Mark Klimek transcript: ANTICHOLINERGIC vs. CHOLINERGIC EFFECTS.
Document Content and Description Below
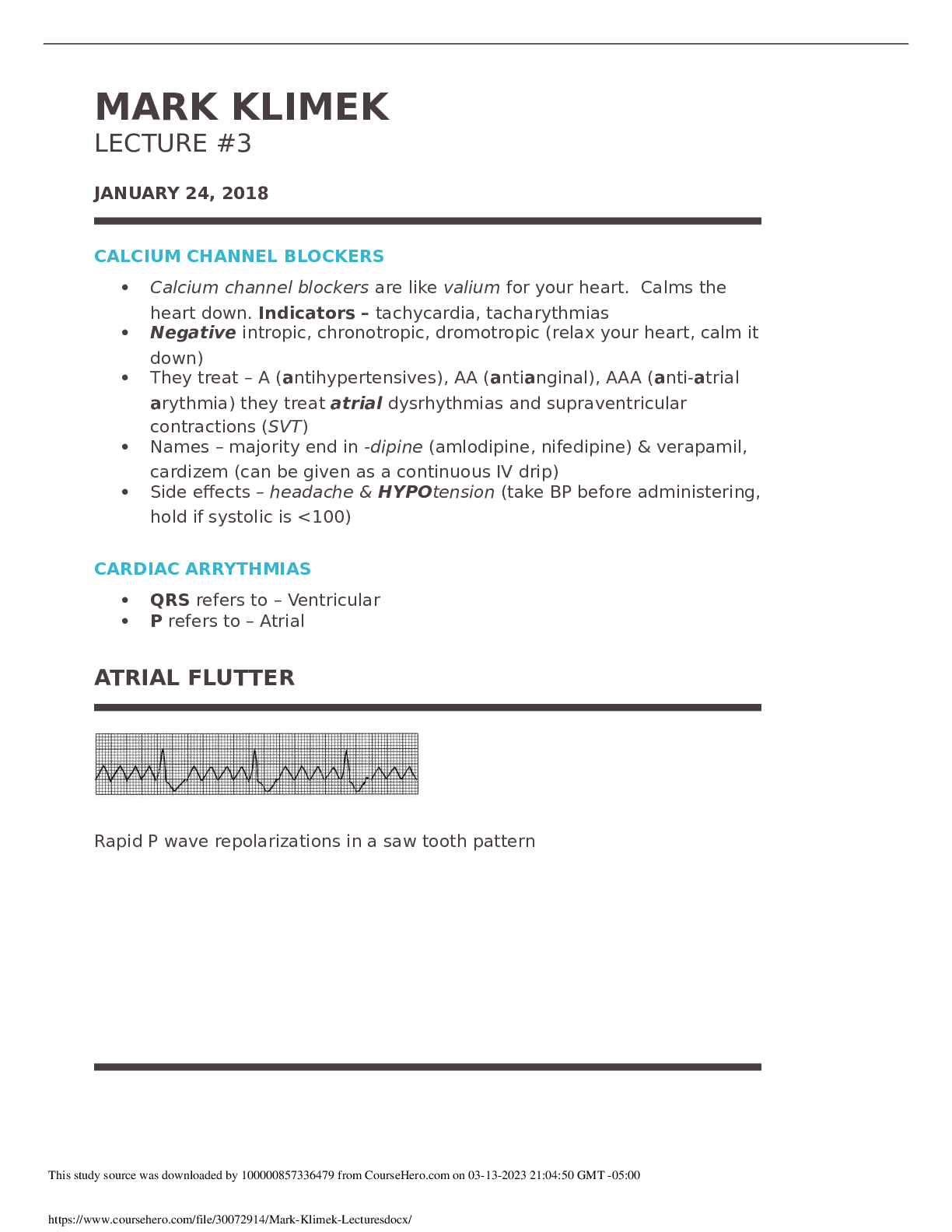
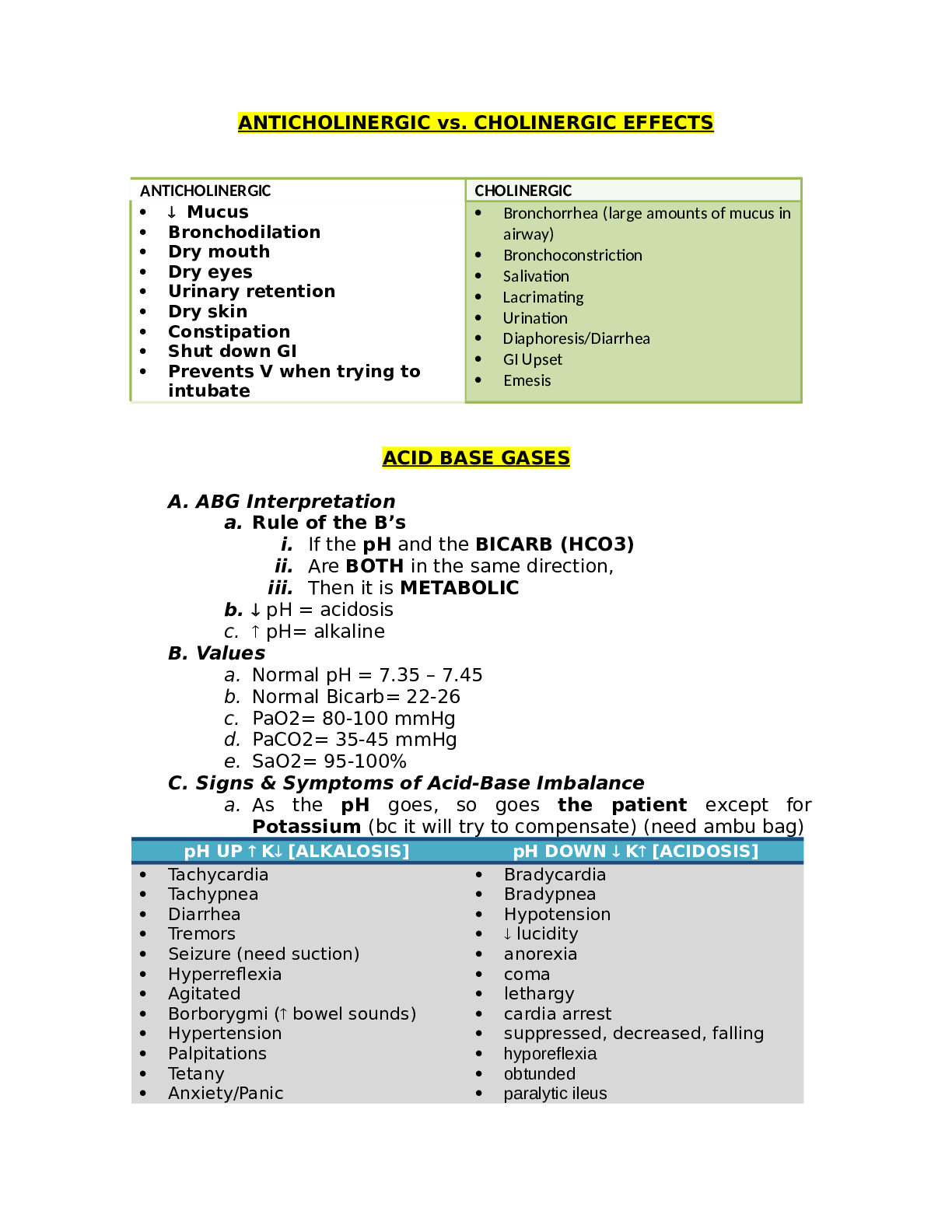
ANTICHOLINERGIC vs. CHOLINERGIC EFFECTS ANTICHOLINERGIC CHOLINERGIC • Mucus • Bronchodilation • Dry mouth • Dry eyes • Urinary retention • Dry skin • Constipation • S... hut down GI • Prevents V when trying to intubate • Bronchorrhea (large amounts of mucus in airway) • Bronchoconstriction • Salivation • Lacrimating • Urination • Diaphoresis/Diarrhea • GI Upset • Emesis ACID BASE GASES A. ABG Interpretation a. Rule of the B’s i. If the pH and the BICARB (HCO3) ii. Are BOTH in the same direction, iii. Then it is METABOLIC b. pH = acidosis c. pH= alkaline B. Values a. Normal pH = 7.35 – 7.45 b. Normal Bicarb= 22-26 c. PaO2= 80-100 mmHg d. PaCO2= 35-45 mmHg e. SaO2= 95-100% C. Signs & Symptoms of Acid-Base Imbalance a. As the pH goes, so goes the patient except for Potassium (bc it will try to compensate) (need ambu bag) pH UP K [ALKALOSIS] pH DOWN K [ACIDOSIS] • Tachycardia • Tachypnea • Diarrhea • Tremors • Seizure (need suction) • Hyperreflexia • Agitated • Borborygmi ( bowel sounds) • Hypertension • Palpitations • Tetany • Anxiety/Panic • Poly • Bradycardia • Bradypnea • Hypotension • lucidity • anorexia • coma • lethargy • cardia arrest • suppressed, decreased, falling • hyporeflexia • obtunded • paralytic ileus • respiratory arrest (need ambu bag) D. Causes of Acid-Base Imbalance a. First ask, “Is it Lung?” i. If YES- then it is Respiratory b. Then ask yourself: i. Are they Overventilating or Underventilating? 1. If Overventilating pick Alkalosis 2. If Underventilating pick Acidosis c. If not lung, then it’s Metabolic i. If the patient has prolonged gastric vomiting or suction, pick Metabolic Alkalosis ii. For everything else that isn’t lung, pick Metabolic Acidosis (Kussmaul – MacKussmaul) 1. Also, if you don’t know what to pick choose Metabolic Acidosis VENTILATOR ALARMS 1. High Pressure Alarms are triggered by resistance to air flow and can be caused by obstructions of three types: a. Kinked Tube i. NRS ACTION: Unkink it b. Water in tubing (caused by condensation) i. NRS ACTION: Empty it/Remove H2O c. Mucus in airway i. NRS ACTION: Turn, Cough&DeepBreathe; only use suction if C&DB fails, as a last resort 2. Low Pressure Alarms are triggered by resistance to air flow and can be caused by disconnections of the: a. Tubing i. NRS ACTION: Pay attention to where tubing is…(contamination) ii. If on floor, change out iii. If on chest, clean with alcohol then put back on 3. Respiratory Alkalosis (Overventilation) means ventilator settings may be too HIGH. 4. Respiratory Acidosis (Underventilation) means ventilator settings may be too LOW. 5. To “Wean” To gradually and incrementally decrease with