AGNP BOARD EXAM: Dermatology Prescription (100 Questions and Answers)
Document Content and Description Below
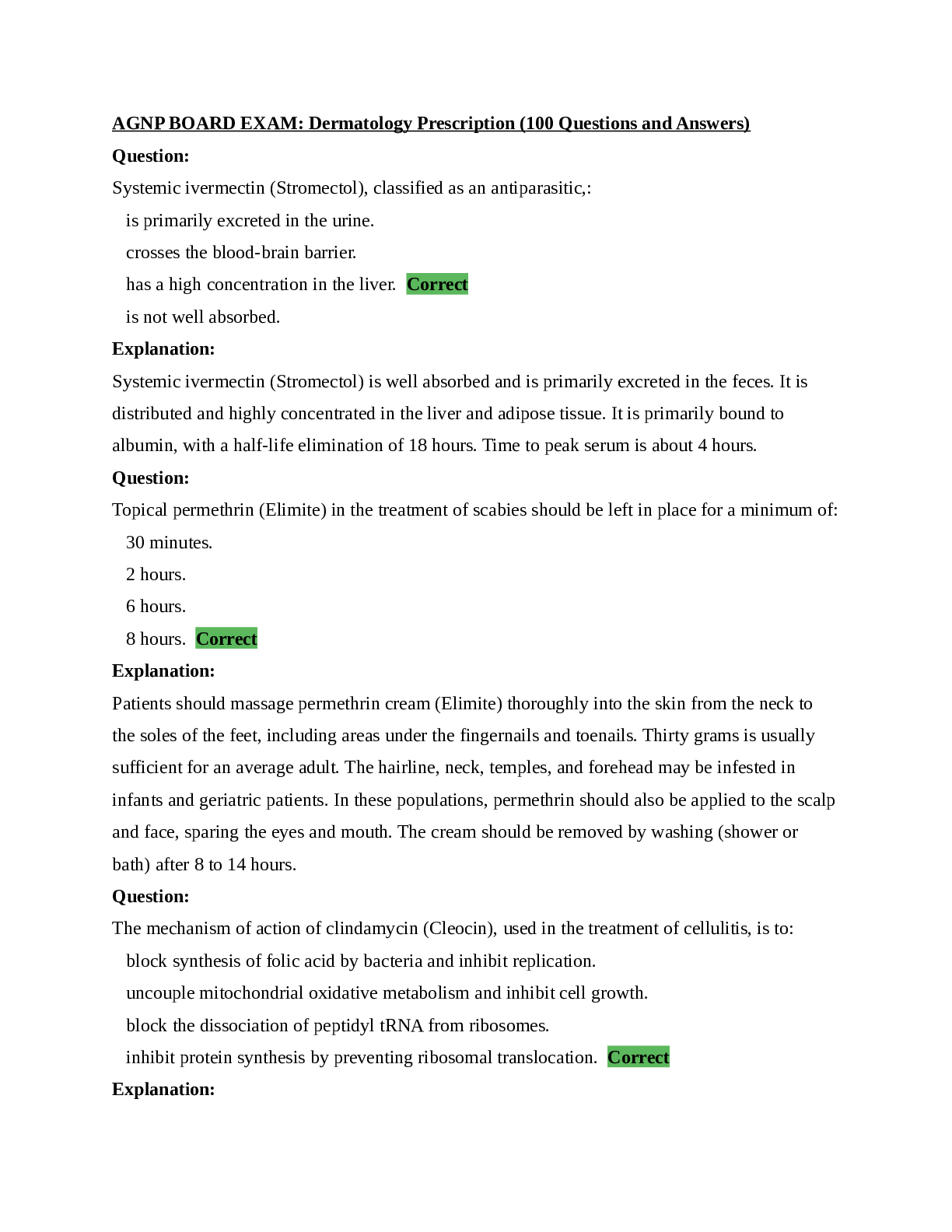
AGNP BOARD EXAM: Dermatology Prescription (100 Questions and Answers) Question: Systemic ivermectin (Stromectol), classified as an antiparasitic,: is primarily excreted in the urine. crosses the... blood-brain barrier. has a high concentration in the liver. Correct is not well absorbed. Explanation: Systemic ivermectin (Stromectol) is well absorbed and is primarily excreted in the feces. It is distributed and highly concentrated in the liver and adipose tissue. It is primarily bound to albumin, with a half-life elimination of 18 hours. Time to peak serum is about 4 hours. Question: Topical permethrin (Elimite) in the treatment of scabies should be left in place for a minimum of: 30 minutes. 2 hours. 6 hours. 8 hours. Correct Explanation: Patients should massage permethrin cream (Elimite) thoroughly into the skin from the neck to the soles of the feet, including areas under the fingernails and toenails. Thirty grams is usually sufficient for an average adult. The hairline, neck, temples, and forehead may be infested in infants and geriatric patients. In these populations, permethrin should also be applied to the scalp and face, sparing the eyes and mouth. The cream should be removed by washing (shower or bath) after 8 to 14 hours. Question: The mechanism of action of clindamycin (Cleocin), used in the treatment of cellulitis, is to: block synthesis of folic acid by bacteria and inhibit replication. uncouple mitochondrial oxidative metabolism and inhibit cell growth. block the dissociation of peptidyl tRNA from ribosomes. inhibit protein synthesis by preventing ribosomal translocation. Correct Explanation: Sulfa agents block synthesis of folic acid by bacteria and thus inhibit bacterial replication. First- generation cephalosporins inhibit cell wall synthesis of bacteria. Antifungals uncouple mitochondrial oxidative metabolism and inhibit cell growth. Macrolides inhibit bacterial growth, possibly by blocking dissociation of peptidyl tRNA from ribosomes, causing RNA-dependent protein synthesis to arrest. Other antibacterials are bacteriostatic or bactericidal and inhibit protein synthesis by preventing ribosomal translocation. Question: Tretinoin topical (Retin-A) is indicated for the treatment of acne vulgaris and: acne rosacea. dermatomyositis. inflammatory keratosis pilaris. mottled hyperpigmentation. Correct Explanation: Tretinoin topical (Retin-A) is indicated for the treatment of acne vulgaris, palliation of fine wrinkles, mottled hyperpigmentation and facial skin roughness. Question: The brand name of oral isotretinoin is: Duac. Absorica. Correct Accolate. Accupril. Explanation: The brand names of oral isotretinoin include Absorica, Amnesteem, Claravis, and Zenatane. The generic name for Duac is clindamycin/benzoyl peroxide, used in the treatment of acne. The generic name for Accolate is zafirlukast. It is a leukotriene inhibitor used in the treatment of asthma. The generic name for Accupril is quinapril; it is an ACE inhibitor. Question: Benzoyl peroxide (Benzac wash) is classified as a topical: antibiotic. astringent. antimicrobial. Correct acetic acid-based cleanser. Explanation: Benzoyl peroxide is a topical antimicrobial used in the treatment of acne. When applied to the skin, benzoyl peroxide works by reducing the amount of acne-causing bacteria and by causing the skin to dry and peel. Question: The generic name for Elidel is: permethrin. pimecrolimus. Correct tacrolimus. urea topical. Explanation: The generic name for Elidel is pimecrolimus. Elidel is a dermatologic agent used in the treatment of atopic dermatitis. The brand name of permethrin is Nix or Elimite. It is an antiparasitic used in the treatment of lice. The brand name for tacrolimus is Prograf. It is an immunosuppressive drug used after transplant. The brand name of urea topical is Keralac and it is used in the treatment of hyperkeratosis. Question: Which of the following conditions is NOT a side effect of long-term use of topical steroids? Cutaneous atrophy Glaucoma Hypotrichosis Correct Telangiectasia Explanation: Cutaneous and systemic side effects can occur, particularly with super potent and potent drugs, or extensive use of lower potency agents with or without occlusion. Treatment with topical corticosteroids should be restricted to the lowest and shortest duration of therapy required to achieve the desired effect. Cutaneous atrophy, telangiectasia, hypertrichosis, striae, purpura, hypopigmentation, glaucoma, and suppression of the hypothalamic-pituitary axis are side effects that may occur with topical corticosteroid use. Question: Patients using fluorouracil (Carac) for the treatment of actinic keratosis should be advised to expect: hypopigmentation. eczema. pustular formation. vesiculation. Correct Explanation: When fluorouracil (Carac) is applied to a lesion, erythema followed by vesiculation, desquamation, erosion and re-epithelialization occurs. Local reactions and alterations in skin appearance may persist for several weeks after discontinuation. Question: Tetracycline (Sumycin) is used in the treatment of skin and skin structure infections caused by: Bartonella bacilliformis. Klebsiella species. Escherichia coli. Staphylococcus aureus. Correct Explanation: Tetracycline (Sumycin) is indicated for the treatment of skin and skin structure infections caused by Staphylococcus aureus or Staphylococcus pyogenes (commonly found in post burn infections). Question: The most appropriate therapy for patients with chronic paronychia is a: systemic antifungal. systemic glucocorticoids. topical steroid. Correct topical antibiotic. Explanation: Chronic paronychia appears to be an eczematous process that can be complicated by secondary Candida infection. Avoidance of environmental triggers is an essential component of treatment. Patients should wear gloves during wet work and should avoid contact with irritating substances. Topical treatment consists of the application of a medium or high-potency topical corticosteroid. If patients do not improve with these measures, a course of topical antifungal therapy may be combined with topical steroid. Question: The use of tetracycline in children younger than 9 years with a bacterial skin infection, may cause: dental enamel hyperplasia. hypopigmentation. serum sickness. reduced bone growth. Correct Explanation: Pediatric use may cause bone growth retardation, tissue hyperpigmentation, enamel hypoplasia, or permanent tooth discoloration; use of tetracyclines should be avoided during tooth development (children <8 years of age) unless other drugs are not likely to be effective or are contraindicated. Question: Daily doses of oral corticosteroids, such as prednisone, should be administered: early in the morning. Correct at noon. with dinner. at bedtime. Explanation: The maximal activity of the adrenal cortex is between 2 am and 8 am, and it is minimal between 4 pm and midnight. Exogenous corticosteroids suppress adrenocorticoid activity the least when given at the time of maximal activity (am) for single dose administration. Therefore, it is recommended that prednisone be administered in the morning prior to 9 am. Question: The mechanism of action of sulfa agents, in the treatment of cellulitis, is to: block synthesis of folic