Health Care > ESSAY > HSM 410 Week 7 Course Project: Final Paper – An Individual Right to Die (Supreme Court of the Unit (All)
HSM 410 Week 7 Course Project: Final Paper – An Individual Right to Die (Supreme Court of the United States, dignity act) | Download To Score An A | DeVry University, Chicago
Document Content and Description Below
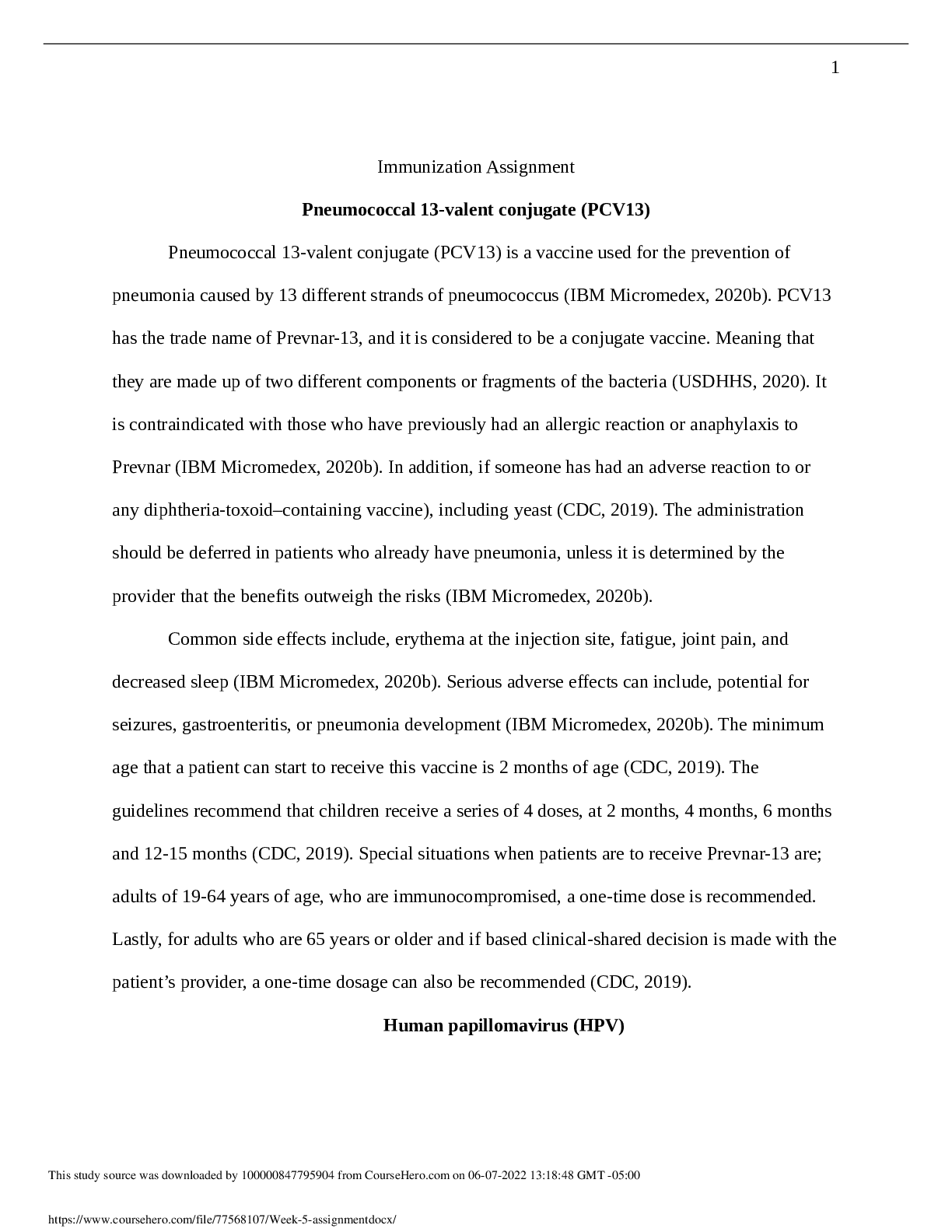
An Individual’s Right to Die Death with Dignity Act HSM 410 An Individual’s Right to Die An individual’s right to die is a topic of discussion that always brings up an argument regardless on... which side you choose to be on. It is so highly debated that there are only two states in the entire country that even have an act in place for a an individual to choose whether or not they want to continue to live, this being Oregon & Washington. The act that is in place in these two states is known as the Death with Dignity Act. Based off what you have just read, you might be thinking to yourself that Oregon & Washington are giving people the right to commit suicide whenever they feel like they want to. But this isn’t the case with the Death & Dignity Act. What these laws actually do is “allow mentally competent, terminally ill adult state residents to voluntarily request & receive a prescription medication to hasten their death” (Death with Dignity Acts). What these laws do for people is give them the option to die on there on terms, & that’s something that everyone should have the right to. The Death with Dignity Act went into affect in Oregon in 1997, & Washington followed with its own act in 2009. When referencing the Death with Dignity Act, many people bring up the terms physician-assisted suicide, physician- assisted death, & euthanasia. All these terms will be discussed later on in this paper. This document will present legislature that pertains to an individual’s right to die in the form of court rulings, arguments for & against these acts, religious beliefs, & my own personal perspective of the Death with Dignity Act. With something as serious as someone’s life, there has to be certain regulations in place for there to even be such a law that deals with taking an individual’s life. This is something that I believe would have been widely talked about when people were voting on whether or not to have the Death in Dignity Act passed in both Oregon & Washington. Now that these laws are in place, there are many rules that go along with it, assuring that not just any individual can take their own life. First of all, they must be a resident of either of the two states that has the act in place. People can’t just come from other states & expect that they will be able to use the law to their benefit. This also goes for the two states that have the act established, as in you can’t be a resident in Oregon & use the Washington’s Death with Dignity Act, or vise versa. As a resident of one of these two states, you must also be of at least 18 years of age, must be suffering from some type of terminal disease that is only giving you 6 months or less to live, & you must have decision-making capacity (Lunge). Now you might be wondering to yourself what exactly is meant when talking about decision-making capacity? Decision-making capacity is determined by a physician to see if the specific individual who is asking for the medication to end their life is in a right state of mind. That they are truly capable of making a major decision such as taking one’s life & that no one is forcing them to make this decision. This is where coercion is brought into question, physician’s have to be able to know that this is the sole choice of the individual & that even family members aren’t playing a role in the decision of whether the loved one is taking the medication. At the end of the day it’s