the goal of ridding all together ALCOHOLISM Note: Remember in a psych question if you are asked to prioritize DO NOT forget Maslow! Use the following priorities: 1. Physiological 2. Safety 3. Comfort 4. Psychological 5. Social 6. Spiritual Also, ALL PSYCH PATIENTS START AS MED SURG PATIENTS…RULE OUT ALL FEASIBLE MED ANSWERS BEFORE PICKING PSYCH ANSWERS 1. Psychodynamics of Alcoholism a. The #1 psychological problem in abuse is DENIAL. i. Definition: 1. Refusal to accept the reality of their problem. ii. Treatment: 1. Confront it by pointing out to the person the difference between what they say and what they do. 2. In contrast, support the denial of loss and grief (BC the use of denial is serving a functioning person) b. DEPENDENCY/CODEPENDENCY i. Dependency: When the abuser gets the significant other to do things for them or make decisions for them. ii. Codependency: When the significant other derives positive self-esteem from doing other things for or making decisions for the abuser. iii. Treatment: 1. Set boundary (limits) and enforce them. Agree in advance on what requests are allowed then enforce the agreement 2. Work on the self-esteem of the codependent person. c. MANIPULATION i. Definition: When the abuser gets the significant other to do things for him/her that are not in the best interest of the Significant Other. The nature of the act is dangerous or harmful to the significant other ii. Treatment: 1. Set limits and enforce 2. Its easier to treat than dependency/codependency because nobody likes to be manipulated 2. Wernicke’s (Korsakoff’s) Syndrome a. Psychosis induced by Vitamin B1 (Thiamine) deficiency. b. Primary symptom: amnesia with confabulation (making up stories to fill in memory loss—believe as true) c. Characteristics: i. Preventable 1. By giving B1 vitamins ii. Arrestable 1. Can stop from getting worse- not imply better iii. Irreversible 1. Dementia symptoms don’t get better—only worse 3. Antabuse/Revia a. Disulfiram (drugs used for alcoholism b. Aversion Therapy – really strong hatred for something c. Onset and duration of effectiveness: 2 weeks i. Take drugs 2 weeks and builds up in blood to a level that when drinking ETOH will become horribly sick; if off for two weeks, will be able to drink without sickness again d. Patient teaching: Avoid ALL forms of alcohol to avoid nausea, vomiting, and possibly death, including: i. Mouthwash, aftershave, perfumes/cologne, insect repellant, vinigarettes (salad dressings), vanilla extract, elixirs (contains alch-OTC med), alcohol prep pad, alch sanitizers OVERDOSE VS. WITHDRAWAL First ask yourself, is the drug an upper or a downer? UPPERS DOWNERS Names: • Caffeine • Cocaine • PCP/LSD (Psychedelic hallucinogens) • Methamphetamines-speed • ADHD- adderrall/Ritalin • Bath Salts (Cath-Kath) Names: • Everything else