrotropin- releasing hormone (TRH) from the hypothalamus. Secretion of TSH stimulates the synthesis and secretion of thyroid hormones. Increasing levels of T4(thyroxine) and T3 (triiodothyronine) then generate negative feedback on the pituitary and hypothalamus to inhibit TRH and TSH synthesis. HORMONE TARGET TISSUE ACTION Substance P Dopamine Prolactin-releasing factor (PRF) Anterior pituitary Inhibits synthesis and release of ACTH Stimulates secretion of GH, FSH, LH, and prolactin Anterior pituitary Inhibits synthesis and secretion of prolactin 58. Signs of breast cancer ( ch 24, pg 873) CLINICAL MANIFESTATION PATHOPHYSIOLOGY Chest pain Metastasis to the lung Dilated blood vessels Obstruction of venous return by a fast-growing tumor; obstruction dilates superficial veins Dimpling of the skin Can occur with invasion of the dermal lymphatics because of retraction of Cooper ligament or involvement of the pectoralis fascia Edema Local inflammation or lymphatic obstruction Edema of the arm Obstruction of lymphatic drainage in the axilla Hemorrhage Erosion of blood vessels Local pain Local obstruction caused by the tumor Nipple/areolar eczema Paget disease Nipple discharge in a nonlactating woman Spontaneous and intermittent discharge caused by tumor obstruction Nipple retraction Shortening of the mammary ducts Pitting of the skin (similar to the surface of an Obstruction of the subcutaneous lymphatics, resulting in the accumulation of fluid orange [peau d’orange]) Reddened skin, local tenderness, and warmth Inflammation Skin retraction Involvement of the suspensory ligaments Ulceration Tumor necrosis 59. Alzheimer’s disease- ( ch5, p 178) ➢ a degenerative disease characterized by amyloid plaques and fibrillary tangles in the cortex and atrophy and widened sulci in the frontal and temporal lobes. ➢ The plaques and tangles lead to progressive neuronal loss, and death usually occurs within 7 to 10 years after the first appearance of symptoms. 60. Guillain-Barre Syndrome (ch 17, p 622) ➢ Guillain-Barré syndrome is an acquired, acute inflammatory demyelinating or axonal disorder caused by a humoral or cell-mediated immunologic response, or both, directed at peripheral nerves. Four subtypes have been identified and clinical manifestations depend on the subtype. SUBTYPES CLINICAL FEATURES PATHOLOGY PATHOGENESIS Acute inflammatory Ascending paralysis Macrophages invade T-cell–mediated demyelinating with typically distant myelin sheaths and lymphocytic infiltration polyneuropathy start denude axons into nerves is common (AIDP accounts for Lymphocytic most cases of GBS) inflammation Demyelination Endoneurial edema Some degree of axon loss (all findings most prominent in the spinal roots and nerve terminals) Antibody-mediated pathogenesis not yet demonstrated CD4 and CD8 lymphocytes and macrophages are present Complement is deposited on the outermost Schwann cell plasmalemma Macrophages invade nodes of Ranvier, leaving the myelin sheath intact (absence of demyelination) Axonal degeneration in ventral root in severe cases Lymphocyte infiltration sparse Similar to AMAN Absence of demyelination Evidence of axonal loss in dorsal and ventral roots Selective antibody- mediated attack on axon (presence of IgG and complement deposits on axolemma along with macrophage recruitment) Associated with Campylobacter jejunienteritis GM1 autoantibodies play a direct pathogenic role through molecular mimicry Undetermined Lymphocytic infiltration sparse Extensive sensory nerve fiber degeneration Pathologic features similar to those in Antibodies to ganglioside GQ1b measured in serum AIDP, but are atypical in 90% of cases FS Deposition of antiganglioside antibodies initially causes reversible conduction block followed by axonal degeneration Anti-GQ1b antibodies cross-react with other gangliosides (typically GT1a, but in many cases with GD3, GD1b, and GT1b) 61. Sympathetic/parasympathetic nervous system ( ch 11 pg 344) ➢ The parasympathetic system balances the sympathetic nervous system and, thus, also influences adaptation or maladaptation to stressful events. The parasympathetic system also has anti-inflammatory effects. ➢ The parasympathetic system opposes the sympathetic (catecholamine) responses, for