Human Nutrition > iHuman > Abdominal pain. The pain is in the right upper quadrant of her abdomen (All)
Abdominal pain. The pain is in the right upper quadrant of her abdomen
Document Content and Description Below
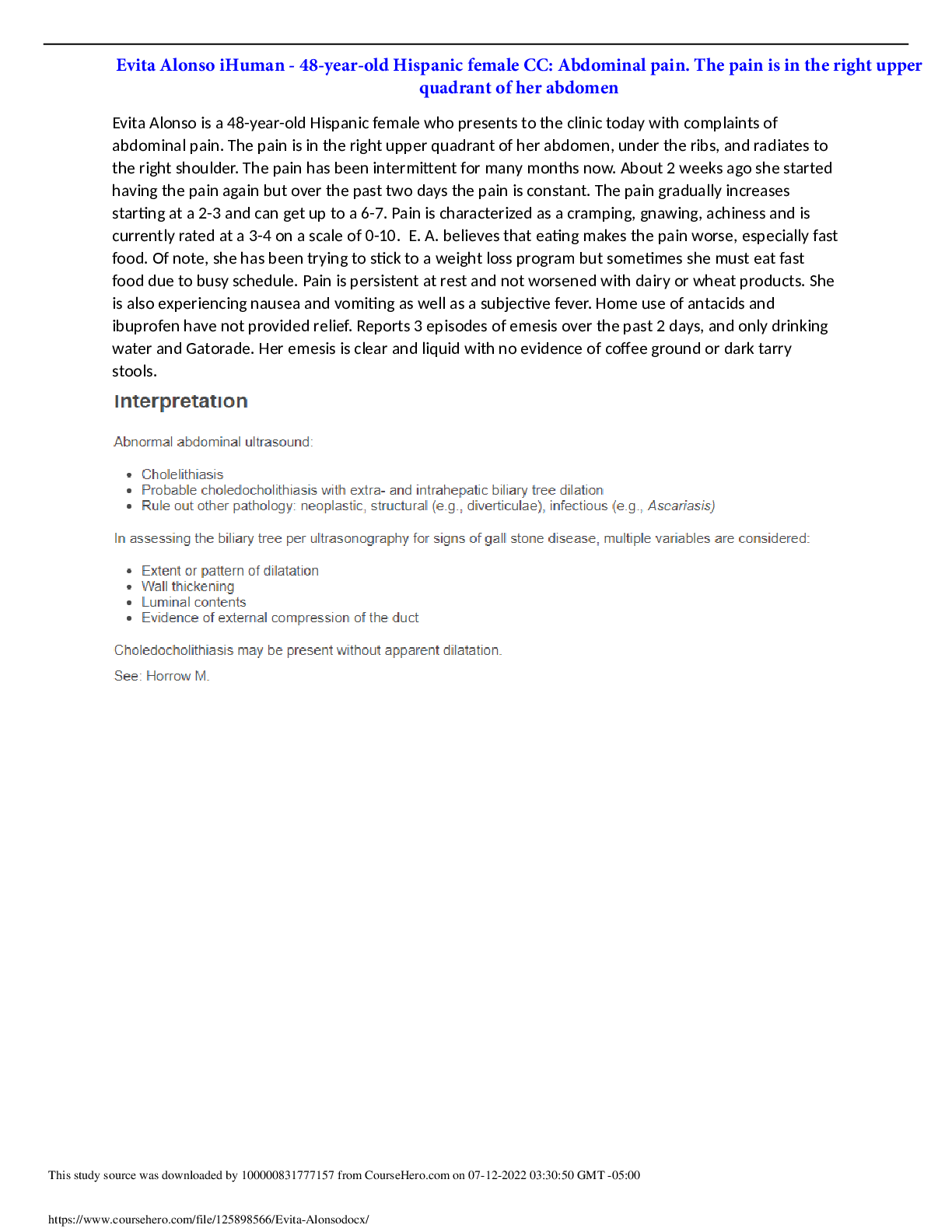
Evita Alonso is a 48-year-old Hispanic female who presents to the clinic today with complaints of abdominal pain. The pain is in the right upper quadrant of her abdomen, under the ribs, and radiates t... o the right shoulder. The pain has been intermittent for many months now. About 2 weeks ago she started having the pain again but over the past two days the pain is constant. The pain gradually increases starting at a 2-3 and can get up to a 6-7. Pain is characterized as a cramping, gnawing, achiness and is currently rated at a 3-4 on a scale of 0-10. E. A. believes that eating makes the pain worse, especially fastfood. Of note, she has been trying to stick to a weight loss program but sometimes she must eat fast food due to busy schedule. Pain is persistent at rest and not worsened with dairy or wheat products. She is also experiencing nausea and vomiting as well as a subjective fever. Home use of antacids and ibuprofen have not provided relief. Reports 3 episodes of emesis over the past 2 days, and only drinking water and Gatorade. Her emesis is clear and liquid with no evidence of coffee ground or dark tarry stools. Additional labs or diagnostic tests: BMP- hydration and electrolyte statusLFT- liver function including direct and indirect bilirubin levelsMRCP- evidence on abdominal ultrasound of extra- and intrahepatic biliary tree dilation. May need prior insurance authorization. This testing may also be ordered by Gastroenterologist. Zakko and Afdhal (2021)suggests evaluation for concurrent choledocholithiasis in patients with acute cholecystitis who have evidence of common bile duct dilation on ultrasound. Consults: Hospital admission. Consult Gastroenterology for possible cholecystectomy and further work up. Direct admit orders outlined in therapeutic modalities section below. Therapeutic modalities: Supportive care to include IV hydration (NS @ 75ml/hr), pain control (Toradol 30mg IV every 6 hours PRN pain- MAX dose 120 mg/day; max duration 5 days), empiric antibiotic therapy (Zosyn 3.375 g IV every 6 hours for 7 days), and nothing per mouth (Vollmer, 2021). Zofran 4mg IV every 6 hours as needed for nausea/vomiting. POC blood glucose every 4 hours to monitor for hypoglycemia due to NPO status. Non-pharmacologic therapies may consist of cool wash cloth to head and neck for nausea. Keep head of bed elevated. Consider NG tube insertion if emesis persists after usedof Zofran. Health Promotion: Pap smear and lipid panel previously performed at visit 4 months ago. Mammogram previously ordered at visit 4 months ago using walk-in clinic service, follow up on completion of testing and results. Breast Cancer Screening: With family history of breast cancer in first degree relative- mammograms yearly and consider BRCA gene testing.Colorectal Cancer Screening: Grade B recommendation for adults aged 45-49 (US Preventive Services Task Force, 2021a). Prediabetes/Type 2 Diabetes Screening: Grade B recommendation for adults ages 35-70 who are overweight or obese (US Preventive Services Task Force, 2021b). Order hemoglobin A1C, due to age and BMI of 27.4.Immunizations: yearly influenza vaccine, Covid series including booster if eligible, tdap every 10 yearsPatient education: The gallbladder is a small organ that is a part of your gastrointestinal system which stores and excrete bile to help the body break down fat. Gallstones can form and clog the