Signs/Symptoms: • Tachycardia • Hypertension • Diarrhea, borborygmi • Agitation • Tremors • Clonus • Belligerence • Seizures, need suction • Exaggerated, shrill, high pitched cry • Difficult to console Signs/Symptoms: • Bradycardia • Hypotension • Constipation • Constricted pupils • Flaccidity • Respiratory arrest, need ambu bag • Decreased core body temp Then ask yourself, “Are they talking about overdose or withdrawal?” Overdose/Intoxication Withdrawal “I have too much…” “I don’t have enough..” Too much upper: Everything is UP Too little upper: Everything is DOWN Too much downer Everything is DOWN Too little downer: Everything is UP Drug Addiction in the Newborn Always assume intoxication (first 24 hours after birth), then after this time, assume withdrawal Alcohol Withdrawal Syndrome vs. Delirium Tremens 1. Differences: a. Every alcoholic goes through alcohol withdrawal syndrome (AWS) (after 24 hours), always precedes delirium tremens. b. Only a minority get delirium tremors (DT) AWS DT’s BOTH Semi-private-anywhere Private-near nurses station Anti-hypertensives Regular diet Clear liquids or NPO Tranquilizer Up Ad Lib (no activity restriction) Restricted bedrest (no bathroom privileges) B1 multi-vitamin (to prevent Wenicke Korsakoff) Do not restrain Should be restrained (2 pt leather restraints) 2 extremity restricted—arm on one side and leg on one, one upper extremity and one opposite lower extremity c. AWS is not life threatening. DT’s can kill you. d. Patients with AWS are not dangerous to themselves or others. Patients with DTs are dangerous to self and others. Get antihypertensive and tranquilizer because everything goes up since they are withdrawing. Top 10 Drugs tested: Psych drugs, Insulins, Anticoagulants, Digitalis, Aminoglycosides, Steroids, CCB, BB, Pain Meds, OB drugs AMINOGLYCOSIDES 1. Think “A mean old mycin” 2. Powerful antibiotics—to treat severe, life-threatening, resistant infections, gram negative 3. All aminoglycosides end in ‘mycin’, but not all drugs that end in mycin are aminoglycosides. For example.. a. Azithromycin, clarithromycin, erythromycin thromycin NOT 4. Examples of aminoglycosides: Streptomycin, Cleomycin, Tobramycin, Gentamicin, Vancomycin, Clindamycin 5. Toxic Effects: a. The most famous feature of the worlds most famous mouse (ears) i. Toxic effect: ototoxicity ii. Must monitor hearing, balance, tinnitus b. The human ear is shaped like a kidney i. Toxic effect: nephrotoxicity ii. Monitor: creatinine 1. Best indicator of kidney function 2. 