example, by slowing the heart rate. Researchers evaluate the relative balance of the parasympathetic and sympathetic nervous systems using a technique known as heart rate variability (the measurement of R wave variability from heartbeat to heartbeat). ➢ Under conditions of allostatic overload, the parasympathetic system may decrease its restraint of the sympathetic system, resulting in increased or prolonged inflammatory responses 62. ACTH- (c 11,pg 339) ➢ Adrenocorticotropic hormone; ➢ the hypothalamus secretes corticotropin-releasing hormone (CRH), which binds to specific receptors on pituitary cells that, in turn, produce adrenocorticotropic hormone (ACTH). ACTH is then transported through the blood to the adrenal glands located on the top of the kidneys 63. Bartholin glands (C24,pg 920) ➢ Bartholin glands]) near the urethra and vagina also are common. The external female genitalia are the mons pubis, labia majora, labia minora, clitoris, vestibule (urinary and vaginal openings), Bartholin glands, and Skene glands. 64. Gonococcal disease (c 26,pg 919) ➢ a sexually transmitted disease caused by the bacteria gonococci that invade the mucous membranes of the genitals and urinary tract and in women the cervix, fallopian tubes, and ovaries, causing chronic pelvic pain or infertility. ➢ Gonorrhea is caused by gonococci (singular, gonococcus), which are microorganisms of the species Neisseria gonorrhoeae. Neisser first identified gonococci in stained smears of vaginal, urethral, and conjunctival exudate in 1879. 65. Glomerulonephritis-( chap 38) ➢ Glomerulonephritis is an inflammation of the glomerulus caused by primary glomerular injury, including immunologic responses, ischemia, free radicals, drugs, toxins, vascular disorders, and infection. 66. Small patent ductus arteriosus ( ch 33, pg 1202) ➢ The patent ductus arteriosus (PDA) is a vessel located between the junction of the main and left pulmonary arteries and the lesser curvature of the descending aorta, usually just distal to the left subclavian artery ➢ PDA closure in asymptomatic children with a murmur is recommended by 2 years of age because of the risk of subacute bacterial endocarditis. No treatment is recommended for small PDA in the absence of a murmur or other cardiac conditions 67. Risk factors for hypertension- ( ch 32, pg 1132-1140) ➢ Risk factors associated with primary hypertension include: (1) family history of hypertension; (2) advancing age; (3) gender (men younger than 55 and women older than 70 years); (4) black race; (5) high dietary sodium intake; (6) glucose intolerance (diabetes mellitus); (7) cigarette smoking; (8) obesity; (9) heavy alcohol consumption; and (10) low dietary intake of potassium, calcium, and magnesium.19 Many of these factors are also risk factors for other cardiovascular disorders. In fact, hypertension, dyslipidemia, and glucose intolerance often are found together in a condition called metabolic syndrome ➢ Evaluation of the hypertensive individual should include a complete medical history and assessment of lifestyle and other risk factors for hypertension and cardiovascular disease, as well as evidence of possible secondary causes of hypertension ➢ Idiopathic, or primary, orthostatic hypotension is the term for hypotension in which there is no known initial cause. It is a significant risk factor for falls and associated injuries and has been associated with an increased risk for cardiovascular events. In addition to cardiovascular symptoms, impotence and bowel and bladder dysfunction often are found in this type. 68. Loss of language and/or comprehension-such as terms-aphasia, etc. ( ch 17, pg 539) ➢ This area is responsible for reception and interpretation of speech, and dysfunction may result in receptive aphasia or dysphasia. ➢ Dysphasia is impairment of comprehension or production of language (semantic processing). With dysphasia, comprehension or use of symbols, in either written or verbal language, is disturbed or lost. ➢ Aphasia is loss of comprehension or production of language. 