*NURSING > STUDY GUIDE > Sepsis/Septic Shock UNFOLDING Reasoning Case Study Jack Holmes, 72 years old (Correctly and Fully an (All)
Sepsis/Septic Shock UNFOLDING Reasoning Case Study Jack Holmes, 72 years old (Correctly and Fully answered, Look no further).
Document Content and Description Below
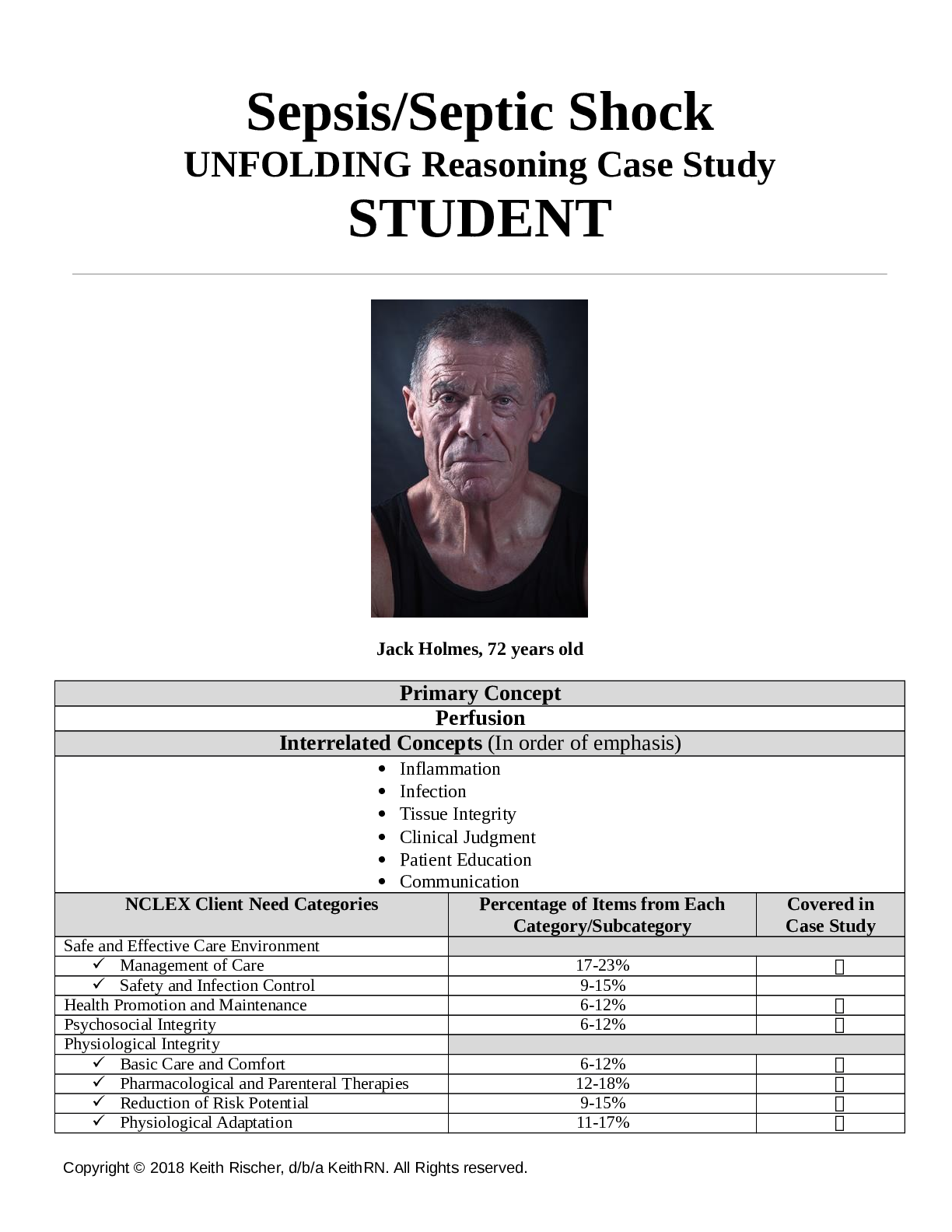
Sepsis/Septic Shock UNFOLDING Reasoning Case Study STUDENT Jack Holmes, 72 years old Primary Concept Perfusion Interrelated Concepts (In order of emphasis) • Inflammation • Infecti on • Tissue I... ntegrity • Clinical Judgment • Patient Education • Communication NCLEX Client Need Categories Percentage of Items from Each Category/Subcategory Covered in Case Study Safe and Effective Care Environment ✓ Management of Care 17-23% ✓ ✓ Safety and Infection Control 9-15% Health Promotion and Maintenance 6-12% ✓ Psychosocial Integrity 6-12% ✓ Physiological Integrity ✓ Basic Care and Comfort 6-12% ✓ ✓ Pharmacological and Parenteral Therapies 12-18% ✓ ✓ Reduction of Risk Potential 9-15% ✓ ✓ Physiological Adaptation 11-17% ✓ History of Present Problem: Jack Holmes a 72-year-old Caucasian male brought to the ED by ambulance from a skilled nursing facility (SNF). According to report from the paramedic, when the SNF nursing staff attempted to wake him this morning, he would not respond, and his BP was 74/40 with a MAP of 51. He has a history of Parkinson’s disease, COPD, CHF, HTN, depression, and a stage IV decubitus ulcer on his coccyx that developed three months ago. He does not follow commands, is unresponsive to verbal stimuli, but responds to a sternal rub with grimacing and withdrawing from stimulus. Personal/Social History: He has lived in the skilled nursing facility the past three years and has been bed bound the past year due to his advanced Parkinson’s disease. He was a heavy smoker, 1 PPD for 40 years until he moved to the SNF. What data from the histories are RELEVANT and must be interpreted as clinically significant by the nurse? (Reduction of Risk Potential) RELEVANT Data from Present Problem: Clinical Significance: Patient would not respond when tried to wake him, his BP was 74/40, Hx of Parkinson’s disease, COPD, CHF, HTN, depression and has a stage IV decubitus ulcer on his coccyx that developed 3 months ago. He does not follow commands, is unresponsive to verbal stimuli, but responds to a sternal rub with grimacing and withdrawing from stimulus. Patient was found unresponsive when found this morning with a BP of 74/40 which is extremely low. His Hx is significant because it can help us decide the cause of the low