organ. In your case the gallstones have caused symptoms such as the abdominal pain, right shoulder pain, nausea, and vomiting. You need to be admitted to the hospital because according to the tests we ran you may have a clogged duct leading to inflammation and infection. This is not a disease process that is typically treated as an outpatient. You may require surgery or additional testing such as an MRCP to look at the ducts. Thesurgery which may be needed is called a cholecystectomy. It is a very common procedure performed andis often done laparoscopically and can sometimes be performed as an outpatient procedure. The procedure itself does have some risks since anesthesia is required, but after the gallbladder is removed there will be no return of gallstones. You have an increased risk of forming gallstones when you are overweight (Crowley & Martin, 2022). After discharge, and you are cleared to resume a regular diet, try to increase your compliance with your diet by devoting one day a week to meal prep. This allows you to have meals already packed and ready to eat when you are in the middle of your busy day and decreases the incidence of eating fast food. Additionally, for your knee pain it is ok to take some ibuprofen, but you may try to alternate between ibuprofen and acetaminophen to prevent injury to your stomach lining. Tryice, rest, and elevation of knees at the end of a long day. You can also use OTC topicals such as BioFreeze,Tiger Balm, or Voltaren gel. Your knee pain may decrease with weight loss. If not, we can look at consulting Orthopedics in the future. Disposition/follow-up instructions: Follow up in clinic 1-3 weeks after discharge. If gallbladder is removed, decrease fat in diet and eat small meals. Avoid any strenuous activities or lifting. Take pain medication as prescribed. Contact physician if pain is not adequately controlled. If you have symptoms ofinfection such as fever/chills or bleeding, contact office sooner for an appointment. Get plenty of rest and drink fluids. References Crowley, K., & Martin, K. A. (2022). Patient education: Gallstones (The Basics). UpToDate. https://www.uptodate.com/contents/gallstones-the-basics?search=cholecystitis%20diagnosis&topicRef=666&source=related_linkUS Preventive Services Task Force. (2021a). Screening for Colorectal Cancer: US Preventive Services Task Force Recommendation Statement. JAMA, 325(19), 1965-1977. https://jamanetwork.com/journals/jama/fullarticle/2779985US Preventive Services Task Force. (2021b). Screening for Prediabetes and Type 2 Diabetes: US Preventive Services Task Force Recommendation Statement. JAMA, 326(8), 736-743. https://jamanetwork.com/journals/jama/fullarticle/2783414Vollmer, C. M., Zakko, S. F., & Afdhal, N. H. (2021). Treatment of acute calculous cholecystitis. UpToDate. https://www.uptodate.com/contents/treatment-of-acute-calculous-cholecystitis?search=cholecystitis&source=search_result&selectedTitle=2~150&usage_type=default&display_rank=2Zakko, S. F., & Afdhal, N. H. (2021). Acute calculous cholecystitis: Clinical features and diagnosis. UpToDate. https://www.uptodate.com/contents/acute-calculous-cholecystitis-clinical-features-and-diagnosis?search=cholecystitis%20diagnosis&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1#H15 SSL site seal Better Business Bureau accredited business [Show More]
Last updated: 1 year ago
Preview 1 out of 4 pages
Reviews( 0 )
Document information
Connected school, study & course
About the document
Uploaded On
Jul 14, 2022
Number of pages
4
Written in

Additional information
This document has been written for:
Uploaded
Jul 14, 2022
Downloads
0
Views
61
 2021.png)