Pharmacology > ATI > ATI Pharmacology IMPORTANT LAB VALUES (All)
ATI Pharmacology IMPORTANT LAB VALUES
Document Content and Description Below
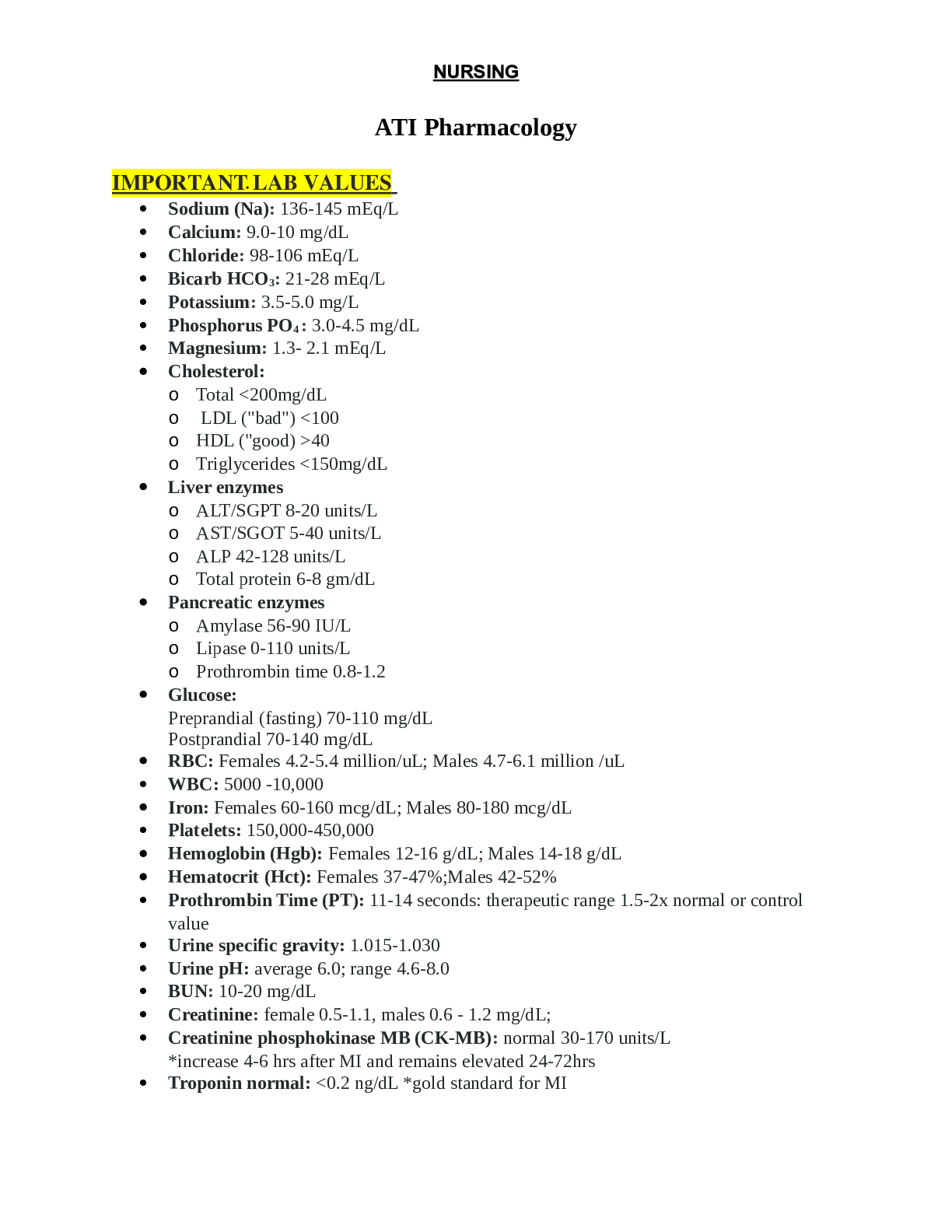
ATI Pharmacology IMPORTANT LAB VALUES ATI Pharmacology IMPORTANT LAB VALUES Sodium (Na): 136-145 mEq/L Calcium: 9.0-10 mg/dL Chloride: 98-106 mEq/L Bicarb HCO3: 21-28 mEq/L P... otassium: 3.5-5.0 mg/L Phosphorus PO4 : 3.0-4.5 mg/dL Magnesium: 1.3- 2.1 mEq/L Cholesterol: o Total <200mg/dL o LDL ("bad") <100 o HDL ("good) >40 o Triglycerides <150mg/dL Liver enzymes o ALT/SGPT 8-20 units/L o AST/SGOT 5-40 units/L o ALP 42-128 units/L o Total protein 6-8 gm/dL Pancreatic enzymes o Amylase 56-90 IU/L o Lipase 0-110 units/L o Prothrombin time 0.8-1.2 Glucose: Preprandial (fasting) 70-110 mg/dL Postprandial 70-140 mg/dL RBC: Females 4.2-5.4 million/uL; Males 4.7-6.1 million /uL WBC: 5000 -10,000 Iron: Females 60-160 mcg/dL; Males 80-180 mcg/dL Platelets: 150,000-450,000 Hemoglobin (Hgb): Females 12-16 g/dL; Males 14-18 g/dL Hematocrit (Hct): Females 37-47%;Males 42-52% Prothrombin Time (PT): 11-14 seconds: therapeutic range 1.5-2x normal or control value Urine specific gravity: 1.015-1.030 Urine pH: average 6.0; range 4.6-8.0 BUN: 10-20 mg/dL Creatinine: female 0.5-1.1, males 0.6 - 1.2 mg/dL; Creatinine phosphokinase MB (CK-MB): normal 30-170 units/L *increase 4-6 hrs after MI and remains elevated 24-72hrs Troponin normal: <0.2 ng/dL *gold standard for MI- Safe Medication Administration and Error Reduction: Reviewing a Medication Administration Record (RN QSEN - Teamwork and Collaboration, Active Learning Template - Nursing Skill, RM Pharm RN 7.0 Ch. 2) 1) Report all errors, and implement corrective measures immediately 2) Complete an incident report within the time frame the facility specifies, usually 24 hr. 3) Do not reference or include this report in the client's medical record 4) Evaluate clients' responses to medications, and document and report them. 5) Identify side and adverse effects, and document and report them. Chapter 12 - Substance Use Disorders: Therapeutic effect of chlordiazepoxide (Ch. 12 pg.85) - Substance Use Disorders: Smoking cessation using bupropion (Ch. 12 pg. 87) - Substance Use Disorders: Treatment for Cocaine Toxicity (Active Learning Template - System Disorder, RM Pharm RN 7.0 Ch. 12) 1) First line treatment = Benzodiazepines (to reduce CNS & cardiovascular effects) 2) Chlordiazepoxide, diazepam, lorazepam, clorazepate, oxazepam 3) Provide seizure precautions 4) Manifestations include nausea; vomiting; tremors; restlessness and inability to sleep; depressed mood or irritability; increased heart rate, blood pressure, respiratory rate, and temperature; diaphoresis; and tonic‑clonic seizures. Illusions are also common 5) Monitor vitals and neurological status on a regular basis Chapter 13 - Chronic Neurologic Disorders: Adverse effects of neostigmine (Ch. 13 pg. 91) Adverse effects: Excessive muscarinic stimulation Cholinergic crisis - Chronic Neurologic Disorders: Medications that interact with Carbamazepine (Ch. 13 pg. 99) - Carbamazepine causes a decrease in the effects of oral contraceptives and warfarin due to stimulation of hepatic medication-metabolizing enzymes. - Grapefruit juice inhibits metabolism, and thus increases carbamazepine levels. - Phenytoin and phenobarbital decrease effects of carbamazepine. - Chronic Neurologic Disorders: Adverse Effects of Phenytoin (RN QSEN - Safety, Active Learning Template - Medication, RM Pharm RN 7.0 Ch. 13) 1) CNS effects: Nystagmus, sedation, ataxia, double vision, cognitive impairment 2) Gingival hyperplasia: Softening and overgrowth of gum tissue, tenderness, and bleeding gums (consider folic acid supplement) 3) Skin rash (stop medication if rash appears) 4) Cardiovascular effects: dysrhythmias, hypotension (administer slow; 50 mg/min and in dilute solution) 5) Endocrine and other effects: Coarsening of facial features, hirsutism, and interference with vitamin D metabolism (consume enough Vitamin D)6) Interference with vitamin K‑dependent clotting factors causing bleeding in newborns. - Miscellaneous Central Nervous System Medications: Treating Malignant Hyperthermia (Active Learning Template - Medication, RM Pharm RN 7.0 Ch. 15) 1) Depolarizing neuromuscular blockers: Succinylcholine 2) Manifestations include muscle rigidity accompanied by increased temperature, as high as 43°C (109.4°) 3) Administer oxygen at 100%. 4) Initiate cooling measures including administration of iced 0.9% sodium chloride, applying a cooling blanket, and placing ice bags in groin and other areas 5) Administer dantrolene to decrease metabolic activity of skeletal muscle. - Airflow Disorders: Therapeutic Action of Montelukast (Active Learning Template - Medication, RM Pharm RN 7.0 Ch. 17) 1) Leukotriene modifiers: suppress the effects of leukotrienes, thereby reducing inflammation, bronchoconstriction, airway edema, and mucus production. 2) Long‑term therapy of asthma in adults and children, and to prevent exercise‑induced bronchospasm 3) Depending on therapeutic intent, effectiveness is evidenced by long‑term control of asthma 4) Advise clients to take montelukast once daily at bedtime. 