0.6-1.2 mg/dL c. The number 8 drawn inside the ear reminds you of: i. Cranial nerve 8 (Drug toxic to) ii. Frequency of administration: Every 8 hours 6. Route of Administration a. Give IM or IV b. Do not give PO (not absorbed) except in these two cases: i. Hepatic encephalopathy 1. Also called Liver Coma, Ammonia-Induced Encephalopathy 2. When want a sterile bowel 3. Due to a high ammonia level, goal is to get ammonia down. ii. Pre-op Bowel surgery 1. REMEMBER this military sound off: a. NEOmycin b. KANmycin c. WHO CAN STERILIZE MY BOWEL? NEO KAN d. ^ PO, 2 bowel sterilizers 7. Trough and Peak Levels a. Reason for drawing TAP (trough, administer, peak) levels: narrow therapeutic range (small window of what works and what kills) b. Time table: ROUTE TROUGH (lowest) PEAK (highest) Sublingual 30 min before next dose 5-10 mins after drug dissolve IV 30 min before next dose 15-30 min after drug finished IM 30 min before next dose 30-60 min after drug given SQ 30 min before next dose See diabetes lecture PO 30 min before next dose Forget about it. BIOTERRORISM 1. Categories of Biological Agents a. Category A (Most serious) i. Small pox ii. Tularemia iii. Anthrax iv. Plague v. Hemorrhagic fever [Ebola] vi. Botolism b. Category B i. All others. A long list. c. Category C i. Hanta virus ii. Nipeh virus 2. Category A Biological Agents a. Smallpox i. Inhaled transmission/on Airborne Precautions ii. Dies from septicemia. Blood infection. *only class A that dies from this. iii. Rash starts around mouth first (early ID & isolation is crucial to contain) b. Tularemia i. Inhaled ii. Chest symptoms (coughing, chest pain, sputum) iii. Dies from respiratory failure iv. Treat with Streptomycin (watch hearing and creatinine) c. Anthrax i. Spread by inhalation ii. Looks like flu (chest symptoms and achy muscles) iii. Dies from respiratory failure iv. Treat with Cipro, PCN, and streptoycin d. Plague i. Spread by inhalation ii. Has the 3 H’s: 1. Hemoptysis (coughing up blood) 2. Hematemesis (vomiting blood) 3. Hematochezia (bloody diarrhea) iii. Dies from respiratory failure and DIC iv. Treat with Doxycycline and Mycins v. No longer communicable after 24 hours of treatment e. Hemorrhagic Fever [Ebola] i. 21 day time frame ii. Primary symptoms are petechair and ecchymosis iii. High % fatal iv. Die of DIC f. Botolism i. Ingested (drink/eat) ii. Has 3 major symptoms: 1. Descending paralysis (starts at head-goes down to diaphragm) 2. Fever 3. But is alert iii. Dies from respiratory failure 3. Chemical Agents a. Mustard Gas Blisters (Vesicant, eventually cover airway) b. Cyanide Respiratory arrest. Treat with Sodium Thiosulfate IV c. Phosgine chloride Choking d. Sarin Nerve agent. i. Symptoms (Cholinergic Effects) 1. Bronchorrhea 2. Bronchoconstriction 3. Salivation 4. Lacrimating 5. Urination 6. Diaphoresis/diarrhea 7. GI upset 8. Emesis 4. All chemical agents require only soap and water cleansing except for Sarin, which requires a bleach a. Nursing Actions: Bioterrorism- Isolation, Antibiotics b. Chemical: Decontamination i. Send all suspected cases to decontamination center ii. Remove all clothing iii. Chemical