69. Chronic inflammatory joint disease ( ch 44, pg 1568-1578) ➢ Rheumatoid arthritis (RA) is a chronic, systemic inflammatory autoimmune disease distinguished by jointswelling and tenderness and destruction of synovial joints, leading to disability and premature death ➢ Ankylosing spondylitis (AS) is the most common of a group of inflammatory arthropathies known as spondyloarthropathies. It is a chronic inflammatory joint disease characterized by stiffening and fusion (ankylosis) of the spine and sacroiliac joints 70. Male and female sex hormone production ( ch 23 pg 726-791) ➢ The male sex hormones are androgens and testosterone is the primary male sex hormone. Leydig cells of the testes and, to a lesser degree, the adrenal glands produce testosterone and other androgens. In men, sex hormone production is relatively constant with some diurnal variation ➢ The sex hormones are all steroid hormones and are synthesized from cholesterol Male and female sex hormones are present in all adults. However, the female body contains low levels of testosterone and other androgens, and the male body contains low levels of estrogen. Individual effects of sex hormones depend on their amount and concentration in the blood. ➢ The dominant female sex hormones, estrogen and progesterone, are produced primarily by the ovaries. During fetal development, infancy, and childhood, sex hormone production is low. 71. Endogenous antigen (c 8,pg 245) ➢ Endogenous antigens are usually components of proteins synthesized in the cytosol. They are degraded in the cytosol by proteasomes into small peptides and transported by TAP (transporter associated with antigen processing) proteins (TAP-1 and TAP-2) into the endoplasmic reticulum, where MHC class I and class II molecules are assembled.The class I MHC molecules have open antigen-binding sites so that antigen, the class I MHC α-chain, and a β2-microglobulin molecule form a stable complex that is transported through the Golgi apparatus to the plasma membrane. The antigenic peptides presented by class I MHC molecules are usually very small, 8 to 10 amino acids in length. 72. Genital warts- (ch 26, pg 934) a. Condylomata acuminata are soft, skin-colored, whitish pink to reddish brown discrete growths. They may occur singly or in clusters and may be broad based or pedunculated and feathery or smooth Sometimes the warts enlarge to form cauliflower-like masses on the male frenulum, glans, foreskin, urinary meatus, shaft, scrotum, or anus and on the female labia, clitoris, perineum, vagina, or anus. Although the lesions are usually not painful, they may cause dyspareunia (painful intercourse) and may be friable and bleed easily. b. Genital warts are very contagious, with transmission rates among individuals estimated to be between 38% and 95%. Such a wide range is attributable to the subclinical nature of some infections and various influencing factors that include number of exposures, HPV type, location of lesions, and cellular immunity response. Infants and children also have been identified as being infected with HPV. Infants can be infected in utero and by passage through an infected birth canal. HPV infection in children has been traced to child sexual abuse; however, reports vary in making this connection. 73. Pancreatic enzymes ( c 40,pg 1415) ➢ pancreatic enzymes hydrolyze proteins (proteases), carbohydrates (amylases), and fats (lipases). The proteases include trypsin, chymotrypsin, carboxypeptidase, and elastase. These enzymes are secreted in their inactive forms—that is, as trypsinogen, chymotrypsinogen, and procarboxypeptidase—to protect the pancreas from the digestive effects of its own enzymes. ➢ pancreatic enzymes (proteases, amylase, and lipase), and bile salts act in the small intestine to digest proteins, carbohydrates, and fats. 74. Process of muscle contraction( c 43,pg 1533) ➢ Muscle contraction is a four-step process: excitation, coupling, contraction, and relaxation. The initial contraction process is the excitation-contraction coupling (ECC) series, which involves the electrical properties of all cells and the movement of ions across the plasma membrane ➢ Excitation, the first step of muscle contraction, begins with the spread of an action potential from the nerve terminal to the neuromuscular junction. ➢ Following depolarization of the T-tubules, the second stage, coupling, occurs. This