NUR 397 /OB HESI Review Latest updated 2021/2022,100% CORRECT
Document Content and Description Below
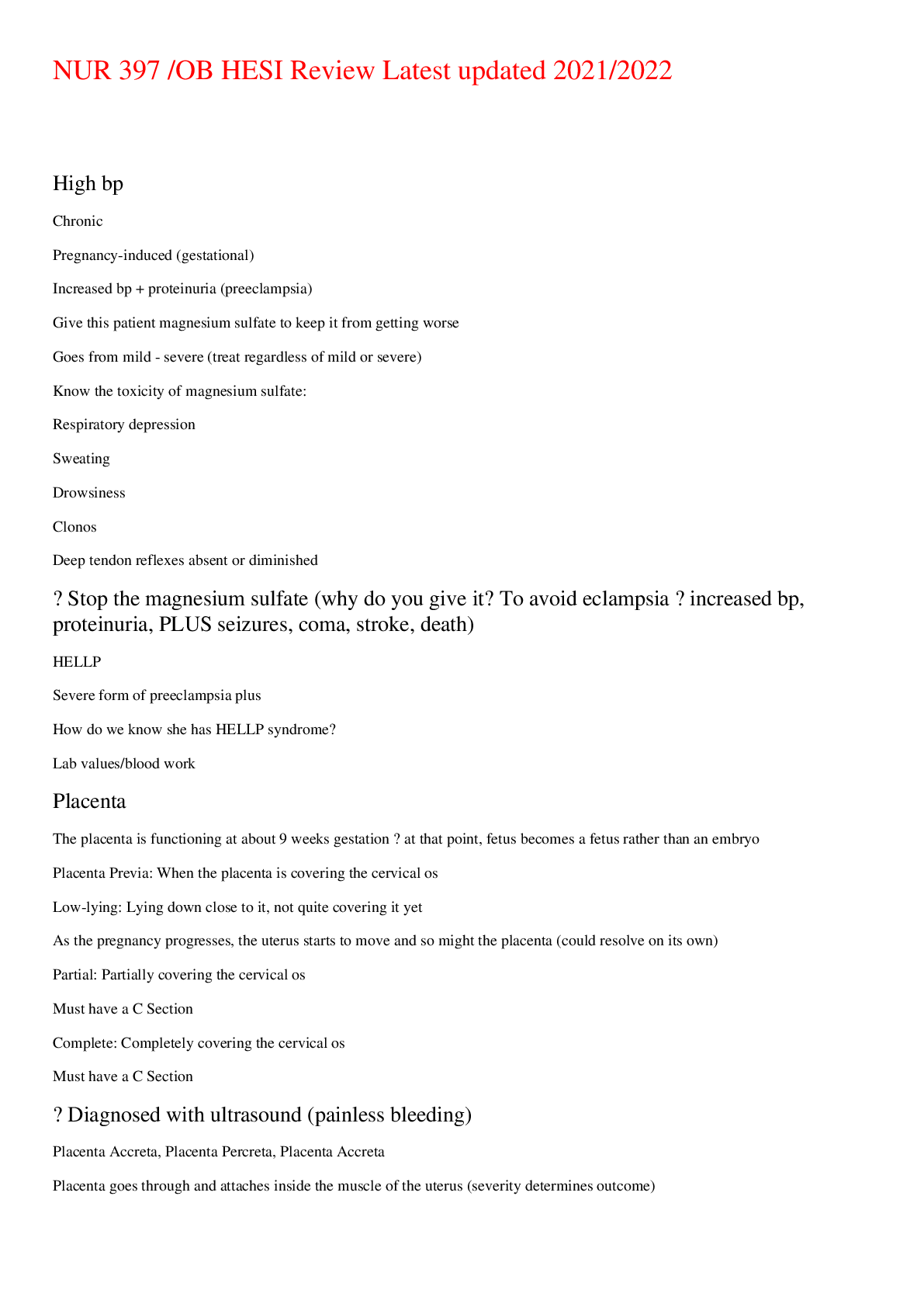
NUR 397 /OB HESI Review Latest updated 2021/2022 High bp ● Chronic ● Pregnancy-induced (gestational) ● Increased bp + proteinuria (preeclampsia) ● Give this patient magnesium sulfate ... to keep it from getting worse ● Goes from mild - severe (treat regardless of mild or severe) ○ Know the toxicity of magnesium sulfate: ■ Respiratory depression ■ Sweating ■ Drowsiness ■ Clonos ■ Deep tendon reflexes absent or diminished → Stop the magnesium sulfate (why do you give it? To avoid eclampsia → increased bp, proteinuria, PLUS seizures, coma, stroke, death) ● HELLP ○ Severe form of preeclampsia plus ○ How do we know she has HELLP syndrome? ■ Lab values/blood work Placenta ● The placenta is functioning at about 9 weeks gestation → at that point, fetus becomes a fetus rather than an embryo ● Placenta Previa: When the placenta is covering the cervical os ○ Low-lying: Lying down close to it, not quite covering it yet ■ As the pregnancy progresses, the uterus starts to move and so might the placenta (could resolve on its own) ○ Partial: Partially covering the cervical os ■ Must have a C Section ○ Complete: Completely covering the cervical os ■ Must have a C Section → Diagnosed with ultrasound (painless bleeding) ● Placenta Accreta, Placenta Percreta, Placenta Accreta ○ Placenta goes through and attaches inside the muscle of the uterus (severity determines outcome) → Also diagnosed with ultrasound (may end up with hysterectomy → high chance of hemorrhage) ● Abruptio Placentae ○ Placenta pulls away from the lining of the uterus ○ Can come on very quickly ○ Risk for hemorrhage ○ When you have abruptio placentae: ■ Painful bleeding ■ Rigid abdomen ○ Possible causes: ■ Cocaine use ■ Tobacco use ■ Any kind of accident (car crash, fell down stairs, etc.) ○ Remember, when placenta is pulled away, baby is no longer getting blood supply and consequently no oxygen → ~8 minutes to deliver baby ● If pt is in the hospital w abruptio placentae→ EFM: must look at heart rate AND contractions together ○ Late decelerations will show up Electronic Fetal Monitor ● Each square = 10 seconds ○ From one dark line to next dark line = 1 minute ● Top part = the baby ● Bottom part = the mother’s contractions ● Fetal heart rate range: 110 - 160 ● Must read both the fetal heart rate and the contractions TOGETHER to assess fetal well-being ○ If baby has a baseline of 110, doesn’t mean much of anything if we do not have contractions to compare it to ● VEAL CHOP ○ VC = Variable Decelerations ■ Indicates issues with the cord ■ Umbilical cord has wharton’s jelly to protect vessels ■ If there’s any kind of problem with the cord (knot, baby lying on it, etc.) we will see variable decelerations → FIRST, turn mother → to get baby off the cord Can also give mother some O2 (any kind of interruption of blood flow - the baby is not getting enough O2 → O2 deprivation leads to other issues with the baby, even death) Oligohydramnios - low amniotic fluid, fetus “floats” to the bottom, or doesn’t float at all, variable decelerations → Can give her amnioinfusion (when oligohydramnios or anhydramnios, normal saline in the uterus’ amniotic sac where the baby is. Done especially if the baby is not close to term. ● EH = Early Head ○ Head of baby is being compressed during