hazard double bag iv. Incinerated v. Shower in soap and water (bleach- sarin) vi. Discharged in government clothes CALCIUM CHANNEL BLOCKERS Note: They are like Valium for your heart. When you want to rest your heart 1. Calcium Channel Blockers: Negative [ ino, chrono, dromo ] cardiac depressant Dig is only drug that mixes + & - effects; other 99% either have + or - ACTION DEFINITION POSITIVE NEGATIVE Inotropic Strength of heartbeat Strong Weak Chronotropic Rate of heartbeat Fast Slow Dromotropic Conductivity Excitable Blocks/Slows conduction 2. What do Calcium Channel Blockers treat? (Indications) a. Antihypertensives (BP way UP-relaxes blood vessels) b. Antianginal (relaxes- reduces O2 demand) decreasing oxygen demand, relaxes heart c. Anti Atrial Arrhythmia (does not tx ventricular arrhythmias) supraventricular arrhythmia 3. Side Effects(): a. Headache (vasodilation in brain=migraine) b. Hypotension (relaxes heart c. Bradycardia 4. Names of Calcium Channel Blockers a. –soptin (Verapamil) b. –zem (Cardizem – continuous IV drip) c. –dipine 5. Nursing Actions: before administrating – BP systolic lower than 100..if < 100 hold and call Dr. Slow it down (titrate down), and measure again CARDIAC ARRYTHMIAS 1. Terminology a. “QRS depolarization” always refer to ventricular (not atrial, junctional, or nodal) b. “P wave” refers to atrial c. Know normal sinus rhythms (P wave evenly spaced) 2. Six rhythms tested on NCLEX a. Asystole (flat line) i. A lack of QRS depolarization’s (a straight line) b. Atrial flutter i. Rapid P-wave depolarization’s in a saw-tooth (flutter) c. Atrial fibrillation i. Chaotic P-wave depolarization’s (lacks any discernable pattern) d. Ventricular fibrillation (squiggly line, no pattern) i. Chaotic QRS depolarization’s (squiggly line) e. Ventricular tachycardia (sharp peaks and jagged, pattern) i. Wide, bizarre QRS’s ii. Tachy is always discernable repeating pattern f. Premature ventricular contractions (PVC) i. Periodic wide, bizarre QRS’s ii. Generally low to moderate priority. unless everyone else has a normal rhythm iii. Be concerned, if: 1. More than 6 per minute 2. 6 in a row 3. PVC falls of T-wave of previous beat 3. Lethal arrhythmias a. Asystole b. V-fib 4. Potentially life threatening arrhythmia: V-tach a. Pulseless v-tach; same as asystole and v. fib and would depend on how long down b. After 8 mins consider dead 5. Treatment a. PVC’s i. Lidocaine (Ventricular, lasts longer), Amiodorone b. V Tach i. Lidocaine c. Supraventricular arrhythmias i. Adenosine (push fast IV push; usually 8s or faster) ii. Beta-Blockers (-lol) iii. Calcium Channel Blockers iv. Digoxin (Digitalis) Lanocin d. V-Fib i. Best treatment electrically ii. Shock = 200 Defibrillate e. Asystole i. Epinephrine ii. Atropine iii. S/E anticholinergics CHEST TUBES The purpose for chest