5) For exercise‑induced bronchospasm, take 2 hr. before exercise. Instruct clients taking daily montelukast to not take an additional dose for exercise induced bronchospasm - Upper Respiratory Disorders: Client Teaching Prior to Allergy Testing (Active Learning Template - Medication, RM Pharm RN 7.0 Ch. 18) 1) Medications that can interfere with skin tests include: antihistamines, Tricyclic antidepressants, heartburn medications, asthma medication omalizumab (Xolair) 2) May need to discontinue certain meds 10 days prior 3) If you are running a fever or have an attack of hay fever or asthma, testing should be delayed 4) Do not change your diet before the test. - Medications Affecting Blood Pressure: Titrating Continuous Nitroprusside Infusion (RN QSEN - Safety, Active Learning Template - Medication, RM Pharm RN 7.0 Ch. 20) 1) Nitroprusside (centrally-acting vasodilator) 2) Direct vasodilation of arteries and veins resulting in rapid reduction of blood pressure (decreased preload and after load 3) Used for hypertensive crisis 4) Administer medication slowly because rapid administration will cause blood pressure to go down to rapidly 5) Prepare medication by adding to diluent for IV infusion.6) Protect IV container and tubing from light & Discard medication after 24 hr. Angina Chapter 22 (pg. 169) Self-administration of nitroglycerine patch (pg. 170) Client teaching for a new prescription of sublingual nitroglycerin PROTOTYPE: Nitroglycerin (NTG) Oral extended-release capsules Sublingual tablet Translingual spray Topical ointment Transdermal patch Intravenous Isosorbide dinitrate (Sublingual) Isosorbide mononitrate (PO) Adverse Effects: Headache: - Instruct clients to use aspirin or acetaminophen to relieve pain - Clients should notify the provider if headache does not resolve in a few weeks. Dosage can be reduced. Orthostatic hypotension: - Advise clients to sit or lie down if experiencing dizziness or faintness. - Clients should avoid sudden changes of position/rise slowly. Reflex Tachycardia: - Monitor vitals. - Administer a beta-blocker such as metoprolol if needed. Tolerance: - Use lowest dose needed to achieve effect. - Take all long-acting forms of nitroglycerin with a medication-free period each day. This action reduces the risk of tolerance. Contraindications/ Precautions: - Pregnancy Risk Category C. - This medication is contraindicated in clients who have hypersensitivity to nitrates. - Nitroglycerin is contraindicated in clients who have severe anemia, closed-angle glaucoma and traumatic head injury because the medication can increase intracranial pressure. - Use cautiously in clients taking antihypertensive medications and clients who have hyperthyroidism or renal or liver dysfunction. Nursing evaluation of medication effectiveness: - Prevention and termination of acute anginal attacks - Long-term management of stable angina. - Control of perioperative blood pressure. - Control of heart failure following acute MI.- In chronic stable exertional angina, nitroglycerin dilates veins and decreases venous return (preload), which decreases cardiac oxygen demand. - Use this rapid‑acting nitrate at the first indication of chest pain. Do not wait until pain is severe. - Use prior to activity that is known to cause chest pain, such as climbing a flight of stairs. - Place the tablet under the tongue and allow it to dissolve - Store tablets in original bottles, and in a cool, dark place. - Medications Affecting Cardiac Rhythm: Ventricular Dysrhythmia (Active Learning Template - Medication, RM Pharm RN 7.0 Ch. 23) 1) Antidysrhythmic meds class IB (Lidocaine) 2) Decrease electrical conduction, Decrease automaticity, Increase rate of repolarization 3) Short‑term use only for ventricular dysrhythmias 4) Administer phenytoin to control seizure activity. 5) Use cautiously in clients who have liver and kidney dysfunction, second‑degree heart block, sinus bradycardia, and heart failure. Medications Affecting Coagulation (Chapter 25 page 191) Administering Heparin (pg. 193) Laboratory values to report to the provider Self- Administration of Enoxaparin (pg. 193) Adverse effects of clopidogrel (pg. 197) Monitoring for adverse effects of Warfarin Adverse effects of Heparin Medication safety with Warfarin (pg. 194) Reviewing client data during heparin infusion (pg. 192) PROTOTYPE: Heparin Low Molecular Weight: PROTOTYPE: Enoxaparin Other: Dalteparin Activated factor (Xa) Inhibitors: PROTOTYPE Medication: Fondaparinux Adverse Effects: Hemorrhage secondary to heparin overdose: - Monitor vital signs. - Advise clients to observe for bleeding (increase heart rate, decreased blood pressure, bruising, petechiae, hematomas, black tarry stools). - In the case of overdose, stop heparin, administer protamine, and avoid aspirin. - Monitor activated partial thromboplastin time (aPTT). Keep value at 1.5 to 2 times the baseline. Heparin induced thrombocytopenia Interventions: - Evidenced by low platelet count and increased development of thrombi: mediated by antibody development (white clot syndrome) - Monitor platelet count periodically throughout treatment, especially in the first month.