acid by bacteria and inhibit replication. Correct uncouple mitochondrial oxidative metabolism and inhibit cell growth. block the dissociation of peptidyl tRNA from ribosomes. inhibit protein synthesis by preventing ribosomal translocation. Explanation: Sulfa agents block synthesis of folic acid by bacteria and thus inhibit bacterial replication. First- generation cephalosporins inhibit cell wall synthesis of bacteria. Antifungals uncouple mitochondrial oxidative metabolism and inhibit cell growth. Macrolides inhibit bacterial growth, possibly by blocking dissociation of peptidyl tRNA from ribosomes, causing RNA-dependent protein synthesis to arrest. Other antibacterials are bacteriostatic or bactericidal and inhibit protein synthesis by preventing ribosomal translocation. Question: Topical salicylic acid, a keratolytic: can be used for genital warts. should be applied once weekly. is safe for use on the face. should not be used in areas with poor blood circulation. Correct Explanation: Topical salicylic acid should not be used on irritated skin or on any area that is infected or reddened; on moles, birthmarks, warts with hair growing from them, genital warts or warts on the face or mucous membranes; or for patients with diabetes or with poor blood circulation. Application is once or twice daily for up to 12 weeks. Question: Retapamulin (Altabax), used in the treatment of impetigo, is NOT: a topical antibiotic. effective against Streptococcus pyogenes. to be applied intranasally or to mucosa. Correct for use in children. Explanation: Retapamulin (Altabax) is for external use only and is not for intranasal, intravaginal, ophthalmic, oral, or mucosal application. It is a topical antibiotic, bacteriostatic agent used for the treatment of impetigo due to Staphylococcus aureus (methicillin-susceptible isolates only) or Streptococcus pyogenes in adults and patients 9 months and older. Question: Initial treatment for irritant contact dermatitis is a: low-potency topical steroid. Correct medium-potency topical steroid. high-potency topical steroid. super high-potency topical steroid. Explanation: Low-potency corticosteroids are indicated for the initial treatment of irritant contact dermatitis. Additionally, the patient should be advised to avoid future exposure to the irritant. Moisturizers without fragrance, antibacterials, or urea are preferred as these substances often cause sensitization. Question: The brand name of clindamycin and benzoyl peroxide topical for the treatment of acne is: Cleocin T. Desonate. Duac. Correct Benzamycin. Explanation: The brand names for the topical combination of clindamycin and benzoyl peroxide include Acanya, BenzaClin, Duac, and Onexton. Benzamycin is the brand name for benzoyl peroxide and erythromycin. Cleocin T is the brand name for clindamycin topical. Desonate is the brand name for desonide, a topical steroid. Question: Dosage reductions should be considered when prescribing first-generation cephalosporins for patients with: hepatic insufficiency. diabetes. cardiomyopathy. renal insufficiency. Correct Explanation: All cephalosporins require dose adjustments in the presence of severe renal failure. BUN and creatinine should be checked at baseline and periodically, especially if the patient is an older adult. First generation cephalosporins are excreted in the urine >90% unchanged. The half-life of the drug is increased in patients with severe renal disease. Question: Diclofenac (Solaraze), a topical anti-inflammatory, is used in the treatment of: actinic keratosis. Correct acne vulgaris. contact dermatitis. eczema. Explanation: Diclofenac (Solaraze) is indicated for the treatment of actinic keratoses. Diclofenac (Solaraze) is applied to lesion areas twice daily. It is to be smoothed onto the affected skin gently. The amount needed depends upon the size of the lesion site. Question: Antiviral agents for the treatment of herpes zoster: are most effective when started within 48-72 hours of outbreak. Correct should not be initiated after 72 hours. do not prevent postherpetic neuralgia. do not reduce the risk of transmission of the virus through shedding. Explanation: Antiviral therapy should be initiated within 48-72 hours of onset of to maximize the potential benefits of treatment. The goals of antiviral therapy in the treatment of herpes zoster is to: lessen the severity and duration of pain associated with acute neuritis; promote more rapid healing of skin lesions; prevent new lesion formation; decrease viral shedding to reduce the risk of transmission; and prevent postherpetic neuralgia. The administration of antiviral therapy after 72 hours is recommended if new lesions are appearing at the time of presentation, as this indicates ongoing viral replication. There is likely minimal benefit of antiviral therapy in the patient who has lesions that have encrusted. Question: A side effect of benzoyl peroxide (Benzac wash) is: hyperpigmentation. bleaching of eyebrows. Correct oily skin. hypopigmentation. Explanation: Benzoyl peroxide (Benzac wash) may bleach hair or fabrics. Advise patients to avoid contact with hair, clothing, and furnishings. Skin reactions such as peeling, itching, irritation, and reddening may occur. Question: Which of the following is NOT appropriate advice for the patient using benzoyl peroxide (Benzagel)? Discontinue use for mild peeling or redness Correct Avoid the use of tanning beds Wear sunscreen Test skin in 1-2 small areas prior to full use Explanation: Skin irritation (e.g., burning, itching, peeling, redness, swelling) may occur with benzoyl peroxide treatment; it should be discontinued if severe irritation develops. Dosing or frequency may need to be temporarily decreased until irritation resolves. When treatment resumes, the drug may titrated up to three times daily if needed. Tanning beds should be avoided while using benzoyl peroxide. Patients should be advised to wear sunscreen and to test a small area prior to full use of the cream. Question: Clindamycin (Cleocin) should NOT be administered with: buspirone (Buspar). erythromycin (Ilotycin). Correct rifampin (Rifadin). ibuprofen (Advil). Explanation: Antagonism has been demonstrated between clindamycin and erythromycin in vitro. Because of possible clinical significance, these two drugs should not be administered concurrently. It is safe to administer with buspirone (Buspar), rifampin (Rifadin) and ibuprofen (Advil). Question: Moderate irritant contact dermatitis to the face should be treated with a: medium-potency topical steroid. Correct high-potency topical steroid. super high-potency topical steroid. oral corticosteroids. Explanation: For acute or chronic irritant contact dermatitis involving the face or flexural areas, a medium- or low-potency topical corticosteroid is recommended. Question: Patients treated with sulfamethoxazole and trimethoprim (Bactrim) should be advised to take it: with 8 ounces of water. Correct with food. on an empty stomach. with folic acid. Explanation: Patients who are treated with sulfamethoxazole and trimethoprim (Bactrim) should be advised to take it with 8 oz of water. Patients should be instructed to maintain an adequate fluid intake in order to prevent crystalluria and stone formation. It may be taken without regard to meals. Question: A breastfed infant has been diagnosed with oral candidiasis. Which of the following statements is true? Do