Sullivan University BIO-2020 103 NCLEX-study guide.
Document Content and Description Below
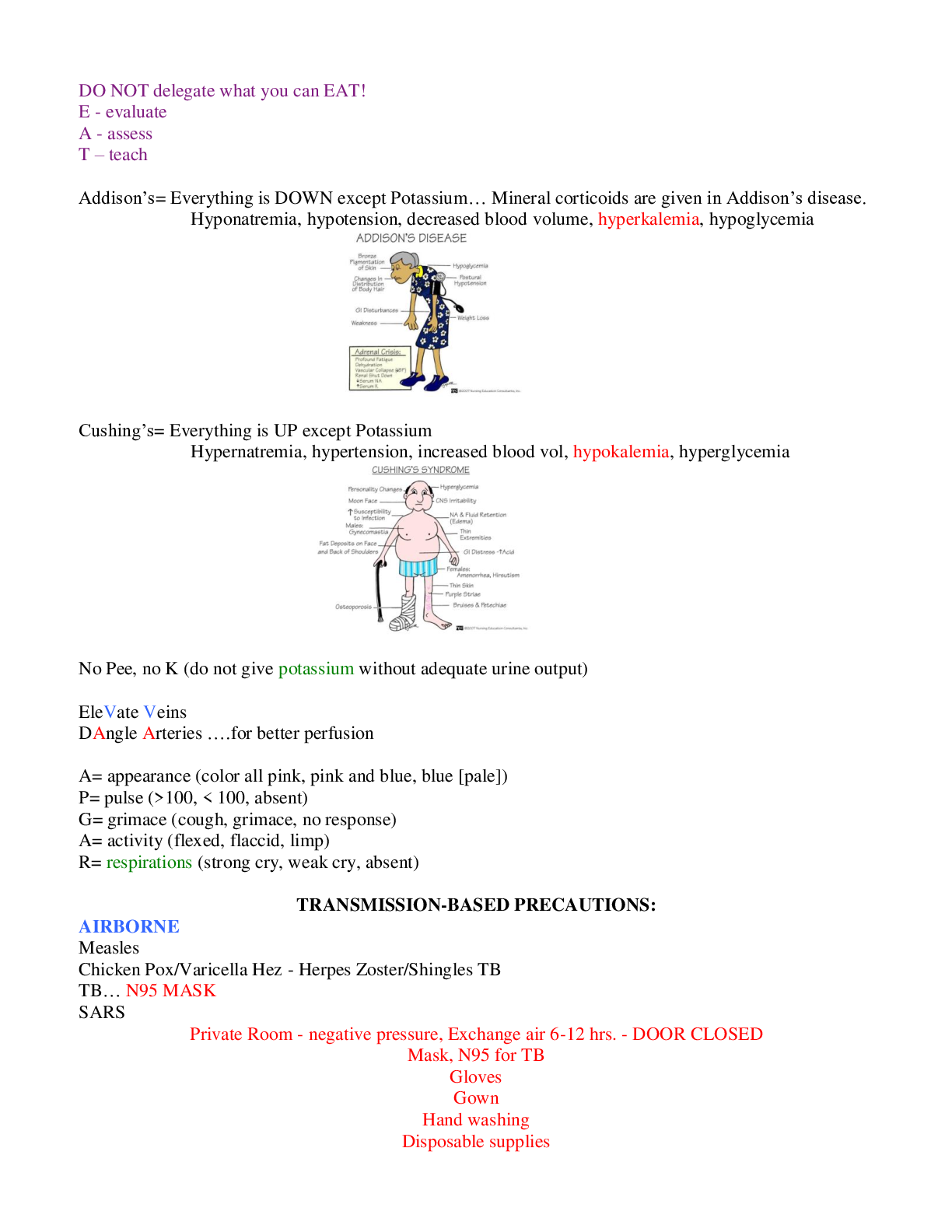
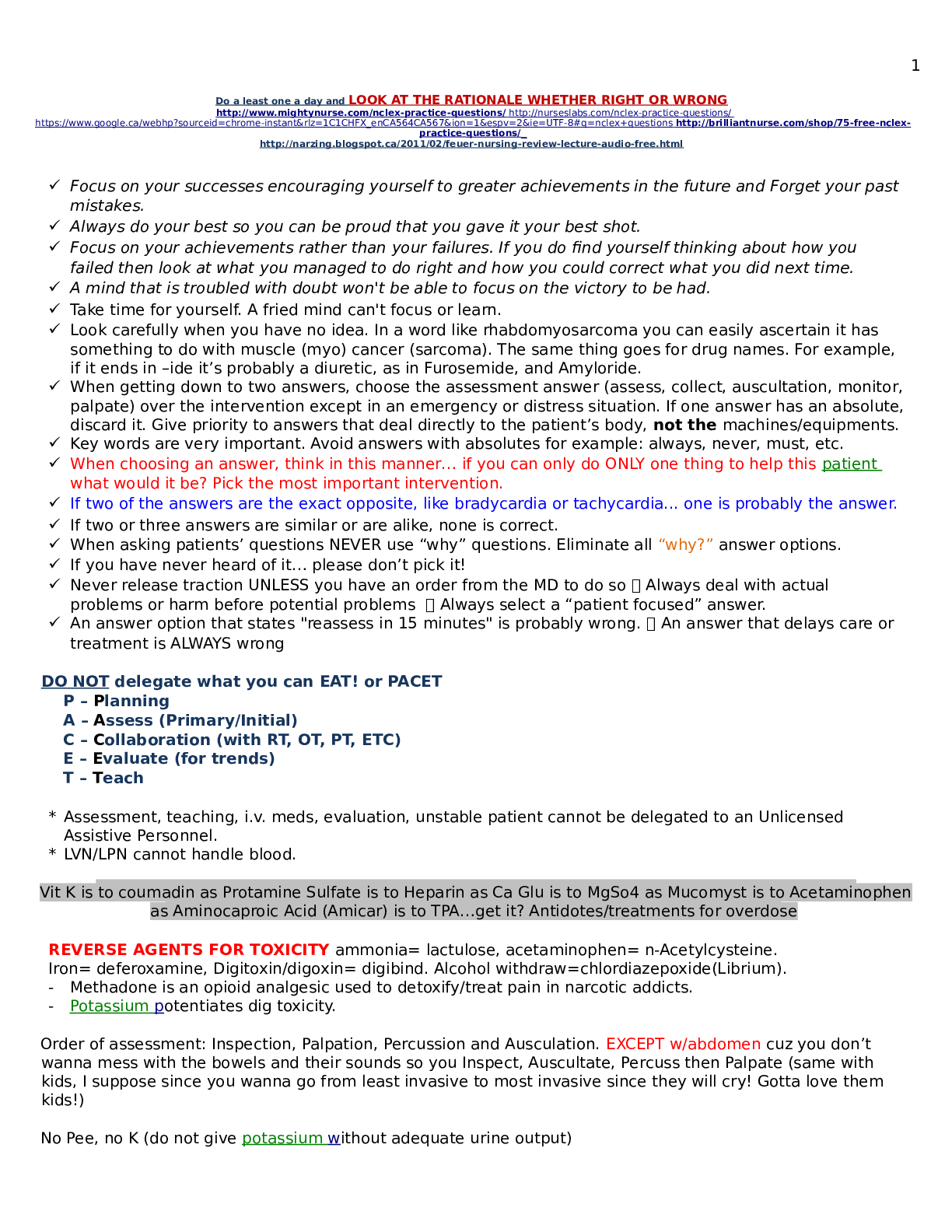
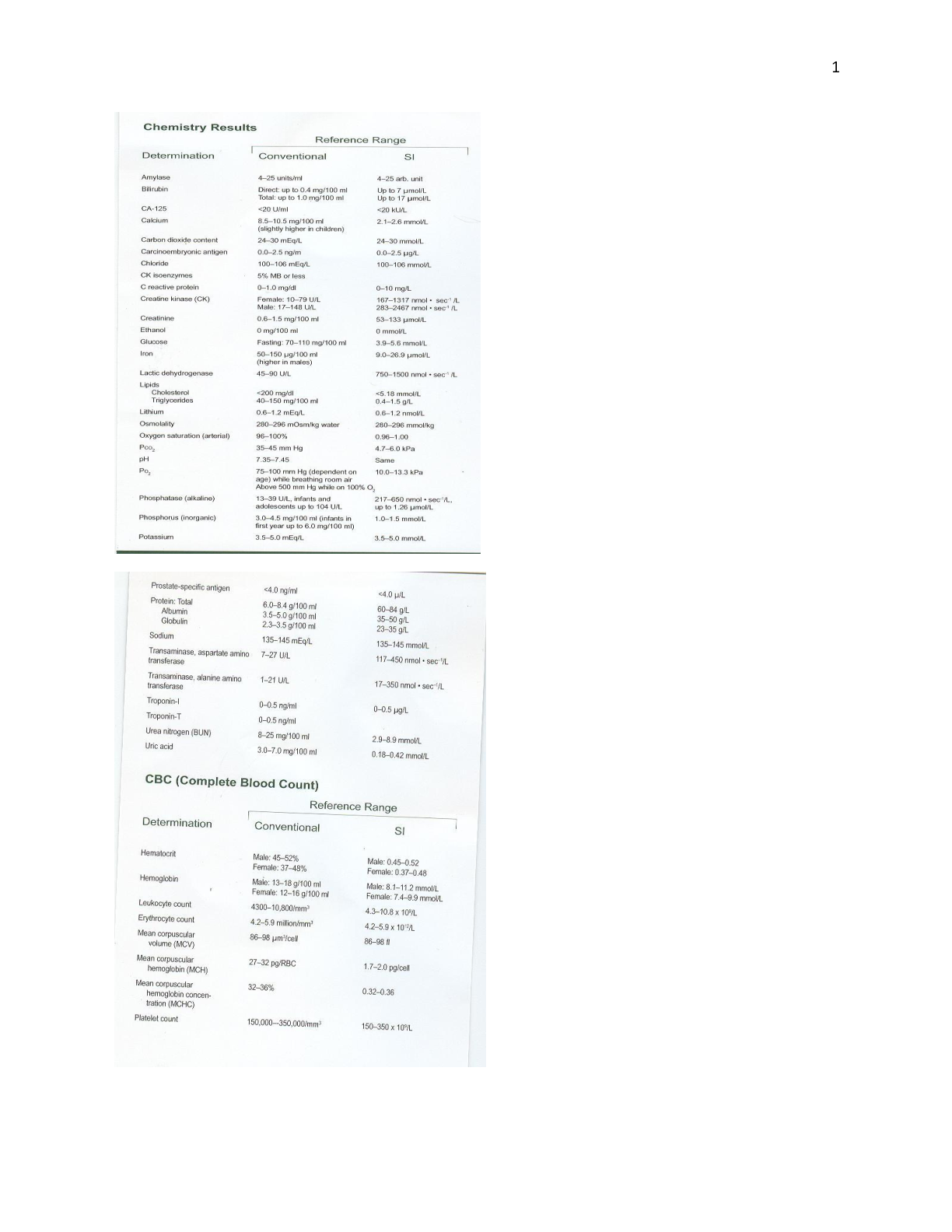
NCLEX/MedSurg Master Study Guide Nursing Process: A - assessment D - diagnosis O - outcome planning (specific, measurable, timely) Ex. The patient will walk 300 ft in the hallway by the end o... f the shift (3pm) P - planning Planning is done WITH patient, not FOR them. Let them assist in making goals that they see as doable I - intervention E - evaluation Reflecting on whether the goal was met/ what could be changed to help the pt. Reach it not evaluating **ourselves** we are evaluating whether or not the goal was MET Nursing Virtues: Beneficence - “do good” Non maleficence - “do no harm” Veracity - telling the truth, never lying or trying to deceive a patient If you make a med error, if a patient asks you about their disease Fidelity - keeping your promises Autonomy - pt. Is allowed (and supported) to make their own decisions Choosing treatment plans, right to advance directives, DNR orders, etc. Justice - providing fair care to all Providing equal care to patients no matter what (age, sex, race, LGBT, religion, disease) Confidentiality - keeping things between you and the patient If a patient tells you something, it should remain between the two of you The ONLY times you can break