- Stop heparin if platelet count is less than 100,000/mm^3; Nonheparin anticoagulants, such as lepirudin or argatroban, can be used as a substitute if anticoagulation is still needed. Hypersensitivity reaction (chills, fever urticaria): - Administer a small test dose prior to the administration of heparin. Toxicity/overdose: - Administer protamine, which binds with heparin-protamine complex that has no anticoagulant properties. - Protamine should be administered slowly IV, no faster than 20mg/min or 50mg in 10 min. - Do not exceed 100 mg in a 2-hr period. Administer carefully to prevent overdose (anticoagulation). Enoxaparin: Hemorrhage: - Monitor vital sings - Advise clients to observe for bleeding (increased heart rate, decreased blood pressure, bruising, petechiae, hematomas, black tarry stools) - Monitor platelet count. Instruct clients to avoid aspirin. Neurologic damage from hematoma formed during spinal or epidural anesthesia: - In clients who have spinal or epidural anesthesia: Assess insertion site for sings of hematoma formation, such as redness or swelling; Monitor sensation and movement of lower extremities; Notify provider of abnormal findings. Thrombocytopenia Interventions: - Monitor platelets. Discontinue medication for platelet count less than 100,000/mm^3. Toxicity/ Overdose - Administer protamine (heparin antagonist) - Protamine should be administered slowly intravenously, no faster than 20 mg/min or 50 mg in 10 min. Fondaparinux: -Hemorrhage -Neurologic damage from hematoma formed during spinal or epidural anesthesia. -Thrombocytopenia, as evidenced by low platelet count. Contraindications/Precautions: -Parenteral anticoagulants are contraindicated in clients who have low platelet counts (thrombocytopenia) or uncontrollable bleeding. -These medications should not be used during or following surgeries of the eyes, brain, or spinal cord; lumbar puncture; or regional anesthesia. -Use cautiously in clients who have hemophilia, increased capillary permeability, dissecting aneurysm, peptic ulcer disease, severe hypertension, hepatic or renal disease, or threatened abortion.Interactions: - Antiplatelet agents such as aspirin, NSAIDs, and other anticoagulants can increase the risk for bleeding. -Avoid concurrent use when possible -Monitor carefully for evidence of bleeding -Take precautionary measures to avoid injury (limit venipuncture and injections). Nursing Evaluation of Medication Effectiveness: - Heparin: aPTT levels of 60 to 80 seconds. - Heparin, enoxaparin, and fondaparinux sodium: No development or no further development of venous thrombi or emboli. Oral Anticoagulants PROTOTYPE: Warfarin Adverse Effects: Hemorrhage - Monitor VS. - Advise clients to observe for bleeding (increased heart rate, decreased blood pressure, bruising, petechiae, hematomas, black tarry stools). - Obtain baseline PT, and monitor PT levels of PT and INR periodically. - In the case of a warfarin overdose, discontinue administration of warfarin, and administer vitamin K. Hepatitis: - Monitor liver enzymes. Toxicity/ Overdose: - Administer Vitamin K, to promote synthesis of coagulation factors VII, IX, X, and prothrombin. - Administer IV vitamin K, slowly and in a diluted solution to prevent anaphylactoid-type reaction. - Administer small doses of vitamin K to prevent development of resistance to warfarin. - If Vitamin K, cannot control bleeding, administer fresh plasma or whole blood. Contraindications/ Precautions: - Classified as Pregnancy Risk Category X due to high risk of fetal hemorrhage, fetal death, and CNS defects. Advise clients to notify the provider if they become pregnant during warfarin therapy. If anticoagulation is needed during pregnancy, heparin can be safely used. - Contraindicated in clients who have low platelet counts (thrombocytopenia) or uncontrollable bleeding. - Contraindicated during or following surgeries of the eye(s), brain, or spinal cord; lumbar puncture; or regional anesthesia. - Contraindicated in clients who have vitamin K deficiencies, liver disorders, and alcohol use disorder due to the additive risk of bleeding.- Use cautiously in clients who have hemophilia, dissecting aneurysm, peptic ulcer disease, severe hypertension, or threatened abortion. Interactions: Concurrent use of heparin, aspirin, acetaminophen, glucocorticoids, sulfonamides, and parenteral cephalosporins increases effects of warfarin, which increases the risk for bleeding. - Avoid concurrent use if possible. - Instruct clients to observe for inclusion of aspirin in OTC medications. - If used concurrently, monitor carefully for indications of bleeding and increased PT, INR, and aPTT levels. - Medication dosage should be adjusted accordingly. Concurrent use of phenobarbital, carbamazepine, phenytoin, oral contraceptives, and vitamin K decreases anticoagulant effects. - Avoid concurrent use if possible. - If used concurrently, monitor carefully for reduced PT and INR levels. - Medication dosage should be adjusted accordingly. Foods high in vitamin K, such as dark green leafy vegetables (lettuce, cooked spinach), cabbage, broccoli, Brussels sprouts, mayonnaise, and canola and soybean oil, can decrease anticoagulant effects with excessive intake. - Provide clients with a list of foods high in vitamin K. - Instruct clients to maintain a consistent intake of vitamin K to avoid sudden fluctuations that could affect the action of warfarin. Multiple other medications interact with warfarin. - Take a complete medication history for clients taking warfarin, and