not feed the infant for at least 1 hour after application of nystatin oral suspension. Nystatin oral suspension is not for prolonged use and should not be administered for more than 3-5 days. The mother should be treated prophylactically with fluconazole (Diflucan). Treatment with nystatin oral suspension should be continued for at least 48 hours after symptoms have disappeared. Correct Explanation: Treatment with nystatin oral suspension should be continued for at least 48 hours after symptoms of oral candidiasis have disappeared. Nystatin oral suspension should be applied to the infant's mouth 4 times daily (1 ml of 200,000 units in each side of mouth) and feeding avoided for 5-10 minutes. It is well tolerated even with prolonged use. The mother should NOT be prophylactically treated. Question: Fluorouracil (Carac), for treatment of actinic keratosis, is classified as a(n): anti-inflammatory. antibiotic. antineoplastic. Correct steroid. Explanation: Fluorouracil (Carac) is classified as an antineoplastic. It is used in the treatment of actinic keratosis. Question: Ciclopirox (Loprox) shampoo for the treatment of seborrheic dermatitis should be applied: daily. twice daily. weekly. twice weekly. Correct Explanation: Ciclopirox (Loprox) shampoo should be applied to wet hair (5 mL or 10 mL for longer hair). Lather and leave on hair and scalp for approximately 3 minutes, then rinse. Application should be repeated twice weekly for 4 weeks. Allow a minimum of 3 days between applications; if no improvement after 4 weeks of treatment, re-evaluate diagnosis. Question: Which of the following antibiotics is NOT approved for the treatment of acne vulgaris? Azithromycin (Zithromax) Doxycycline (Doryx) Metronidazole (Flagyl) Correct Trimethoprim-sulfamethoxazole (Bactrim DS) Explanation: Oral antibiotics used in the treatment of acne include tetracycline, doxycycline, minocycline, erythromycin, trimethoprim-sulfamethoxazole, clindamycin, and azithromycin. Metronidazole (Flagyl) is not indicated in the treatment of acne vulgaris. Question: The greatest concern with long-term use of topical corticosteroids is: purpura. rosacea-like eruptions. acneiform eruptions. skin atrophy. Correct Explanation: Cutaneous side effects include purpura, telangiectasia, striae, focal hypertrichosis, and acneiform or rosacea-like eruptions. Of greatest concern is skin atrophy, which can be induced by any topical corticosteroid. Higher-potency agents, occlusion, use on thinner skin, and older patient age increase this risk. Question: Patients with comedonal noninflammatory acne should be treated with a topical: retinoid. Correct antibiotic. antimicrobial. antimicrobial/antibiotic combination. Explanation: A topical retinoid or salicylic acid is the recommended therapy for treatment of comedonal noninflammatory acne. Antibiotics and antimicrobials are indicated in inflammatory conditions. Question: Dynacin, used in the treatment of skin infections, is the brand name for: tetracycline. doxycycline. minocycline. Correct demeclocycline. Explanation: Dynacin, Minocin, Solodyn are all brand name for minocycline. Minocycline is classified as a tetracycline. It is used in the treatment of acne and some skin infections. Question: Tretinoin topical gel (Atralin) should be used cautiously in patients who are allergic to: eggs. peanuts. fish. Correct strawberries. Explanation: Atralin gel contains soluble fish proteins; use caution in patients with sensitivities or allergies to fish. Question: A patient received a prescription for clindamycin/benzoyl peroxide topical with orders to dispense 2 containers. Until ready for the use, the patient should store the additional container: in the freezer. at room temperature. in the refrigerator. Correct in a warm, dry place. Explanation: Prior to use of clindamycin/benzoyl peroxide topical (Duac) it should be stored in a cold place, preferably in a refrigerator, between 2°C and 8°C (36°F and 46°F; not in a freezer). The container that is in use should be stored at room temperature and discarded at the 60 day expiration date. Question: Given the same percentage and type of topical corticosteroid, the vehicle with the highest potency would be the: cream. lotion. ointment. Correct gel. Explanation: Given the same percentage and type of topical corticosteroid, the strengths of the medication are, from highest to lowest: ointment, gels, creams, and lotions. An ointment base is more occlusive and will drive the medication into the skin more rapidly than a solution or a cream base. Question: Patients should be advised that clindamycin (Cleocin) should be administered with: a full glass of water. Correct lactobacillus. food. milk. Explanation: Clindamycin (Cleocin) should be administered with a full glass of water to minimize esophageal ulceration. Coadministration with food does not adversely affect the absorption of clindamycin- flavored granules. An unpleasant or metallic taste has been reported after oral administration regardless of whether taken with food. Question: The body surface area with the LEAST ability to absorb topical steroids is: the axillae. the face. the groin. the palms. Correct Explanation: The areas with greatest absorption of steroid are the face, groin and axillae. The palms of the hands are least absorptive. Question: The most troublesome adverse reaction to clindamycin (Cleocin), used in the treatment of cellulitis, is: esophageal ulcerations. nephrotoxicity. Clostridium difficile-related colitis. Correct photosensitivity. Explanation: The most troublesome adverse reaction of clindamycin is diarrhea related to C. difficile-related colitis. This drug has rarely caused drug fever, rash, blood dyscrasias, or hepatotoxicity. Nephrotoxicity has been seen with vancomycin (Vancocin). Doxycycline (Doryx) has been associated with esophageal ulcerations and photosensitivity. Question: The best treatment for mild cellulitis caused by methicillin-resistant Staphylococcus aureus is: topical mupirocin (Bactroban). oral amoxicillin/clavulanate (Augmentin). oral trimethoprim-sulfamethoxazole (Bactrim). Correct oral cephalexin (Keflex). Explanation: The best treatment for mild cellulitis caused by methicillin-resistant Staphylococcus aureus is oral trimethoprim-sulfamethoxazole (Bactrim). Question: The preferred treatment for Lyme disease in a 16-year-old male is: amoxicillin (Amoxil). azithromycin (Zithromax). clarithromycin (Biaxin). doxycycline (Vibramycin). Correct Explanation: The preferred treatment for erythema migrans (early Lyme disease) is doxycycline (Vibramycin). Doxycycline is generally preferred because it is also effective against A. phagocytophilum, which causes human granulocytic anaplasmosis. However, doxycycline should be avoided in pregnant women and children younger than 8 years; amoxicillin (Amoxil) or cefuroxime axetil (Ceftin) is preferred in such patients. Question: The most effective way to assure that the patient has enough topical corticosteroid for the duration of treatment is to: give the largest tube available. give one refill for every 2 days of use. determine the amount needed using the fingertip unit (FTU). Correct determine the amount based on 0.1 grams per square inch needed to cover. Explanation: Assuming that a proper diagnosis is made, one of the most common treatment errors is suboptimal medication use related to improper medication strength, improper vehicle, or insufficient dosage. The most effective way to assure that the patient has enough topical corticosteroid for the duration of treatment is to use the Fingertip Unit (FTU). This is a convenient method to estimate the amount of a topical preparation to be used per application. Question: Which of the following medications for the treatment of acne is extended-release and is dosed according to weight? Rifampin (Rifadin) Metronidazole (Flagyl) Clindamycin (Cleocin) minocycline (Minocin) Correct Explanation: A once-daily, extended-release formulation of minocycline (Minocin) is prescribed as a weight- based dose. The lowest effective dose with the most favorable side effect profile is 1 mg/kg/day; higher doses do not offer additional benefit. Extended-release minocycline is available as 45, 90, and 135 mg tablets as a generic and in additional tablet doses as a brand. Question: To assure maximum efficacy in the treatment of actinic keratosis, fluorouracil (Carac) should be applied for at least: 4 days. 4 weeks. Correct 6 weeks. 