up to the patient to sign the forms. Once a patient has decided to go forward with taking the medication then they must go through more steps to continue the process. “A patient must make one written & two oral requests for medication to end his or her life, the written one…signed, dated, witnessed by two persons in the presence of the patient who attest that the patient is “capable, acting voluntarily, & not being coerced to sign the request,” & there are stringent qualifications as to who may act as a witness” (Lunge, 2004, p.4). Once all of this is accounted for, the physician must inform the patient of how the medication will work, what could be potential risks, as well as alternatives to taking the medication such as hospice care. I believe that this step in the process is extremely important as it gives the patient knowledge about every aspect that is going on. By being informed about all the possibilities I think it gives the patient more reasoning in there thought process. After one physician has gone through all the tests with the patient such as seeing they are capable of making this type of decision, their voluntariness, & their diagnosis, another physician needs to conform it all as well. Now after all of that is taken care off, the patient can then receive the prescription to end their life. One thing that I thought made a lot of sense in all of this was the fact that at any moment that you wanted to cancel your previous decision of ending your life, you could. It wasn’t set in stone that once you gave the okay, there was no going back. If the patient does decide to go ahead & get the prescription, at that point it is up to the patient to administer the medication. A physician is not allowed to end the patient’s life, & this is where PAS, PAD, & euthanasia come in to play. Many people get physician-assisted suicide, physician-assisted death, & euthanasia confused with what exactly the Death with Dignity Act is all about. All a physician can really do is make sure that the terminally ill patient is in a right state of mind & write out the prescription for the medication. They aren’t allowed to administer the medication to the patient or any type of lethal injections as that would be known as euthanasia. Euthanasia is illegal throughout the United States & comes with some serious charges if you are found doing it. Mercy killing is also not allowed as you are still assisting in the death the patient. At the end of all this, a physician must a copy of the record to the state health division. The state health division must then issue an annual report that summarizes the experience with the statute (Lunge). As we move on we will discuss the court cases that pertain to the Death with Dignity Act. There are two court cases that directly have to do with the Death with Dignity Act. Washington v. Glucksberg will be the first one to be discussed. In this court case we had the dispute of whether or not it was a crime to have physicians aid in the death of a terminally ill patient. Physician’s wanted to be able to help there terminally ill patients the best way they could, even if the result was helping them pass along, but they couldn’t because of the petitioner’s ban that was against assisted suicides. It made its way all the way up to the Supreme Court, which upheld the ruling of Washington State’s legal ban on physician-assisted suicide (Washington v. Glucksberg). This was definitely a major win for the organizations that are pro- lifers as it ruled in their favor. Physician would not be able to prescribe medication to their terminally ill patients to end their own lives. The way the court looked at it was that they preventing people from just committing suicide, leaving the medical profession’s integrity in tact, & above all else