confidentiality are when the patient’s safety is involved (ex. Pt. is going to commit suicide, mandatory reporting of elder abuse, etc) Privacy - pt. Is entitled to their own personal privacy Closing the door /curtain when they are physically exposed/leaving the room if the patient is on the toilet Normal Lab Values: Digoxin 0.5-2, anything above 2 will give nausea, vomiting, diarrhea, and VISUAL disturbances (yellow halo around anything they are looking at) If the patient is hypokalemic (low potassium), makes it easier for them to go into Dig. toxicity Hold digoxin if their heart rate is below 60 bpm Lithium - 0.5-1.5, hold for anything higher! Tremors, confusion, seizures etc. Typically used for bipolar disorder Never double up 22 on lithium doses if you miss one -- safety! Lithium messes with their sodium! They need to stay stable with their sodium intake and consult their doctor before vigorous work outs / saunas / etc. because sweat can cause them to lose too much sodium. When they lose sodium, it makes it easier for lithium toxicity to occur Phenytoin/Dilantin 10-20 Used most often for seizure disorders Blood levels have to monitored over time to adjust dosage -- pt. Gets frequent lab draws Phenytoin reaction can cause anemia - dyspnea, fatigue, paleness, rashes, swelling and bleeding of the gums. BUN: 10-20, indicative of kidney function, monitor for nephrotoxic drugs Creatinine: 0.6-1.3, indicative