8 weeks. Explanation: Fluorouracil (Carac) is indicated in the treatment of actinic keratosis. Fluorouracil is classified as an antineoplastic. It should be applied daily for 1-4 weeks. Continued treatment up to 4 weeks results in greater lesion reduction. Question: A 23-year-old man has completed 12 weeks of therapy with clindamycin/benzoyl peroxide topical for acne. He should be advised to return immediately if he develops: dizziness. xeroderma. abdominal pain and diarrhea. Correct muscle pain and weakness. Explanation: Clindamycin/benzoyl peroxide topical (Duac) may be absorbed into the bloodstream. Although Clostridium difficile associated diarrhea is rare, it may occur and would cause abdominal pain and diarrhea. This condition may occur weeks after treatment has stopped. Severe dizziness may be associated with an allergic reaction to the medication. Xeroderma is a potential side effect but would occur during use of the medication. Muscle pain and weakness is not associated with the use of this medication. Question: Due to potential systemic absorption, the use of fluorouracil (Carac) should be avoided in patients who: have anemia. are pregnant. Correct have renal insufficiency. have a history of seizures. Explanation: Adverse effects have been reported following use of topical fluorouracil products in humans. Use is contraindicated during pregnancy. Women of reproductive potential should use effective contraception during and for 1 month after the final application of topical fluorouracil. Question: Topical corticosteroids, used to treat various skin conditions,: do not suppress the immune system. possess anti-inflammatory properties. Correct do not cause systemic side effects. are safe to use during pregnancy. Explanation: Topical corticosteroids have potent anti-inflammatory properties and also suppress the immune response. Topical corticosteroids are used based on their potency, the area of the body to which they will be applied, and type of skin condition being treated. Most topical corticosteroids are considered safe to use during pregnancy. However, using very potent topical corticosteroids is not usually recommended during pregnancy, because research has found they may increase the risk of a low birthweight infant. Question: Patients should be advised that after an intralesional corticosteroid injection, they should expect: swelling, redness and warmth in the area. possible hyper- or hypopigmentation. Correct complete resolution of the lesion within 1 week. sloughing of the skin. Explanation: Patients should be advised that after an intralesional corticosteroid injection, they should expect possible atrophy and hypopigmentation, the most common side effects. Atrophy and pigment changes usually resolve over several weeks but occasionally persist longer and are sometimes permanent. Swelling, redness and warmth may indicate an infection in the area, and the patient should return to the clinic. Patients should be advised that the first treatment may not be completely effective and more than one injection may be necessary. Injecting too high in the skin, in the upper dermis and epidermis, may cause sloughing of the skin and may require "flushing" of the corticosteroid. Question: Imiquimod (Aldara) is indicated for the treatment of: acne. actinic keratosis. Correct erysipelas. keloids. Explanation: Imiquimod (Aldara) is indicated for the treatment of actinic keratosis, perianal warts/condyloma acuminata, and superficial basal cell carcinoma. Question: Benzoyl peroxide (Benzagel) is indicated for the treatment of: hyperpigmentation. mild acne and rosacea. Correct dermatomyositis. severe acne vulgaris. Explanation: Benzoyl peroxide (Benzagel) is indicated in the treatment of mild to moderate acne vulgaris and acne rosacea Question: Patients using diclofenac (Solaraze) should be advised to expect optimal therapeutic effect of actinic keratoses within: 2 weeks of continuous application. 4 weeks of continuous application. 6 weeks of continuous application. 1 month following cessation of therapy. Correct Explanation: Diclofenac (Solaraze) is applied to lesion areas twice daily. It is to be smoothed onto the affected skin gently. The amount needed depends upon the size of the lesion site. Assure that enough Solaraze is applied to adequately cover each lesion. Typically 0.5 g of gel is used on each 5 cm x 5 cm lesion site. The recommended duration of therapy is 60 days to 90 days. Complete healing of the lesion(s) or optimal therapeutic effect may not be evident for up to 30 days following cessation of therapy. Lesions that do not respond to therapy should be carefully re-evaluated and management reconsidered. Question: Which statement about the action of silver sulfadiazine (Silvadene) cream is TRUE? It acts by inhibiting cell wall synthesis. It is a carbonic anhydrase inhibitor. It inhibits folic acid synthesis. It acts by damaging the cell membrane and cell wall. Correct Explanation: Mechanism of action of silver sulfadiazine (Silvadene) is unknown; however, it is thought to act by damaging the cell membrane and cell wall to produce its bactericidal effect and does not inhibit cell wall synthesis. Silver sulfadiazine is not a carbonic anhydrase inhibitor and may be useful in situations when such agents are contraindicated. Question: A potential systemic reaction to imiquimod (Aldara), used to treat superficial basal cell carcinomas, is: bradycardia. hypoglycemia. flu-like symptoms. Correct renal calculi. Explanation: Systemic effects of topical imiquimod (Aldara) have been reported and include malaise, fatigue and fever (flu-like symptoms). Effects may also include hyperglycemia, headaches, arrhythmias, joint pain and upper respiratory infections. Question: Patients with seborrheic dermatitis who have patchy, orange to salmon-colored plaques covered with scales should be treated with: topical antihistamines in combination with antifungal shampoo. a high-potency corticosteroid shampoo. Correct systemic glucocorticoids. systemic antifungals. Explanation: For patients with seborrheic dermatitis with itching and/or visible inflammation (patchy, orange to salmon-colored plaques covered with scale), a high-potency corticosteroid shampoo, lotion, or foam is recommended. The topical corticosteroid should be applied once daily for 2 to 4 weeks. Question: Intralesional corticosteroid injections should NOT be: diluted with lidocaine, a local anesthetic. injected into the dermis. injected into the subcutaneous tissue. Correct utilized for lesions in thin skinned areas such as the face. Explanation: Corticosteroids cause a burning sensation for up to 3 to 5 minutes after injection. Most corticosteroids are diluted prior to injection to minimize patient discomfort. Saline is an excellent diluent for all corticosteroids, but some clinicians prefer to dilute with the local anesthetic lidocaine. Long-acting anesthetics such as bupivacaine should not be used. Most pathology in inflammatory skin lesions is in the dermis, and it is in this layer of skin that corticosteroids should be deposited. Caution is needed to avoid injecting into subcutaneous tissue. Lesions in thin-skinned areas such as the face and central chest necessitate lower corticosteroid concentrations and smaller drug quantities. Question: Laboratory monitoring for a patient on cephalexin (Keflex) should include: urine microalbumin. PT/INR. Correct amylase. electrolytes. Explanation: Cephalexin (Keflex) may be associated with increased INR, especially in nutritionally deficient patients, with prolonged treatment, and in patients with hepatic or renal disease. Question: Prednisolone topical cream belongs to which of the following drug classes? Anabolic steroids Androgenic steroids Glucocorticoids Correct Mineralocorticoids Explanation: Prednisone is a glucocorticoid, a class of corticosteroids that are indicated for inflammatory dermatoses and suppress the immune response. They are used based on their potency, area of body to which they will be applied and the type of skin condition being treated. Additionally, they are readily absorbed from the gastrointestinal tract. Question: Silver sulfadiazine (Silvadene) cream, indicated for the treatment of burns, is: bacteriostatic. a broad-spectrum antimicrobial. Correct only a prophylactic measure to prevent infection. not recommended for third-degree burns. Explanation: Silver sulfadiazine (Silvadene) is a topical cream with broad antimicrobial activity. It is bactericidal for many gram-negative and gram-positive bacteria and is effective against yeast. Silvadene is indicated as an adjunct for the prevention and treatment of wound sepsis in patients with second- and third-degree burns. Question: The use of silver sulfadiazine (Silvadene) cream should be avoided in: patients older than 75 years. the presence of renal insufficiency. areas where skin grafting may be needed. pregnant women during the third trimester. Correct Explanation: Because sulfonamide therapy increases the possibility of kernicterus, silver sulfadiazine (Silvadene) cream 1% should not be used on pregnant women approaching or at term, on premature infants, or on newborn infants during the first 2 months of life. No overall differences in safety or effectiveness occur in older adults and younger subjects, and other reported clinical experience has not identified differences in responses between the older adult and younger patients. It is not contraindicated in areas that may require grafting. Patients with renal insufficiency should be monitored closely. Question: Dapsone (Aczone) topical 5% gel should be applied: daily in a dime-sized amount. twice daily in a nickel-sized amount. daily in a thumb-sized amount. twice daily in a pea-sized amount. Correct Explanation: Dapsone (Aczone) topical 5% gel, is a bacteriostatic agent used in the treatment of acne. Dapsone should be applied twice daily in a pea-sized amount. Dapsone topical 7.5% gel may be applied daily in a pea-sized amount. Question: The recommended first-line treatment of tinea capitis in a 5-year-old child is: griseofulvin (Grifulvin V). Correct fluconazole (Diflucan) systemic. ketoconazole (Nizoral) shampoo. moderate-dose topical steroids. Explanation: The systemic antifungal therapies for tinea capitis include griseofulvin (Grifulvin V), terbinafine (Lamisil), fluconazole (Diflucan), and itraconazole (Sporanox). Griseofulvin has a long history of use for childhood tinea capitis and is a well-accepted first-line therapy. Terbinafine is an acceptable alternative that may offer the advantage of shorter treatment courses. Fluconazole and itraconazole are effective, but less frequently used than griseofulvin and terbinafine. Only griseofulvin and terbinafine have formulations that are approved by the FDA for the treatment of tinea capitis. Question: Patients applying low-potency steroids to the face should be instructed to: apply 2-3 fingertips of the medication once daily for 7 days. apply a thin film 2-3 times daily for 7 days. Correct discontinue use if changes in skin color appear. discontinue use after 6 weeks even if the condition continues. Explanation: Generally, a thin film applied to the face 2-3 times daily for 7 days yields the best results. Discontinue use after 3 weeks. Changes in skin color may occur but usually resolve after discontinuation. Question: Lidocaine (Lidoderm) patch should NOT be prescribed for patients allergic to: benzocaine (Anbesol). bupivacaine (Marcaine). Correct tetracaine (Pontocaine). diphenhydramine (Dermarest). Explanation: Lidocaine (Lidoderm) patch should NOT be prescribed for patients allergic to bupivacaine (Marcaine), which is an amide-type anesthetic. Cross sensitivity among members of the amide- type local anesthetic group has been reported. Benzocaine (Anbesol) and tetracaine (Pontocaine) are both ester-type anesthetics. Diphenhydramine (Dermarest) is a topical antihistamine. Question: Topical permethrin should be avoided in patients with an allergy to: milk. peanuts. ragweed. Correct strawberries. Explanation: Pyrethroids, such as permethrin, have extremely low mammalian toxicity. Pyrethrins, derived from chrysanthemums, may cause breathing difficulties in patients with ragweed allergy. Therefore, permethrin use is not recommended in patients who are allergic to ragweed and chrysanthemums. Skin irritation is a potential side effect. Question: The most effective therapies in the treatment of acne related to increased sebum production are: benzoyl peroxide and topical antibiotics. benzoyl peroxide and oral antibiotics. oral tetracyclines and topical retinoids. hormonal therapies and isotretinoin. Correct Explanation: Androgens stimulate increased sebum production, which contributes to the formation of acne. Hormonal therapy may benefit women with moderate to severe acne, even in the absence of a hyperandrogenic state. Isotretinoin also can reduce sebum production. This medication is indicated in the treatment of severe, recalcitrant nodular acne and can cause skin dryness. Question: A potential adverse reaction related to the use of sulfacetamide (Klaron) topical, indicated for the treatment of seborrheic dermatitis, is: systemic lupus erythematous. Correct skin irritation. localized infection. renal insufficiency. Explanation: Sulfacetamide topical (Klaron) is a sulfonamide. The following potentially adverse reactions should be considered by the provider, regardless of the route administered. Severe reactions may include drug-induced systemic lupus erythematosus, agranulocytosis, acute hemolytic anemia, aplastic anemia, purpura hemorrhagic, Stevens-Johnson syndrome, toxic epidermal necrolysis, drug fever, fulminant hepatic necrosis and jaundice. Question: The addition