advise clients to inform the provider if any new medication is started. Nursing Administer: Depending on therapeutic intent, effectiveness can be evidenced by the following. - PT 1.5 to 2 times control. - INR of 2 to 3 for treatment of acute myocardial infarction, atrial fibrillation, pulmonary embolism, venous thrombosis, or tissue heart valves. - INR of 3 to 4.5 for mechanical heart valve or recurrent systemic embolism. - No development or no further development of venous thrombi. Laboratory Values: - Prothrombin time (PT): 11-14 seconds - Partial thromboplastin time (PTT): 25-35 seconds - International normalized ratio (INR): 0.8 to 1.2 - Hct: M: 41-53% & F: 36-46% - Hgb: M: 13.5-17.5 g/dL & F: 12.0-16.0 g/dL Adverse effects of Clopidogrel: Bleeding: Prolonged bleeding time, gastric bleed, thrombocytopenia. -Monitor bleeding time.-Monitor for gastric bleed (coffee‑ground emesis or bloody, tarry stools). -Monitor for bruising, petechial, and bleeding gums. -Apply pressure to cardiac catheter access. GI effects (diarrhea, dyspepsia, pain): - Teach client to monitor for effects and notify the provider. Growth factors (chapter 26 pg. 201) Evaluating Client response Monitoring adverse effects of Epoetin alfa Effectiveness of oprelvekin therapy PROTOTYPE: Epoetin Alfa, erythropoietin Other: Darbepoetin alfa, long acting erythropoietin Adverse effects: Hypertension: Secondary to elevation in hematocrit level. - Monitor Hgb levels and blood pressure. If elevated administer antihypertensive medications. Risk for a thrombic event: Such as myocardial infraction or stroke if the client has a Hgb of 11/g/dL or higher, or an increase of more than 1g/dL in 2 weeks. Seizures can also occur with a too-rapid rise in the blood counts. - Decrease dosage when these limits are reached. Therapy can be resumed when Hgb drops to acceptable level, but dosage should be produced. - Consider placing client on seizure precautions if rapid increase in Hgb or blood pressure occurs. Deep-vein thrombosis: Increased risk in preoperative care. - Prophylactic use of an anticoagulant might be needed for preoperative clients. Headache and body aches: - Report headaches that are frequent or severe to the provider. Hypertension can be the cause. Contraindications/ Precautions: - Pregnancy Risk Category C. - Contraindicated in clients who have uncontrolled hypertension. - Contraindicated in clients who have some cancers due to possible increase in tumor growth. Nursing evaluation of medication effectiveness:- Depending on therapeutic intent, effectiveness can be evidenced by Hgb level of 10 to 11 g/dL and maximum Hct of 33% - Erythropoietic growth factors: Depending on therapeutic intent, effectiveness can be evidenced by Hgb level of 10 to 11 g/dL and maximum Hct of 33% - Leukopoietic growth factors: effectiveness can be evidenced by the following: Absence of infection & WBC count and differential within expected reference range - Thrombopoietic growth factors: Depending on therapeutic intent, effectiveness can be evidenced by platelet count greater than 50,000/mm3. - Granulocyte‑macrophage colony‑stimulating factor: effectiveness can be evidenced by the following: Absence of infection & WBC and differential within expected reference ranges. Oprelvekin Nursing evaluation of medication effectiveness: - Depending on therapeutic intent, effectiveness can be evidenced by platelet count greater than 50,000/mm3. Peptic Ulcer Disease (Chapter 28 pg. 215) Antacid therapy: Patient-centered care Client teaching about sucralfate (pg. 216) Teaching about Ranitidine Histamine 2-receptor antagonists: PROTOTYPE: Ranitidine (-ine) Other Medications: -Cimetidine -Famotidine -Nizatidine: PO use only Cimetidine Adverse Effects: Blocked androgen receptors - Resulting in decreased libido, gynecomastia, and impotence. - Inform clients of these possible effects. CNS Effects (lethargy, depression, confusion): - These effects are seen more often in older adults who have kidney or liver dysfunction. - Cimetidine should be avoided in older adults. Ranitidine Adverse Effects: Constipation, diarrhea, nausea - Report these effects to the provider.Famotidine Adverse Effects: Dizziness, drowsiness, constipation - Avoid tasks that require alertness, and take medication at bedtime. Contraindications/ Precautions: - These medications are Pregnancy Risk Category B. - Use in older adults can cause antiadrenergic effects (impotence) and CNS effects (confusion). - H 2-receptor antagonists decrease gastric acidity, which promotes bacterial colonization of the stomach and the respiratory tract. Use cautiously in clients who are at risk for pneumonia, including clients who have chronic obstructive pulmonary disease (COPD). Interactions: Cimetidine can inhibit medication-metabolizing enzymes and thus increase the levels of warfarin, phenytoin, theophylline, and lidocaine. - In clients taking warfarin, monitor indications for bleeding. - Monitor INR & PT levels, and adjust warfarin dosages accordingly. - In clients taking phenytoin, theophylline, and lidocaine, monitor serum levels and adjust dosages accordingly. Concurrent use of antacids can decrease absorption of histamine2-receptor antagonists. - Advise clients not to take an antacid 1 hour before or after taking a