avoiding any chance of falling into euthanasia. I think euthanasia was ultimately what made the judges rule in favor of upholding the rule because this is what most people are worried about when you argue against it. People don’t want physician’s to be able to just actively give anyone a lethal injection to that specific patient’s life. & I have to agree with that; I don’t think physicians or anyone for that matter should have that type of power. I see a difference between the Death & Dignity Act v. euthanasia. Yes they lead to the same result, but the way it is done & the process that you must go through with the Death & Dignity Act is different than that of simply giving someone a lethal injection. But it wasn’t a complete loss for those who apposed the court’s ruling. Soon after the court case had ended death-with-dignity supporters began to promote what would become known as the third path. Essentially the third path was the alternative for assisted suicide. “The “third path” involves the refusal or withdrawal of medical treatment – including both artificial & natural provision of hydration & nutrition – & proper palliative care, including pain management, during the ensuing “dying process” to be provided by hospice” (Lynne, 2005). This really changed the way people were looking at death. This wasn’t assisted suicide; this was simply rejecting any form of medical treatment. Instead of trying to prolong your life, a patient could simply pass away by not receiving any medical help, & this would still be completely up to the patient. What I also found interesting is that it religious groups who were pro-lifers didn’t have a problem with this. I think it’s because terminally ill patients were dying on their own without any medication, assistance from a physician, or assistance from anyone else. Moving forward, we also have another court case that took place in Oregon. The other court case that involved the Death with Dignity Act was Gonzales v. Oregon. In this case, we had a similar argument to that of the Washington v. Glucksberg court case. Those supporting the Death with Dignity Act claimed that terminally ill patients should have the right to ask their physician’s to help them in ending their life through the form of lethal medication. “Opponents maintained such action violates religious teachings on the sanctity of life & leads to a "slippery slope" toward euthanasia” (Johns, p.1). So as in the previous court case, we can see that the dispute is very similar to one another. They both regard whether or not a physician should be able to assist in a patient’s death. But there was a difference in this case as well, being who had the power in this case, federal or state. Oregon voters had already approved the law twice, but those opposing the law had stated that the law was violating the Controlled Substances Act that was under federal control. This case also made it all the way to the Supreme Court; here the supporting side stated that as a state they had the right to decide what constitutes proper medical practice (Johns). Which the Supreme Court upheld, they agreed with the proponents that the Controlled Substances Act doesn’t overrule the law that Oregon had in place. Physicians no longer had to worry about losing their licenses over prescribing lethal medicine to those that were covered by the Death with Dignity Act. Despite the dispute with this law there are positives that go along with it. The Death with Dignity Act can mean different things for any individual involved. We all at some point have had to deal with seeing someone we love go through their last days, whether it’s peaceful or in pain. It isn’t easy for anyone that is involved. & it is especially hard when the person is in constant pain & they just want death to come upon