BP and his unresponsiveness. RELEVANT Data from Social History: Clinical Significance: He was a heavy smoker of 40 years (1PPD), he has been bedbound for the past year due to his advanced Parkinson’s disease. His smoker contributed to his Dx of COPD, and probably his HTN. Being bedbound and advancing progression of PD could be a contributing factor of his depression. Patient Care Begins Current VS: P-Q-R-S-T Pain Assessment: T: 103.4 F/39.7 C (oral) Provoking/Palliative: Not responsive verbally, withdraws to pain, no other indicators of pain P: 135 (irregular) Quality: R: 32 (regular) Region/Radiation: BP: 76/39 MAP: 51 Severity: O2 sat: 91% 2 liters n/c Timing: What VS data are RELEVANT and must be interpreted as clinically significant by the nurse? (Reduction of Risk Potential/Health Promotion and Maintenance) RELEVANT VS Data: Clinical Significance: Temp: 103.4F P:135 R:32 BP:76/39 O2 sat: 91% 2L of O2 via N/C Patient is febrile which indicates an infection is present. P&RR is high. BP and O2 sat is low. These are S&S of sepsis. Current Assessment: GENERAL APPEARANCE: Pale and warm to touch. Appears tense. RESP: Tachypneic and working hard to breathe, intercostal and suprasternal retractions present. Breath sounds diminished and light crackles in lower lobes bilat. Nail beds have noticeable clubbing, barrel chest present. CARDIAC: Pale, 1+ pitting edema lower extremities, systolic murmur with an irregular rhythm, radial pulses weak and thready, cap refill 3 seconds NEURO: Does not open eyes to sound or pain, withdraws to pain, incomprehensible sounds to painful stimuli, does not follow commands but does not resist when moved on a stretcher. PERRL GI: Distended abdomen, firm/nontender, bowel sounds hypoactive in all quadrants GU: Foley catheter placed to monitor urine output. 50 mL tea-colored urine with no sediment, and no odor present SKIN: Stage IV decubitus to coccyx 1 cm x 0.5 cm x 0.5 cm depth, wound bed with visual bone noted at the base with large areas of necrosis on both sides of the sacrum bone. When dressing was removed, a large amount of yellow/green purulent drainage on dressing with a foul odor. Mucus membranes dry and pale. Determine current Glasgow coma scale score based on neurological assessment data: Glasgow Coma Scale Eye Opening Spontaneous 4 To sound 3 To pain 2 Never 1 Motor Response Obeys commands 6 Localizes pain 5 Normal flexion (withdrawal) 4 Abnormal flexion 3 Extension 2 None 1 Verbal Response Oriented 5 Confused conversation 4 Inappropriate words 3 Incomprehensible sounds 2 None 1 Total What assessment data is RELEVANT