stage consists of the migration of calcium ions to the myofilaments. Calcium affects troponin and tropomyosin, muscleproteins that bind with actin when the muscle is at rest. ➢ Contraction begins as the calcium ions combine with troponin, a reaction that overcomes the inhibitory function of the troponin-tropomyosin system. The thin filament actin then slides toward the thick filament myosin. ➢ relaxation, begins as the sarcoplasmic reticulum absorbs the calcium molecules, removing them from interaction with troponin. Calcium is pumped back into the sarcoplasmic reticulum by means of an active transport process. The cross-bridges detach, and the sarcomere lengthens. 75. Cervical dysplasia (C 24,pg 825) ➢ Cervical dysplasia (cervical intraepithelial neoplasia [CIN]) a condition characterized by the appearance of abnormal cervical cells that are considered precancerous. ➢ It is established that cervical cancer is almost exclusively caused by cervical human papillomavirus (HPV) infection. Infection with “high-risk” (oncogenic) types of HPV (predominantly 16 and 18) is a necessary precursor to development of the precancerous cell changes, known as dysplasia, of the cervix that leads to invasive cancer ➢ these cell changes can be detected noninvasively through examination of the cervical cells. The cells can be destroyed to prevent cancer development if dysplasia can be detected early. 76. Consanguinity- (c4,pg 156) ➢ Consanguinity is sometimes present in families with autosomal recessive diseases, and it becomes more prevalent with rarer recessive diseases. ➢ Consanguinity and inbreeding are related concepts. Consanguinity refers to the mating of two related individuals, and the offspring of such mating are said to be inbred. Consanguinity is often an important characteristic of pedigrees for recessive diseases because relatives share a certain proportion of genes received from a common ancestor. The proportion of shared genes depends on the closeness of their biologic relationship. For example, siblings share one half of their DNA, on average, because of their descent from the same parents. 77. Nephrotic syndrome ( chap 38) ➢ Nephrotic syndrome is the excretion of 3.0 g or more of protein in the urine per day, hypoalbuminemia (less than 3.0 g/dl), and peripheral edema. Nephrotic syndrome is characteristic of glomerular injury. ➢ Primary causes of nephrotic syndrome include minimal change disease (lipoid nephrosis), membranous glomerulonephritis, and focal segmental glomerulosclerosis. ➢ Secondary forms of nephrotic syndrome occur in systemic diseases including diabetes mellitus, amyloidosis, systemic lupus erythematosus, and Henoch-Schönlein purpura. Nephrotic syndrome also is seen with certain drugs, infections, malignancies, and vascular disorders ➢ S/S of nephrotic syndrome -hematuria -urinary casts -leukocytes -low GFR -oliguria -azotemia (build up of waste products) -HTN [Show More]
Last updated: 1 year ago
Preview 1 out of 20 pages
Reviews( 0 )
Recommended For You
*NURSING> STUDY GUIDE > NUR2356 / NUR 2356 Multidimensional Care Exam 2 Final Exam Study Guide. Rasmussen College (All)
 Rasmussen College.png)
NUR2356 / NUR 2356 Multidimensional Care Exam 2 Final Exam Study Guide. Rasmussen College
NUR2356 / NUR 2356: Multidimensional Care Exam 2 / MDC 2 Final Exam Study Guide (Fall 2020) Rasmussen College
By Good grade , Uploaded: Sep 18, 2020
$10
*NURSING> STUDY GUIDE > NR599 / NR 599 Nursing Informatics for Advanced Practice - Comprehensive Final Exam Study Guide (Latest 2021 /2022):Chamberlain (All)
NR599 / NR 599 Nursing Informatics for Advanced Practice - Comprehensive Final Exam Study Guide (Latest 2021 /2022):Chamberlain
NR599 Nursing Informatics: Comprehensive Final Exam Study Guide
By quiz_bit , Uploaded: Feb 17, 2021
$10
*NURSING> STUDY GUIDE > NUR 2058 / NUR2058 Dimensions of Nursing Practice Final Exam Study Guide | Rated A |Rasmussen College (All)
NUR 2058 / NUR2058 Dimensions of Nursing Practice Final Exam Study Guide | Rated A |Rasmussen College
NUR 2058 / NUR2058 Dimensions of Nursing Practice Final Exam Study Guide | Rated A |Rasmussen College Nursing is activities that manipulates the environment and helps client achieve the balanced st...