tubes is to re-establish negative pressure in the pleural space 1. In a pneumothorax, the best tube removes air 2. In a hemothorax, the chest tube removes blood 3. In a pnemohemothorax, the chest tube removes air and blood Location of chest tubes: 1. Apicals (HIGH) for Air a. Label “A”- up high 2. Basilar (LOW) for Blood a. Label “B”- placed at base; bottom of lung Examples 1. How many chest tubes (and where) for unilateral pneumohemothorax? a. 2; apical and basilar all on same side 2. How many chest tubes (and where) for bilateral pneumothorax? a. 2; apical right and left 3. How many chest tubes (and where) for post-op chest surgery? a. 2; apical and basilar unilateral b. Exception: If surgery total pneymonectomy then no chest tube bc no pleural space c. Always assume chest trauma and surgery is unilateral Problem Solving 1. What do you do if you kick over the collection bottle? a. Not a big deal; can just sit it right back up; have take a couple deep breaths 2. What do you do if the water seal breaks? a. This is more serious, because it is allowing air in creating a 2 way b. First: Clamp chest tube (Better no way than 2 way for brief period of time) **in routine care never clamp chest tube!! c. Best: Submerge i. Cut tube away (down) by device; submerge under water preferably sterile-then unclamp 3. What do you do if the chest tube comes out? a. First: cover hole with gloved hand; Vaseline gauze dressing; 4 sided sterile dressing; tape b. Best: Vaseline gauze 4. Bubbling a. Ask yourself two questions: i. WHEN is it bubbling ii. WHERE is it bubbling 5. Rules for clamping the tube: a. Never clamp for longer than 15 seconds without a Dr.’s order b. Use rubber tipped double clamp CONGENITAL HEART DEFECTS Every congenital heart defect is either TROUBLE or NO TROUBLE T R o u B L e R-L Blood shunts, B Cyanotic, T All CHD’s beginning with “T” are trouble Exception Left ventricular hyperplasic syndrome Examples of “Trouble” Examples of “No Trouble” • Tricuspid • Tricuspid arterioles • Tetralogy of Fallot • Ventricular septal defect • Patent foramen ovale • Patent ductus arteriosis • Pulmonary All CHD kids have two things whether trouble or not: 1. Murmur, because of shunt of blood 2. All get echocardiogram done (@ least 1) Four defects present in Tetralogy of Fallot: 1. VarieD Ventricular Defect 2. PictureS Pulmonic Stenosis 3. Of A Overriding Aorta 4. RancH Right Hypertrophy CRUTCHES, CANES, & WALKERS 1. How to measure: 2-3 finger widths below anterior anxillary fold to a point lateral to and slightly in front of foot 2. When the handgrip is properly placed, the angle of elbow flexion will be 30 degrees 3. Types of gaits: a. 2-Point Gait i. Step One: Move one crutch and opposite foot together ii. Step Two: Move other crutch and other foot together iii. Remember: 2 points together for