histamine2-receptor antagonist. Proton pump inhibitor: (-prazole) PROTOTYPE: Omeprazole Other medications: -Pantoprazole -Lansoprazole -Dexlansoprazole -Rabeprazole -Esomeprazole Adverse effects: Minor adverse effects with short-term treatment include headache, diarrhea, nausea, and vomiting. Long- term treatment: Pneumonia - Inform clients of these possible effects and to monitor and report manifestations of a respiratory infection. Osteoporosis and fractures - Advise clients to increase vitamin D and calcium intake. Rebound acid hypersecretion - Advise clients to take low dose if possible and to taper slowly to discontinue.Hypomagnesemia - Advise clients to monitor and report manifestations of hypomagnesemia, such as tremors, muscle cramps, and seizures Contraindications/ Precautions: - These medications are Pregnancy Risk Category B, except for omeprazole, which is Category C. - Contraindicated for clients hypersensitive to medications and during lactation. - Use cautiously in children and with clients who have dysphagia or liver disease. - These medications increase the risk for pneumonia. Use cautiously in clients at high risk for pneumonia, including clients who have COPD. Interactions: Digoxin and phenytoin levels can increase when used concurrently with omeprazole. - Monitor digoxin and phenytoin levels carefully if prescribed concurrently. Absorption of ketoconazole, itraconzale, and antazanvavir is decreased when taken concurrently with protein pump inhibitors. - Avoid concurrent use. If necessary to administer concurrently, separate medication administration concurrently, separate medication by 2 to 12 hr. The beneficial effects of clopidogrel can decrease with concurrent use. - Monitor thrombotic events. Nursing administration: - Do not crush, chew, or break sustained-release capsules. - Do not open capsule and sprinkle contents over food to facilitate swallowing. - Clients should take omeprazole once per day prior to eating in the morning. - Encourage clients to avoid alcohol and irritating medications, such as NSAIDs. - Active ulcers should be treated for 4 to 6 weeks. - Pantoprazole can be administered to clients by IV. In addition to slow incidence of headache and diarrhea, there can be irritation at the injection site leading to thrombophlebitis. Monitor the - IV site for indications of inflammation (redness, swelling, local pain), and change the IV site indicated. - Teach clients to notify the provider for any indication of obvious or occult GI bleeding such as coffee-ground emesis. Mucosal Protectant: PROTOTYPE: Sucrasulfate Adverse effects: Constipation - To prevent constipation, encourage clients to increase dietary fiber and drink at least 1,500 mL/day if fluids are not restricted. Contraindications/ Precautions: -Pregnancy Risk Category B -Contraindicated in clients who are hypersensitive to the medication.-Use cautiously in clients who have kidney disease. Interactions: Sucralfate can interfere with the absorption of phenytoin, digoxin, warfarin, and ciprofloxacin. - Maintain a 2-hr interval between these medications and sucralfate to minimize interaction. Antacids interfere with the absorption of sucraflate. - Take sucralfate 30 min before or after antacids. Nursing administration: - Assist clients with the medication regimen. - Instruct clients that sucralfate should be taken four times a day, 1 hr. before meals, and again at bedtime. - Clients can break or dissolve the medication in water, but should not crush or chew the tablet. - Encourage clients to complete the course of treatment. Antacids: PROTOTYPE: Aluminum hydroxide Other: -Magnesium hydroxide -Calcium carbonate Adverse effects: Constipation, diarrhea - Aluminum and calcium compounds: constipation - Magnesium compounds: diarrhea - Advise clients that use of these compounds can be alternated to offset intestinal effects and normalize bowel function. - If a client has difficulty managing bowel function, recommend a combination product that contains aluminum hydroxide and magnesium hydroxide. Fluid retention - Antacids containing sodium can result in fluid retention. - Teach clients who have hypertension or heart failure to avoid antacids that contain sodium. Hypophosphatemia, hypomagnesemia - Possible effects of aluminum hydroxide. - Monitor electrolyte levels. Toxicity, hypermagnesemia - Magnesium compounds can lead to toxicity and hypermagnesemia in clients who have impaired kidney function. - Teach clients who have impaired kidney function to avoid antacids that contain magnesium. - Monitor for CNS depression. Contraindications/ Precautions:- Aluminum hydroxide is Pregnancy Risk Category C. - Antacids should be used with caution in clients who have GI perforation or obstruction. - Use cautiously in clients who have abdominal pain. Interactions: Aluminum compounds bind to phenytoin, and tetracycline interferes with absorption. - Teach clients to take these medications 4 to 6 hours apart. Nursing administration: - Clients taking tablets should be instructed to chew the tablets thoroughly and then drink at least 8 oz. of water or milk. - Teach clients to shake liquid formulations to ensure even dispersion of the medication. - Compliance is difficult for clients due to the frequency of administration. Medication can be administered