the contractions ○ Mirror image ● AO = Acceleration Okay ○ When the baby’s baseline heart rate increases ● LP = Late Placenta ○ SERIOUS SITUATION (baby not getting any oxygen from the mother) → Turn patient, put on O2 (quickly) C section Rupture of membranes: TACO ( > 18 hours = higher risk of infection - ex. Chorio - you will have a temperature, pain, and amniotic fluid will have very foul odor - baby at risk for contracting chorio and requiring antibiotics; endometritis; sepsis → death) ■ T = Time ■ A = Amount ■ C = Color ● Any other color besides clear → something is wrong ■ O = Odor ○ Spontaneous Rupture of Membrane (SROM) ○ Artificial Rupture of Membranes (AROM - aka Amniotomy) ■ Must look first at FETAL HEART RATE ■ Also make sure nothing is coming from the vagina (ex. Prolapsed cord → emergency situation - emergency C Section) ○ Premature ROM (PROM) ○ Preterm Premature ROM (PPROM) Menarche to Menopause ● Health history is absolutely vital to treat patient in best way possible ● Birth control types: go over natural planning bc method → average person has a 28-day cycle where woman starts bleeding on day 1, ovulates on day 14, then last day before next period is the 28th day ○ Most fertile right before and right after ovulation ● STIs: understand bacterial vs viral ○ Bacterial: Treated and will go away ○ Viral: Can be treated, but will not go away (will return) ● Pre Pregnancy Counseling ○ FOLIC ACID → helps to prevent neural tube defects ○ Prenatal vitamin = enough folic acid ○ Teach pt first about when she is going to ovulate, educate that she takes prenatal vitamin or folic acid ● Naegele's Rule ○ To determine when a woman is going to deliver ● Pregnancy test ○ Determine hCG (will increase as pregnancy increases) ■ Loss of pregnancy or ectopic, other issues → hCG will be lower ■ Multiples and molar pregnancy → hCG will increase ● Quickening: Fetal movements ● GTPAL ○ When coming into prenatal visit WOMAN IS PREGNANT (Only disregard as a pregnancy if she is visiting something like dermatologist) ● GP = gravida and parity ○ Parity = a delivery after 20 weeks ● Alpha fetoprotein ○ 15 - 20 weeks ○ High levels could indicate neural tube defects or twins; low levels could indicate down syndrome ● High-Risk Pregnancies ○ Obesity ○ Advanced Maternal Age (AMA) ○ STIs ○ Gestational Diabetes ○ Incompetent cervix → cerclage ○ Large babies ○ Preeclampsia ● The most common place for ectopic pregnancy = in the fallopian tubes ● Preterm Labor ○ Could be brought on by ■ Dehydration (ex. from hyperemesis) ■ UTI ■ Cocaine use and tobacco (bc of vasoconstriction) ○ Tocolytic therapy to repress the labor ● True labor = contractions at regular rate - don’t go away with bath/shower or walking - consistent ● False labor = contractions will go away ● Doula = person hired to help with coaching of delivery ○ Could also be someone to lean on after delivery ● VDAC = Vaginal Delivery After Cesarean ○ If you have had C section, remember tissues are no longer as strong ■ Rupture risk increases with post C sections bc muscle fibers are cut and then mended, causing a weak spot KNOW BISHOP SCORE → Dilation is when the woman’s cervix will dilate or get bigger ( 0 - 10 cm) ● 10 cm = size of Moon Pie/Bagel → Effacement is the thinning of the cervix (0 or closed - 100 or complete) ● Cervix is very thin at completion → Station ( 0 negative to 0 positive) **Ischial spine is