of epinephrine to lidocaine hydrochloride: causes vasodilation. prolongs the duration of anesthesia. Correct reduces microorganism penetration. decreases the pain of the anesthetic injection. Explanation: The addition of epinephrine at 1:100,000 to 200,000 (5 to 10 µg per mL) is useful to prolong the duration of anesthesia and provide some degree of hemostasis. Question: High-potency topical corticosteroids: can be applied to the face. may be absorbed and cause systemic side effects. Correct may cause hypoglycemia. may cause hypotension. Explanation: Topically applied corticosteroids, particularly high- and very high-potency agents, can be absorbed at a degree sufficient to cause systemic side effects. The risk of hypothalamic-pituitary- adrenal axis suppression is low but increases with prolonged continuous use, especially in patients concurrently receiving corticosteroids in other forms (inhaled, intranasal, or oral). Hyperglycemia and hypertension are rarely reported. Question: First-generation cephalosporins for the treatment of bacterial skin infections: have a decreased risk of cross-reactivity in penicillin allergic patients in comparison to other cephalosporins. have broad coverage against both gram-positive and gram-negative organisms. primarily are effective against gram-positive organisms. Correct mostly decrease activity against gram-negative organisms. Explanation: First-generation cephalosporins (i.e. Keflex and Duracef) primarily are effective against gram- positive organisms. Only a few first-generation cephalosporins are effective against gram- negative organisms. First-generation cephalosporins also have an increased cross-reactivity risk in penicillin-allergic patients compared to other cephalosporins. Fourth-generation cephalosporins have broad coverage against both gram-positive and gram-negative organisms. Question: Which of the following is NOT a topical pediculicide? Benzyl alcohol (Ulesfia) Ivermectin (Stromectol) Permethrin (Elimite) Selenium sulfide (Selsun Blue) Correct Explanation: Topical pediculicides include permethrin (Elimite), malathion (Ovide), benzyl alcohol (Ulesfia), spinosad (Natroba) and ivermectin (Stromectol). Spinosad and ivermectin are rarely used due to high cost. Selenium sulfide is the active ingredient in Selsun Blue for dandruff. Question: Pediatric patients are at greater risk than adults for developing adrenal suppression related to topical steroid use due to their: higher metabolism. decreased lean muscle mass. higher ratio of skin surface area to body mass. Correct lower basal cortisol rates. Explanation: Because of a higher ratio of skin surface area to body mass, pediatric patients are at greater risk than adults for HPA axis suppression when they are treated with topical corticosteroids. They are also at greater risk for glucocorticosteroid insufficiency after treatment withdrawal for Cushing's syndrome while on treatment. Adverse effects, including striae, have been reported with inappropriate use of topical corticosteroids in infants and pediatric patients. Question: The patient receiving imiquimod (Aldara) topical for the treatment of actinic keratosis should be instructed to apply: daily for a maximum therapy duration of 16 weeks. daily, as long as it takes to resolve the lesions. every other day until lesions are resolved. twice weekly for maximum of 16 weeks. Correct Explanation: Treatment consists of twice weekly application for a maximum of 16 weeks. The medication should be applied prior to sleep and left on the skin for approximately 6-10 hours, then removed by washing the area with mild soap and water. Treatment should be continued for the full treatment course, even if all actinic keratoses appear to be gone. Lesions that do not respond to treatment should be carefully re-evaluated and management reconsidered. Question: A combination topical antimicrobial-antibiotic medication used in the treatment of acne is: benzoyl peroxide and erythromycin. Correct benzoyl peroxide and adapalene. benzoyl peroxide and tretinoin. benzoyl peroxide and dapsone. Explanation: A combination topical antimicrobial and antibiotic medication used in the treatment of acne is benzoyl peroxide (a topical antimicrobial) with erythromycin (a topical antibiotic). This is marketed under the brand name Benzamycin. Question: Children receiving griseofulvin (Grifulvin V) for the treatment of tinea capitis should be monitored for: alopecia. clay-colored stools. Correct tinea versicolor. tinnitus. Explanation: Griseofulvin (Grifulvin V) can cause hepatotoxicity. Elevations in AST, ALT, bilirubin, and jaundice have been reported with griseofulvin use. Signs and symptoms of hepatoxicity include nausea and vomiting, decreased appetite, dark-colored urine, clay-colored stools, fatigue, fever, stomach pain and jaundice. Patients should be monitored for hepatic adverse events and discontinuation of griseofulvin considered if warranted. Question: Which of the following statements about systemic clindamycin (Cleocin) is true? Dialysis is effective in removing clindamycin (Cleocin) from the serum. Clindamycin (Cleocin) adequately diffuses into the cerebrospinal fluid and is effective for the treatment of meningitis. Colitis related to clindamycin (Cleocin) may occur more than 2 months after cessation of therapy. Correct Clindamycin (Cleocin) is safe to prescribe to atopic patients. Explanation: Diarrhea is a common problem caused by antibiotics and usually ends when the antibiotic is discontinued. Some patients develop watery and bloody stools (with or without stomach cramps and fever) even as late as 2 or more months after taking the last dose of the antibiotic. Atopy (atopic syndrome) is a syndrome characterized by a tendency to be “hyperallergic.” Clindamycin (Cleocin) should be avoided in these patients. Question: Sulfamethoxazole and trimethoprim (Bactrim) should NOT be prescribed for patients who: have megaloblastic anemia due to folic acid deficiency. Correct have mild to moderate renal insufficiency. are between the ages of 2-6 years. have bronchial asthma. Explanation: Sulfamethoxazole and trimethoprim (Bactrim) is contraindicated in patients with a known hypersensitivity to trimethoprim or sulfonamides, in patients with a history of drug-induced immune thrombocytopenia with use of trimethoprim and/or sulfonamides, and in patients with documented megaloblastic anemia due to folate deficiency. It is contraindicated in patients younger than 2 months of age and patients with marked hepatic damage or with severe renal insufficiency when renal function status cannot be monitored. Caution should be used in the presence of mild to moderate renal insufficiency and patients with bronchial asthma. Question: The best medication choice for the treatment of acne in hairy areas is: clindamycin topical cream (Cleocin T). clindamycin topical lotion (Cleocin T). benzoyl peroxide/clindamycin gel (Clindagel). clindamycin phosphate (Clindamycin Foam). Correct Explanation: Foams are easier to apply to hairy areas. Gels have a more drying effect than other choices. Creams and lotions tend to be moisturizing. Solutions are drying, but are typically used to cover a large area. Question: An example of a first-generation cephalosporin is: cefixime (Suprax). ceftriaxone (Rocephin). ceftaroline (Teflaro). cephalexin (Keflex). Correct Explanation: Cephalexin (Keflex) is an example of a first-generation cephalosporin. Cefixime is second- generation, ceftriaxone is third-generation, and ceftaroline is a fifth-generation cephalosporin. Most first-generation cephalosporins begin with "ceph" and newer first-generation and all the later cephalosporins begin with "cef." Question: The half life of trimethoprim-sulfamethoxazole (Bactrim DS) is approximately: 4 hours. 