seven times a day: 1 hr. and 3 hr. after meals, and again at bedtime. Encourage compliance by reinforcing the intended effect of the antacid (such as relief of pain, healing of ulcer). - Teach clients to take all medications at least 1 hr. before or after taking an antacid. - Opioid Agonist and Antagonists: Findings to Report to the Provider (RN QSEN - Safety, Active Learning Template - Medication, RM Pharm RN 7.0 Ch. 36) 1) Opioid agonists: Have naloxone and resuscitation equipment available 2) Opioid agonists complications: respiratory depression (stop if <12), constipation, orthostatic hypotension, urinary retention, cough suppression, sedation, biliary colic, N/V, overdose 3) Opioid antagonists: Naloxone 4) Antagonist complications: Tachycardia, tachypnea, abstinence syndrome (cramping, hypertension, vomiting, and reversal of analgesia) 5) Naloxone and naltrexone are contraindicated in clients who have opioid dependency. - Miscellaneous Pain Medications: Teaching About a Prescription for Antigout Medication (RN QSEN - Patient-centered Care, Active Learning Template - Medication, RM Pharm RN 7.0 Ch. 38) 1) proto: colchicine (Colcrys) 2) monitor uric acid levels, CBC, uric acid levels, urinalysis, liver and kidney function tests 3) allopurinol should be well-diluted and administered as an infusion over 30-60 min 4) avoid alcohol and food high in purine (red meat, scallops, cream sauces) 5) Prednisone is used for clients with acute gout who are unable to take or unresponsive to NSAIDS. - Miscellaneous Pain Medications: Adverse Effects of Ergotamine (RN QSEN – Safety, Active Learning Template - Medication, RM Pharm RN 7.0 Ch. 38) 1) GI upset (N/V); Administer an antiemetic, such as metoclopramide 2) Acute or chronic overdose (ergotism): Muscle pain, paresthesia in fingers and toes; peripheral ischemia3) Physical dependence 4) Fetal harm or abortion 5) Contraindicated in clients who have renal and/or liver dysfunction, sepsis, hypertension, history of myocardial infarction, and CAD, as well as during pregnancy & Pregnancy Risk Category X. - Diabetes Mellitus: Evaluating Understanding of Insulin Self-Administration (RN QSEN - Patient-centered Care, Active Learning Template - Medication, RM Pharm RN 7.0 Ch. 39) 1) When mixing short‑acting insulin with longer‑acting insulin, draw the short‑acting insulin up into the syringe first, then the longer‑acting insulin. This prevents the possibility of accidentally injecting some of the longer‑acting insulin into the shorter‑acting insulin vial. (This can pose a risk for unexpected insulin effects with subsequent uses of the vial. 2) NPH and premixed insulins should appear cloudy. Do not administer other insulins if they are cloudy or any insulins that are discolored or if a precipitate is present 3) Instruct clients to administer subcutaneous insulin in one general area to have consistent rates of absorption. 4) Vials of premixed insulins can be stored for up to 3months under refrigeration. 5) Store the vial that is in use at room temperature, avoiding proximity to sunlight and intense heat. Discard after 1 month. - Endocrine Disorders: Client Teaching About Antidiuretic Hormones (RN QSEN - Patient-centered Care, Active Learning Template - Medication, RM Pharm RN 7.0 Ch. 40) 1) Antidiuretic hormone (ADH), produced by the hypothalamus and stored in the posterior pituitary, promotes reabsorption of water within the kidney 2) In general, clients should reduce fluid intake during therapy 3) Monitor ECG and blood pressure. Advise clients to notify the provider of chest pain, tightness, or diaphoresis 4) Monitor vital signs, central venous pressure, I&O, specific gravity, and laboratory studies (potassium, sodium, BUN, creatinine, specific gravity, osmolality), BP & HR 5) Intranasal desmopressin starts with a bedtime dose. I&O is monitored. When nocturia is controlled, doses are given twice daily 6) Reduction in the large volumes of urine output associated with diabetes insipidus to normal levels of urine output. - Endocrine Disorders: Adverse Effects of Thyroid Hormone (Active Learning Template - Medication, RM Pharm RN 7.0 Ch. 40) 1) Overmedication can result in indications of hyperthyroidism (anxiety, tachycardia, palpitations, altered appetite, abdominal cramping, heat intolerance, fever, diaphoresis, weight loss, menstrual irregularities) 2) Chronic overtreatment can cause atrial fibrillation and an increased risk of fractures from bone loss, especially in older adults. 3) TSH levels should be monitored at least once a year4) Use cautiously in obese patients, older adults and those with cardiovascular problems (hypertension, angina pectoris, ischemic heart disease) because of cardiac stimulant effects. - Endocrine Disorders: Identifying a Need for a Dosage Increase of Levothyroxine (Active Learning Template - Medication, RM Pharm RN 7.0 Ch. 40) 1) Binding agents, antiulcer medications, calcium and iron supplements, and food reduce levothyroxine absorption with concurrent use (4 hours between) 2) Many antiseizure and antidepressant medications, including carbamazepine, phenytoin, phenobarbital, and sertraline, can increase levothyroxine metabolism (dosages may need to be increased) 3) Levothyroxine can increase the anticoagulant effects of warfarin by breaking down vitamin K (monitor INR & PT; report signs of bleeding; warfarin dosages may need to be decreased) 4) Daily therapy begins with a low dose that increases gradually over several weeks. Full effect of medication can take 6 to 8 week 5) Instruct clients to take the medication daily on an empty stomach 30 to 60 min before breakfast. - Immunizations: Contraindication for Receiving Varicella Vaccine (RN QSEN - Safety, Active Learning Template - Medication, RM Pharm RN 7.0 Ch. 41) 1) Administer one dose at 12 to 15 months and 4 to 6 years or two doses administered a minimum of 4weeks apart if administered after age 13 years. 