of kidney function, monitor for nephrotoxic drugs INR (Warfarin) normal 1-2, on warfarin want it to be 2-3 to prevent clots PT (Warfarin) normal 11-13 seconds,want it to be 1.5-2x longer than that aPTT (Heparin) (remember 2 T’s in H) normal 30-45 seconds, want it to be 1.5-2.5x longer than that. <45sec =clots! Hgb 12-18% HCt female: 37-47%, male: 42-52% In pregnancy, H&H can **appear** lower because the woman’s plasma volume is expanding -- does not mean they are necessarily bleeding if H&H dips a little bit CVP (central venous pressure, in the heart) 2-6, low CVP is dehydration, high CVP is fluid overload High CVP = rales in lungs, JVD, dyspnea, tachycardia Low CVP = shock, signs of dehydration Platelets 150,000-400,000, below 150 we are worried about bleeding - bleeding precautions! ANC (Absolute neutrophil count) - ~2200-7000 Minimum urine in an hour: 30ml/hr GFR (glomerular filtration rate): should be above 60 with healthy kidneys WBC’s: 4,000-11,000 Sodium: 135-145 - low/high sodium causes neuro problems = confusion, altered LOC, coma ALL things potassium: Potassium: 3.5-5 -- altered potassium = HEART Dysrhythmias, mainly V-tach Foods with a lot of potassium: bananas, sweet potatoes We NEVER give potassium via IV push, it can kill the person!! K+ always given on IV pump, needs to be SLOW over 2-4 HOURS so that we don’t change their K+ too quickly; never more than 10 mEq/hr If patient has