6 hours. 10 hours. 12 hours. Explanation: Peak blood levels for the individual components occur 1 to 4 hours after oral administration. The mean serum half-lives of sulfamethoxazole and trimethoprim are 10 and 8 to 10 hours, respectively. During administration of 800 mg sulfamethoxazole and 160 mg trimethoprim BID, the mean steady-state plasma concentration of trimethoprim was 1.72 µg/mL. The steady-state mean plasma levels of free and total sulfamethoxazole were 57.4 µg/mL and 68.0 µg/mL, respectively. These steady-state levels were achieved after 3 days of drug administration. Question: Zinc oxide is indicated in the treatment of: dermatophytosis. diaper dermatitis. animal bites. puncture wounds. Explanation: Zinc oxide is a skin barrier indicated in the treatment of diaper dermatitis. It is a mild astringent with weak antiseptic properties. Skin barriers form a barrier to protect the skin from irritants and moisture. It may also be used in other minor skin irritations such as burns, cuts, and scrapes. Question: A treatment regimen for acne will only be considered ineffective after consistent adherence for at least: 2 weeks. 4 weeks. 6 weeks. 8 weeks. Correct Explanation: At least 2 to 3 months of consistent adherence to a therapeutic regimen is necessary prior to determining ineffectiveness and choosing a new treatment plan. Question: Severe nodular acne should be treated with: oral isotretinoin monotherapy. Correct topical retinoid and topical benzoyl peroxide. topical retinoid and oral isotretinoin. a topical retinoid, benzoyl peroxide and a topical antibiotic. Explanation: Treatment of severe nodular acne includes a topical retinoid plus an oral antibiotic plus topical benzoyl peroxide. Another option is oral isotretinoin as monotherapy. Question: Patients receiving imiquimod (Aldara) should not receive: fluoroquinolones. live vaccines. Correct oral steroids. tetracyclines. Explanation: Immunosuppressants may enhance the adverse/toxic effect of live vaccines and may diminish their therapeutic effect. Avoid use of live organism vaccines with immunosuppressants; live- attenuated vaccines should not be given for at least 3 months after immunosuppressants. Question: Zinc oxide, for the treatment of diaper dermatitis, is classified as a(n): antimicrobial. antifungal. bacteriostatic agent. skin barrier. Correct Explanation: Zinc oxide, used in the treatment of diaper dermatitis, is classified as a skin barrier. Skin barriers form a barrier to protect the skin from irritants and moisture. It is a mild astringent with weak antiseptic properties. It may also be used in other minor skin irritations such as burns, cuts, and scrapes. Question: Instructions given to patients being treated with Silver sulfadiazine (Silvadene) cream should NOT include: apply with sterile gloves. cover with a dressing after applying the cream. apply immediately after debridement. apply to the face. Correct Explanation: Silver sulfadiazine (Silvadene) should be NOT be applied to the face. It should be applied to burn wounds under sterile conditions, after the wound is cleansed and debrided. The burn areas should be covered with silver sulfadiazine (Silvadene) cream 1% at all times. The cream should be applied once to twice daily to a thickness of approximately 1/16 inch. Whenever necessary, the cream should be reapplied to any areas where patient activity has rubbed it off. Administration may be accomplished in minimal time because dressings are not required. However, if individual patient requirements make dressings necessary, they may be used. Question: A patient with psoriasis has a salicylic acid sensitivity and should be instructed to avoid: soy milk. bananas. almonds. Correct white potatoes. Explanation: Foods that are high in salicylates include almonds. There is a very long list of foods that contain high levels of salicylates and patients with a salicylate sensitivity, should read labels and avoid those foods with a high content. The other choices contain a negligible amount and should be safe to consume for the salicylic-sensitive patient. Question: The initial recommended therapy for patients with moderate postherpetic neuralgia is: capsaicin cream (Capsagel). gabapentin (Neurontin). Correct hydrocodone and acetaminophen (Norco). diphenhydramine (Dermarest). Explanation: Gabapentin (Neurontin) or pregabalin (Lyrica) is recommended for patients with moderate to severe postherpetic neuralgia (PHN). Tricyclic antidepressants (TCAs) are an off-label treatment for postherpetic neuralgia and neuropathic pain. TCAs are poorly tolerated in older adults. Topical capsaicin (Capsagel, Salon Pas Patches) is recommended for patients with mild to moderate localized pain from PHN who do not desire systemic therapy with tricyclic drugs, gabapentin, and pregabalin. However, topical capsaicin is often poorly tolerated. Topical lidocaine is an alternative that may provide short-term relief. Opioids are associated with the potential for abuse and addiction, and thus many experts consider them as second- or third-line treatment options for PHN. Question: Capsaicin topical cream, used to relieve pain related to herpes zoster,: is used to debride open wounds and blisters. may cause extreme irritation to eyes and mucous membranes. Correct should be used with a heating pad. is derived from banana peppers. Explanation: Capsaicin topical cream is an over the counter preparation for the relief of pain associated with arthritis, herpes zoster, back/muscle strain, and bruises. It is made of chili peppers and contact with eyes and mucous membranes should be avoided as it will cause extreme irritation to those areas. Wearing gloves during application or very good handwashing is recommended. It should not be applied to wounds, damaged, broken or irritated skin. Question: The steps to correctly apply topical permethrin (Nix) in the treatment of pediculosis capitis is to: 1. Apply to dry hair, devoid of conditioner. 2. Leave in place for 10 minutes. 3. Rinse with warm water over the sink. 4. Repeat treatment 7 days later if needed. Correct 1. Apply to wet hair. 2. Leave in place for 30 minutes. 3. Rinse with warm water over the sink. 4. Repeat treatment 3 days later if needed. 1. Apply to wet hair that has been conditioned. 2. Leave in place for 15 minutes. 3. Rinse with warm water in the shower. 4. Repeat treatment 7 days later if needed. 1. Apply to dry hair sparingly. 2. Leave in place for 30 minutes. 3. Rinse with warm water in the shower. 