By nurse_steph , Uploaded: Dec 05, 2020
$13.5
*NURSING> STUDY GUIDE > NR602 / NR 602 Primary Care of the Childbearing and Childrearing Family Practicum Final Exam Study Guide | Highly Rated | LATEST| Chamberlain College (All)
NR602 / NR 602 Primary Care of the Childbearing and Childrearing Family Practicum Final Exam Study Guide | Highly Rated | LATEST| Chamberlain College
NR602 / NR 602 Primary Care of the Childbearing and Childrearing Family Practicum Final Exam Study Guide | Highly Rated | LATEST| Chamberlain College Eye Disorders Strabismus- a defect in In oc...
By nurse_steph , Uploaded: Feb 07, 2021
$13
*NURSING> STUDY GUIDE > NR601 / NR 601 Primary Care of the Maturing and Aged Family Practicum Final Exam Study Guide | Week 5-7 | Highly Rated | LATEST | Chamberlain College of Nursing (All)
NR601 / NR 601 Primary Care of the Maturing and Aged Family Practicum Final Exam Study Guide | Week 5-7 | Highly Rated | LATEST | Chamberlain College of Nursing
NR601 / NR 601 Primary Care of the Maturing and Aged Family Practicum Final Exam Study Guide | Week 5-7 | Highly Rated | LATEST | Chamberlain College of Nursing Week 5 : Glucose Metabolism Disorders...
By nurse_steph , Uploaded: Feb 07, 2021
$13
*NURSING> STUDY GUIDE > NR 507 / NR507 Advanced Pathophysiology Week 2 Study Guide | Rated A | LATEST | Chamberline College (All)
NR 507 / NR507 Advanced Pathophysiology Week 2 Study Guide | Rated A | LATEST | Chamberline College
Respiratory disorders and alterations in acid-base fluid balance and electrolytes: Water balance: Solvent= water Solute= any substance in water Solution/fluid= water and the substance in it...
By nurse_steph , Uploaded: Feb 07, 2021
$10
*NURSING> STUDY GUIDE > NR511 / NR 511 Differential Diagnosis and Primary Care Practicum Final Exam Study Guide| Highly Rated | Latest | Chamberlain College (All)
NR511 / NR 511 Differential Diagnosis and Primary Care Practicum Final Exam Study Guide| Highly Rated | Latest | Chamberlain College
NR511 / NR 511 Differential Diagnosis and Primary Care Practicum Final Exam Study Guide| Highly Rated | Latest | Chamberlain College 1. Signs and symptoms and management of thyroid disorders Hy...
By nurse_steph , Uploaded: Mar 02, 2021
$13
*NURSING> STUDY GUIDE > NSG6430 Final Exam South University NSG 6430 Final Exam Study Guide (All)
NSG6430 Final Exam South University NSG 6430 Final Exam Study Guide
NSG6430 Final Exam South University NSG 6430 Final ExamStudy Guide
By khalid11 , Uploaded: Sep 29, 2023
$13
*NURSING> STUDY GUIDE > NR 503 Week 8 Final Exam Study Guide | Download For best results (All)
NR 503 Week 8 Final Exam Study Guide | Download For best results
NR 503 Week 8 Final Exam Study Guide | Download For best results
By A+ Solutions , Uploaded: Feb 02, 2022
$10
*NURSING> STUDY GUIDE > NR 503 Week 8 Final Exam Study Guide; Chapter 2-4, 5-6, 7-8, 9-15, 16-20 (100% Verified Correct Solutions) (All)
NR 503 Week 8 Final Exam Study Guide; Chapter 2-4, 5-6, 7-8, 9-15, 16-20 (100% Verified Correct Solutions)
NR 503 Week 8 Final Exam Study Guide; Chapter 2-4, 5-6, 7-8, 9-15, 16-20 Chapters 2-4 Which of the following is a condition which may occur during the incubation period? Chicken pox is a hi...
By A+ Solutions , Uploaded: Feb 02, 2022
$16
Document information
Connected school, study & course
About the document
Uploaded On
Apr 20, 2021
Number of pages
20
Written in

Additional information
This document has been written for:
Uploaded
Apr 20, 2021
Downloads
0
Views
51