2) Contraindicated: pregnancy & Anaphylactic reaction to gelatin or neomycin 3) Treatment with antiviral medication within 24 hr. prior to immunization (avoid taking antivirals for 14 days following immunization) 4) Extended use (2 weeks or longer) of corticosteroids or other medications that affect the immune system 5) Transfusion with blood product containing antibodies within the prior 11 /months. - Principles of Antimicrobial Therapy: Identifying Types of Infections (Active Learning Template - System Disorder, RM Pharm RN 7.0 Ch. 43) 1) Suprainfection is a type of resistance that results when an antibiotic kills normal flora, thus favoring the emergence of a new infection that is difficult to eliminate 2) changes in the DNA of micro‑organisms, called conjugation, which produces resistance to multiple existing medications, mandates the continual creation of new antimicrobials 3) Originating or taking place in a hospital, acquired in a hospital, especially in reference to an infection. Antibiotics affecting the Bacterial Cell wall. (Chapter 44 pg. 357) - Priority Finding After a Penicillin Injection - Plan of care for client administered antibiotics - Interventions for Uritcaria - Antibiotic interactions with cefazolin- Laboratory results to report - Caring for a client who has a penicillin allergy - Ceftazidime/PCN Cross-Sensitivity Penicillins: Narrow: (PROTOTYPE)Penicillin G benzathine (IM), Penicillin V (PO) Broad: Amoxicillin (PO), Amoxicillin-clavulanate (PO), Ampicillin (PO/IV) Antistaphylococcal: Nafcillin (IM) Antipseudomonal: Ticarcillin-clavulanate (IV), Piperacillin tazobactam (IV) Adverse effects: Allergies/ Anaphylaxis: - Interview clients for prior allergy. - Advise clients to wear an allergy identification bracelet. - Observe for allergic reactions for 30 min following parenteral administration of penicillin. Renal impairment - Monitor kidney function & I&O. Hyperkalemia, dysrhythmias (high doses of penicillin G potassium) Hypernatremia (IV ticarcillin-clavulante) - Monitor cardiac status and electrolyte levels. Contraindications/Precautions: - A history of severe allergic reactions to penicillins, cephalosporin, or imipenem is a contraindication for penicillins. - Use cautiously for clients who have or are at risk for kidney dysfunction (clients who are acutely ill, older adults, or young children). - Clients who are allergic to one penicillin are cross‑allergic to other penicillins and are at risk for cross‑sensitivity to cephalosporins. Interactions: - Penicillin in the same IV solution as aminoglycosides inactivates the aminoglycoside. Do not mix penicillin and aminoglycosides in the same IV solution. - Probenecid (treats Gout) delays the excretion of penicillin. Providers sometimes add probenecid to prolong the action of penicillin therapy. Nursing Administration: - Instruct clients to take penicillin V, amoxicillin, and amoxicillin‑clavulanate with meals. Tell them to take all others with 8 oz. of water 1 hr. before or 2 hr. after meals. - Instruct clients to report any signs of an allergic response such as dyspnea, a skin rash, itching, and hives. - Give IM injections cautiously to avoid injecting into a nerve or an artery. - Advise clients to complete the entire course of therapy, even if symptoms resolve. - Advise client to use an additional contraceptive method when taking penicillins.Cephalosporins: PROTOTYPE: Cephalexin, first generation First generation: Cefazolin (IM/IV) Second generation: Cefaclor, cefotetan (PO) Third generation: Ceftriaxone, cefotaxime (IM/IV) Fourth generation: Cefepime (IM/IV) Adverse effects: - Allergy, hypersensitivity, anaphylaxis, possible cross‑sensitivity to penicillin. - If indications of allergy appear (urticaria, rash, hypotension, dyspnea), stop the cephalosporin immediately, and notify the provider. - Question clients carefully about a history of allergy to a penicillin or another cephalosporin, and notify the provider if present. - Bleeding tendencies from cefotetan and ceftriaxone - Avoid use for clients who have bleeding disorders and for clients taking anticoagulants. - Observe clients for bleeding. - Monitor prothrombin and bleeding times. Delays in clotting can require discontinuation of the - medication. - Administer parenteral vitamin K. - Thrombophlebitis with IV infusion - Rotate injection sites. - Administer as a dilute intermittent infusion or slowly over 3 to 5 min and in a dilute solution for bolus dosing. - Renal Insufficiency - Giver lower dosage of most cephalosporin to prevent accumulation to toxic levels. - Pain with IM injection - Administer IM injections deep into a large muscle mass such as into the