hyperkalemia - Give IV insulin and then immediately give IV dextrose - forces potassium back into cells so it is not floating around in the blood causing problems Hyperkalemia: HIGH potassium = peaked T waves, wide QRS, wide PR (everything is UP) Hypokalemia: LOW potassium = U wave at the end, depressed “low waves”, muscle cramps = especially CALF -- if pt has low potassium they can go into torsades = BAD Also tell patient to avoid “salt substitutes” in their diet because those oftentimes contain potassium in them instead Calcium: normal 8.6-10.2 Low calcium = crazy muscles! Laryngospasms*** priority because this is your throat! Airway compromise! Positive chvostek / trousseau’s sign Seizures Muscle tightness and cramping Hyperactive bowel sounds, diarrhea When to worry about low calcium?? After a thyroidectomy!! The parathyroid glands (which break down bone and put calcium into the blood) are on the thyroid….. So sometimes during surgery the parathyroid glands can be removed with the thyroid!! This will cause low low calcium = look for the low calcium signs when they get back from thyroid surgery! [Show More]
Last updated: 1 year ago
Preview 1 out of 35 pages
Reviews( 0 )
Document information
Connected school, study & course
About the document
Uploaded On
Oct 15, 2021
Number of pages
35
Written in

Additional information
This document has been written for:
Uploaded
Oct 15, 2021
Downloads
0
Views
107
.png)