them. This is where I can see the Death with Dignity Act doing some good for families. It gives everyone that is involved a peace of mind, being able to know that the loved one’s suffering can finally end is a real blessing. It ultimately puts the patient back in control of their own life, they no longer have to wonder how much longer they are going to have to suffer through the pain they are experiencing. When you really think of it, the Death with Dignity Act only becomes available to the terminally ill patients when they have six months or less to live, so its not like it’s the first thing that is talked about with the physician. A physician is going to do absolutely everything they can to prolong the patient’s life. Once the physician is finding it hard to see how the patient will continue on living then things such as hospice, palliative care, & taking medication can be brought up. But what people need to realize is that the patients are receiving the information that they should be given. They way their options & move on from there. “Awareness of end-of-life care options is probably greater in Oregon, especially among health care professionals. Every Oregonian who has used [the Act] has been offered hospice care... Nearly 89% [of patients] over the six years were in hospice care at the time they ingested medication, 93% in 2003” (Lunge, 2004, p.24). So it’s not like they are simply giving people medication & sending them home on their way to go end their lives. It’s the exact opposite, for the most part they are already in some type of hospice care getting the attention they need for their last days & they medication is really more for a piece of mind. Again, sometimes all the patient really needs is to have the option of the medication. & as you can see more people are actually going into hospice or palliative care because of the Death & Dignity. While some people are for the act, there are always going to be people who argue against it as well. As we looked into both of the court cases, one thing that would stand out for those arguing against the Death with Dignity Act would be the religious aspect of it all. They would argue that by taking away someone’s life before their so-called time is to go, that they are playing with God’s plans for that specific individual. I’m a Christian myself, & I have mixed views on the act myself. But I do believe that a person should at least have the option to take the medication. There is also the argument that you are actively killing the terminally ill patient, but I see it more as physician’s helping the patient to let go & move on to the afterlife. Another thing that could be considered an argument is the ethical standpoint in all of this. As physician’s you are suppose to do everything that you can to preserve that person’s life. & by allowing the individual to choose the path of lethal medication the physician isn’t doing all they can to keep them alive. But I think as a physician you can see it from a different manner as well. Yes, you want to do everything you can for the patient, but sometimes death is the inevitable. I think a physician also has the responsibility to relieve a patient’s suffering if it becomes unbearable, & that where the Death with Dignity Act plays a positive role. “Another major objection to physician-assisted suicide is the loss of trust of a doctor. What will a patient think if it is known that their physician actively aided in someone else’s death?” (Boyd, p.3). Not everyone will see the physician in the same manner. Some will see that the physician was just helping someone who was suffering, while others may see it as the physician gave up on the patient. This could make some patients uncomfortable & even make them want to change to another physician. The physician