and must be interpreted as clinically significant by the nurse? (Reduction of Risk Potential/Health Promotion & Maintenance) RELEVANT Assessment Data: Clinical Significance: RESP: Tachypneic and working hard to breathe, intercostal and suprasternal retractions present. Breath sounds diminished and light crackles in lower lobes bilat. Nail beds have noticeable clubbing, barrel chest present. CARDIAC: Pale, 1+ pitting edema lower extremities, systolic murmur with an irregular rhythm, radial pulses weak and thready. NEURO: Does not open eyes to sound or pain, withdraws to pain, incomprehensible sounds to painful stimuli, does not follow commands but does not resist when moved on a stretcher. GI: Distended abdomen, firm/nontender, bowel sounds hypoactive in all quadrants. SKIN: Stage IV decubitus to coccyx 1 cm x 0.5 cm x 0.5 cm depth, wound bed with visual bone noted at the base with large areas of necrosis on both sides of the sacrum bone. When dressing was removed, a large amount of yellow/green purulent drainage on dressing with a foul odor. Mucus membranes dry and pale. Patient’s respiratory status is compromised, cardiac status is compromised. Patient’s GI status is slowed. Patient’s skin integrity is compromised due to the pressure ulcer on his coccyx. All of this assessment data can indicate the patient is septic and leading to shock. Radiology Reports: What diagnostic results are RELEVANT and must be interpreted as clinically significant by the nurse? (Reduction of Risk Potential/Physiologic Adaptation) Radiology: Chest X-Ray Results: Clinical Significance: Cardiac silhouette slightly enlarged. No infiltrates present. Lab Results: Complete Blood Count (CBC) WBC HGB PLTs % Neuts Bands Current: 18.5 13.1 250 85.2 3 Most Recent: 12.4 13.2 175 64 0 What lab results are RELEVANT and must be recognized as clinically significant by the nurse? (Reduction of Risk Potential/Physiologic Adaptation) RELEVANT Lab(s): Clinical Significance: TREND: Improve/Worsening/Stable: WBC: 18.5 Neuts: 85.2% Bands-3 WBC and Neuts elevation indicate infection is present. Bands indicate that the body is overwhelmed. [Show More]
Last updated: 1 year ago
Preview 1 out of 19 pages
Instant download
Buy this document to get the full access instantly
Instant Download Access after purchase
Add to cartInstant download
Reviews( 0 )
Document information
Connected school, study & course
About the document
Uploaded On
Nov 13, 2021
Number of pages
19
Written in

Additional information
This document has been written for:
Uploaded
Nov 13, 2021
Downloads
0
Views
100

 (1).png)
.png)