4. Repeat treatment 14 days later if needed. Explanation: Topical pediculicides should be applied according to the package instructions. Basic principles for treatment include: hair conditioners should not be used prior to application; these products may result in reduced efficacy. Rinsing of topical pediculicides should be performed over a sink rather than in a shower or bath to limit skin exposure; rinsing with warm water is preferred over hot water to minimize vasodilation and systemic absorption. Topical pediculicides should be applied to dry hair and hair should be saturated. The pediculicide remains on the hair for 10 minutes before rinsing off. A second treatment is indicated in 7 days if there is evidence of lice activity. Combing is performed with a fine-toothed comb; the hair should be wet, with an added lubricant such as hair conditioner. Question: When administering cephalexin (Keflex) suspension, sometimes used in the treatment of acne vulgaris,: administer the suspension with food. administer it at bedtime. refrigerate the suspension. Correct leave the suspension at room temperature. Explanation: After mixing cephalexin (Keflex), it should be refrigerated for up to 14 days. It is not administered with regard to food and can be administered any time throughout the day. Question: The mechanism of action of oral antifungal agents, used in the treatment of tinea corporis, is to: block synthesis of folic acid by bacteria and inhibit replication. uncouple mitochondrial oxidative metabolism and inhibit cell growth. Correct block the dissociation of peptidyl tRNA from ribosomes. inhibit protein synthesis by preventing ribosomal translocation. Explanation: Sulfa agents block synthesis of folic acid by bacteria and thus inhibit bacterial replication. First- generation cephalosporins inhibit cell wall synthesis of bacteria. Antifungals uncouple mitochondrial oxidative metabolism and inhibit cell growth. Macrolides inhibit bacterial growth, possibly by blocking dissociation of peptidyl tRNA from ribosomes, causing RNA-dependent protein synthesis to arrest. Other antibacterials are bacteriostatic or bactericidal and inhibit protein synthesis by preventing ribosomal translocation. Question: Oral antibiotics for the treatment of acne vulgaris: should not be used as monotherapy. Correct must be tapered slowly to discontinue. are indicated as initial treatment. are used as maintenance therapy. Explanation: Oral antibiotics for the treatment of acne vulgaris should not be used as monotherapy or maintenance therapy. Oral antibiotics should only be used when absolutely necessary when other therapies have not been successful. No consensus exists regarding whether oral antibiotics should be tapered or abruptly stopped. Question: The best choice for the relief of painful oral lesions associated with hand foot and mouth disease in children is: topical lidocaine. topical anesthetics. diphenhydramine suspension and Maalox mixed. oral acetaminophen. Correct Explanation: Pain and fever related to hand, foot and mouth disease are generally short lived and should be managed with ibuprofen or acetaminophen in children who are not dehydrated. Topical oral therapies containing lidocaine or other topical therapies (e.g., diphenhydramine, Kaolin pectin) to coat oral lesions and/or soothe pain in children are not usually recommended due to lack of evidence of benefit, potential for harm (e.g., toxicity from systemic absorption, allergic reaction) and difficulty of application in young children. Patients may suck on ice or popsicles, eat ice cream or sherbet, drink cold beverages, avoid citrus fruits, fruit drinks, and soda, and avoid spicy or salty foods. Children who are capable of gargling may do so with warm salt water, which may help with oral discomfort. Question: Imiquimod (Aldara) is classified as a topical: anti-inflammatory. antibiotic. antineoplastic. Correct steroid. Explanation: Imiquimod (Aldara) is classified as a topical antineoplastic. It is used in the treatment of actinic keratosis, superficial basal cell carcinoma, and genital warts. Question: Pimecrolimus (Elidel) is classified as a topical: antineoplastic. calcineurin inhibitor. Correct corticosteroid. keratolytic. Explanation: Pimecrolimus (Elidel) is classified as a topical calcineurin inhibitor. It is a dermatologic agent used in the treatment of atopic dermatitis. The exact mechanism of action is unknown, but there is inhibition of T-lymphocyte activation. Question: Gabapentin (Neurontin), indicated in the treatment of postherpetic neuralgia,: is highly protein bound. has dose proportional bioavailability. is metabolized into a prodrug. is excreted unchanged in the urine. Correct Explanation: Gabapentin (Neurontin) is eliminated from systemic circulation by renal excretion as unchanged drug. It is not appreciably metabolized in humans. Gabapentin bioavailability is not dose proportional (i.e., as dose is increased, bioavailability decreases). Less than 3% of gabapentin circulates bound to plasma protein. Gabapentin elimination half-life is 5 to 7 hours and is unaltered by dose or following multiple dosing. Gabapentin's elimination rate is constant; plasma clearance and renal clearance are directly proportional to creatinine clearance. Adjustment of the dose amount and frequency should be considered if creatinine clearance is decreased. Question: The Fingertip Unit (FTU) method is used when prescribing topical medications. If one arm equals 3 fingertips, approximately how many grams will need to be prescribed for a man who needs BID application to one arm for 7 days? 15 grams 21 grams Correct 30 grams 60 grams Explanation: A Fingertip Unit (FTU) is measured from the very tip of the finger to the first crease (DIP joint) in the finger. Each FTU is approximately equivalent to 0.5 and 0.4 grams of ointment in men and women, respectively. An estimate of the number of FTUs required to cover various areas of the body is as follows: head and neck = 4.5; trunk (front or back) = 7; one arm = 3; one hand = 1; one leg = 6; and one foot = 2. Therefore, one application to one arm would be 3 x 0.5 gms x 2 (twice daily), then x 7 days = 21 grams. Question: To enhance absorption, tetracycline should be administered: with milk. on an empty stomach. Correct with food. with an antacid. Explanation: Administer on an empty stomach (i.e., 1 hour prior to, or 2 hours after, meals) to increase total absorption and with adequate amount of fluid to reduce risk of esophageal irritation and ulceration. Administer at least 1 to 2 hours prior to, or 4 hours after, antacid because aluminum and magnesium cations may chelate with tetracycline and reduce its total absorption. Question: Pimecrolimus (Elidel) is indicated in the treatment of: actinic keratosis. acne vulgaris. atopic dermatitis. Correct psoriasis. Explanation: Pimecrolimus (Elidel) is classified as a topical calcineurin inhibitor. It is a dermatologic agent used in the treatment of atopic dermatitis. The exact mechanism of action is unknown, but there is inhibition of T-lymphocyte activation. Question: The generic name for Mycostatin is: atorvastatin. fluvastatin. nystatin. Correct pravastatin. Explanation: The generic name for Mycostatin is nystatin. It is a topical antifungal agent and is often confused with HMG-CoA reductase inhibitors, also known as "statins." Atorvastatin (Lipitor), fluvastatin (Lescol), and pravastatin (Pravachol) are classified as HMG-CoA reductase inhibitors for the treatment of hyperlipidemia. [Show More]
Last updated: 1 year ago
Preview 1 out of 38 pages
Reviews( 0 )
Document information
Connected school, study & course
About the document
Uploaded On
May 15, 2021
Number of pages
38
Written in

Additional information
This document has been written for:
Uploaded
May 15, 2021
Downloads
0
Views
60

.png)

 _ Dermatology Prescription (100 Questions and Answers) – South University Savannah.png)