also has the choice of een prescribing the medication in the first place though. They at no point have to be the one to go hrough the steps with the patient; the physicians can pass it along to someone else if they arent okay to do it themselves. There is debate for the Deth with Dignity Act. There are valid arguments to both sides. I am torn myself on the subject becuse I believe that we as people should have the right to be able to end our own lives if we are suffering from excruciating pain. At the same time though, I see how as a religious person that’s nt your way of thought. Regardless of what side you are on in this argument it’s always good tohave some knowledge on the subject. To inform yourself of what is out there so that you can ake the decision on your own. Even though Oregon & Washington are the only two stats that currently have the law in effect, others have tried, but with no luck. In 2011, Montana sent out three bills but all failed to pass (Death with Dignity Acts). One thing is for certain; this law will continue to be debated regardless of what side you are on. References Boyd, A. D. (n.d.). Physician-Assisted Suicide: For & Against. Retrieved from https://docs.google.com/viewer?a=v&q=cache:K7YLg- wTjgMJ:www.amsa.org/AMSA/Libraries/Committee_Docs/PhysicianAssistedSuicide.sfl b.ashx+&hl=en&gl=us&pid=bl&srcid=ADGEEShSpdt2pGGUqOjOC9kDKs- uXGBWGxdjluNaFI03CwozUPWF6D2iaseSBBaxhVtrDWak3To4bYRLJNW1IUD4tT6 EbqpZeC8SV3wbR9qg99PA-_hCc_Gx_7pryeHVH5- O3V8kv5vw&sig=AHIEtbQED17xHVq3Rpp8hki_OvbX3PuvKg&pli=1 Death with Dignity Acts. (n.d.). Retrieved November 9, 2012, from Death with Dignity National Center website: http://www.deathwithdignity.org/acts Johns, F. M. (n.d.). U.S. Supreme Court Upholds Oregon’s Right-to-Die Law A step toward securing death with dignity or a slippery slope toward accepting euthanasia? Retrieved November 30, 2012, from beliefnet website: http://www.beliefnet.com/News/2006/01/U- S-Supreme-Court-Upholds-Oregons-Right-To-Die-Law.aspx Lunge, R., Royle, M., & Slater, M. (2004). OREGON’S DEATH WITH DIGNITY LAW & EUTHANASIA IN THE NETHERLANDS: FACTUAL DISPUTES. Retrieved November 30, 2012, from http://www.leg.state.vt.us/reports/04death/death_with_dignity_report.htm Lynne, D. (2005, October 12). Anatomy Of Right-To-Die-Law. Retrieved November 30, 2012, from WND website: http://www.wnd.com/2005/10/32803/ Washington v. Glucksberg. (n.d.). Retrieved December 12, 2012, from Ascension Health website: http://www.ascensionhealth.org/index.php? option=com_content&view=article&id=260&Itemid=173 HSM 410 Healthcare Policy HSM 410 Week 1 DQ 1, What is Healthcare Policy HSM 410 Week 1 DQ 2, Foreign Healthcare HSM 410 Week 2 Course Project, Policy Paper Topic HSM 410 Week 2 DQ 1, U.S. Healthcare System Organization HSM 410 Week 2 DQ 2, Financing A Changing Healthcare System HSM 410 Week 3 Healthcare Interview Paper HSM 410 Week 3 DQ 1, Financial Cost Controls HSM 410 Week 3 DQ 2, Reimbursement Cost Controls HSM 410 Week 4 DQ 1, Access HSM 410 Week 4 DQ 2, Quality HSM 410 Week 4 Midterm Exam HSM 410 Week 5 Course Project Outline HSM 410 Week 5 DQ 1, The Baby Boomers - Are We Ready HSM 410 Week 5 DQ 2, The Future of Long-Term Care HSM 410 Week 6 DQ 1, Ethical Considerations in Health Care HSM 410 Week 6 DQ 2, The Importance of Prevention HSM 410 Week 7 Final Paper, Course Project HSM 410 Week 7 DQ 1, What is our Future HSM 410 Week 7 DQ 2, Obamacare – Patient Protection & Affordable Care Act [Show More]
Last updated: 1 year ago
Preview 1 out of 10 pages
Reviews( 0 )
Document information
Connected school, study & course
About the document
Uploaded On
Mar 03, 2022
Number of pages
10
Written in

Additional information
This document has been written for:
Uploaded
Mar 03, 2022
Downloads
0
Views
80






 (1).png)
.png)
.png)

.png)