ventrogluteal site. - Antibiotic‑associated pseudomembranous colitis - Observe for diarrhea, and notify the provider if present. - Stop the medication. Contraindications/Precautions: - Do not give cephalosporins to clients who have a history of severe allergic reactions to penicillins. - Use cautiously with clients who have renal impairment or bleeding tendencies. Interactions: - Disulfiram reaction (intolerance to alcohol) occurs with simultaneous use of alcohol and either cefotetan or cefazolin. Instruct clients not to consume alcohol while taking these cephalosporins. - Probenecid (gout) delays renal excretion. Monitor I&O. Nursing Administration: - Instruct clients to complete the entire course of therapy, even if symptoms resolve. - Advise clients to take oral cephalosporins with food. - Instruct clients to store oral cephalosporin suspensions in a refrigerator.Carbapenems: PROTOTYPE: Imipenenem-cilastaton (IM/IV), Meropenem (IV) Adverse Effects: - Allergy, hypersensitivity, possible cross‑sensitivity to penicillin or cephalosporins - Monitor for indications of allergic reactions, such as dyspnea, rashes, and pruritus. - Question clients carefully about their history of allergy to a penicillin or other cephalosporin, and notify the provider if present. - Gastrointestinal upset (nausea, vomiting, diarrhea) - Observe for manifestations, and notify the provider if they occur. - Monitor I&O. - Suprainfection - Monitor for indications of colitis (diarrhea), oral thrush, and vaginal yeast infection. Contraindications/ Precautions: - Imipenem‑cilastatin is a Pregnancy Risk Category C medication. - Use cautiously in clients who have renal impairment. Interactions: - Imipenem‑cilastatin can reduce blood levels of valproic acid. Breakthrough seizures are possible. - Avoid using together. If concurrent use is unavoidable, monitor for increased seizure activity. Nursing Administration: - Advise client to complete the entire course of therapy, even if symptoms resolve. Other inhibitors of cell wall synthesis: - Vancomycin (PO/IV) - Aztreonam, a monobactam, (IM/IV) - Fosfomycin (PO) Adverse Effects: Ototoxicity (rare and reversible) - Assess for indications of hearing loss. - Instruct clients to notify the provider if changes in hearing acuity develop. - Monitor vancomycin levels. Infusion reactions - Monitor for red man syndrome: rashes, flushing, tachycardia, and hypotension.) - Administer vancomycin slowly over 60 min. IM and IV injection‑site pain, thrombophlebitis - Rotate injection sites. - Monitor the infusion site for redness, swelling, and inflammation. Renal toxicity- Monitor I&O and kidney function tests. - Monitor vancomycin trough levels. Contraindications/ Precautions: - An allergy to corn or corn products and previous allergy to vancomycin are contraindications. - Use cautiously for older adults and with clients who have renal impairment or hearing loss. Interactions: - Increased risk for ototoxicity when taking vancomycin concurrently with another medication that causes ototoxicity (loop diuretics, aminoglycoside antibiotics). - Assess for hearing loss. Nursing Administration: - Monitor vancomycin trough levels routinely after blood levels have reached a steady state. - For clients who have renal insufficiency, creatinine clearance levels indicate IV dosage adjustments. Nursing Evaluation of Medication Effectiveness: Indications of effectiveness include the following. - Reduction of manifestations such as fever, pain, inflammation, and adventitious breath sounds - Resolution of infection. - Antibiotics Affecting Protein Synthesis: Dietary Supplement Interactions with Tetracycline (Active Learning Template - Medication, RM Pharm RN 7.0 Ch. 45) 1) Instruct clients to take tetracyclines (except for minocycline) on an empty stomach with 8 oz. water. It may be taken with food if gastric distress occurs. 2) Interaction with milk products, calcium and iron supplements, laxatives containing magnesium, and antacids causes formation of nonabsorbable chelates, thus reducing the absorption of tetracyclines. 3) Tell clients not to take tetracyclines just before lying down because it increases the risk of esophageal ulceration. 4) Instruct clients to maintain a 2‑hr interval between ingestion of chelating agents and tetracyclines. 5) Avoid milk products and antacids, or separate by 2 hr. - Urinary Tract Infections: Evaluating Client Response to an Analgesic (Active Learning Template - Medication, RM Pharm RN 7.0 Ch. 46) 1) Urinary tract analgesic (Phenazopyridine) 2) The medication is an azo dye that functions as a local anesthetic on the mucosa of the urinary tract 3) Relieves manifestations of burning with urination, pain, frequency, and urgency 4) Acute kidney injury and chronic kidney disease are contraindications 5) It changes urine to an orange‑red color (can stain clothing) [Show More]
Last updated: 1 year ago
Preview 1 out of 20 pages
Instant download
Buy this document to get the full access instantly
Instant Download Access after purchase
Add to cartInstant download
Reviews( 0 )
Document information
Connected school, study & course
About the document
Uploaded On
Oct 08, 2021
Number of pages
20
Written in

Additional information
This document has been written for:
Uploaded
Oct 08, 2021
Downloads
0
Views
74