most narrow part of the pelvis → Imaginary line across it is the 0 station ● Baby higher than ischial spine = negative ● Baby lower = positive; closer to delivery - happy/good Beta Strep screen tells us if mother is positive or negative for group beta strep ● Can affect the baby → Will give mom antibiotics (ex. penicillin during labor - penicillin before that will not be helping the baby) Pain Management ● Alternative therapies are safest Spinal block is used for C section ● Because it is one and done ● Give medication, lasts for ~ 3 hours ● Must be concerned about spinal headache that may occur after spinal block is given Epidural given most of the time for vaginal delivery ● Catheter stays in place for additional doses ○ Don't know how long it will last General Anesthesia given in emergency C section - no time for spinal block ○ Woman could end up with aspiration of stomach contents*** Who is prone to hemorrhaging? Fundal rub - when in doubt, massage the fundus ● You want it to be firm - firm is fine ● Boggy is blood, bad ● Boggy to the side means the bladder is full ● Not getting anywhere with fundus massage? Empty bladder! Then massage fundus. Involution and subinvolution ● Involution = uterus returns to its nonpregnant state ● Subinvolution = failure of the uterus to return to its nonpregnant state Any kind of blood disorder, clotting disorder → be aware of *** Thrombosis → DVT, Superficial, do NOT rub the legggggg ● Does it make a difference if you put the head of the bed up? NO ● Ambulate quickly ● Do not want dislodge and go to the lungs to cause a PE Lochia ● Rubra ○ If you have lochia rubra at 2 weeks, there is something wrong ● Serousa ● Alba Breastfeeding ● Recommended breastfeed exclusively for the first 6 months ● Very first couple of days you will have colostrum (high in antibodies and protein) ○ 72 - 96 hours later milk will come in Milk suppression ● No stimulation to breasts ○ Firm-fitting bra ○ No warm showers, no bra, etc. ● Engorgement is when there is a lot of milk that comes in and causes breasts to feel uncomfortable ○ Best thing to do is feed your baby ○ Not breastfeeding? Something cold on your breasts (compresses, cabbage leaves) ● Mastitis comes across as feeling like the flu. Comes on very quickly, swelling, pain heat from one area → plugged milk duct ○ Treated with antibiotics Newborn post-delivery ● After delivery newborn has APGAR at 1 minute and 5 min ● Vitamin K produced in intestine by bacteria - infant has been in sterile environment so no clotting factor in first 7 days ○ Vitamin K promotes clotting ○ Vitamin K does not cross the placenta ● Meconium and urination within 24 hours ● Know reflexes!!!!*** ○ Babinski goes away ○ When do fontanelles go away? ■ Anterior = 12 - 18 months ■ Posterior = by the end of the 2nd month ● Newborns → Figure out if they have patent airway and respirations, good circulatory system, then thermoregulation ○ Make sure they do not lose any heat → Important to teach mother and significant other/caretaker (avoid hypothermia that can lead to cold ● Necrotizing Enterocolitis [Show More]
Last updated: 1 year ago
Preview 1 out of 13 pages
Reviews( 0 )
Document information
Connected school, study & course
About the document
Uploaded On
Apr 17, 2022
Number of pages
13
Written in

Additional information
This document has been written for:
Uploaded
Apr 17, 2022
Downloads
0
Views
40



 (1).png)