a 2 point gait iv. Examples: one knee replacement b. 3-Point Gait i. Step One: Move two crutches and bad leg together ii. Step Two: move good foot by self iii. Remember: 3 point is called 3 point because three points touch down at once iv. Examples: Stairs c. 4-Point Gait i. Step One: One crutch ii. Step Two: Opposite foot iii. Step Three: Other Crutch iv. Step Four: Other food v. Examples: total both knee right after surgery d. Swing-through: for two braced extremities i. Examples: arthritis braced legs 4. When to use each gait a. Use the even numbered gaits (2&4 point) when weakness is evenly distributed (bilateral). Two point for mild problem; four-point for severe problem b. Use the odd numbered gait (3 point) when one leg is odd (unilateral problem) 5. Stairs: which foot leads when going up and down stairs on crutches? a. Remember: UP with the good; DOWN with the bad b. The crutches always move with the bad leg 6. Cane a. Hold can on the strong (unaffected) side b. Advance cane with the weak side for a wide base of support 7. Walkers a. Pick it up, set it down, walk to it b. Tie belongings to side of walker, not front c. Getting out of chair to walker- always push, never pull (same for cane, crutches) DELUSIONS, HALLUCINATIONS, & ILLUSIONS 1. Psychotic vs Non-Psychotic a. A non-psychotic person has insight & is reality based b. A psychotic person has NO insight and is NOT reality based 2. Delusions a. Definition: a delusion is a false, fixed belief or idea or thought. There is no sensory component. b. Three types of delusions: i. Paranoid or Persecutory: false, fixed belief that people are out to harm you. ii. Grandiose: False, fixed belief that you are superior iii. Somatic: False, fixed belief about parts of your body 3. Hallucinations a. Definition: a hallucination is a false, fixed sensory experience b. Five types of hallucinations: i. Auditory (most common* hearing) ii. Visual iii. Tactile iv. Olfactory v. Gustatory 4. Illusions a. Definition: An illusion is a misinterpretation of reality. It is a sensory experience. b. Differentiation between illusions & hallucinations: with illusions there is a referent in reality 5. When dealing with a patient experiencing delusions, hallucinations or illusions, first ask yourself, “What is their problem?” a. Functional Psychosis b. Psychosis of Dementia c. Psychotic Delirium 6. Functional Psychosis a. These are: i. Schizophrenia ii. Schizoaffective Disorder iii. Major Depression iv. Mania b. Patient has the potential to learn reality c. Four steps: i. Acknowledge how they feel ii. Present reality iii. Set a limit iv. Enforce the limit ::::::::::::::::::::::::::::::::::::::::CONTENT CONTINUED IN THE ATTACHMENT::::::::::::::::::::::::::::::::::::::::::::::::::: [Show More]
Last updated: 1 year ago
Preview 1 out of 74 pages
Reviews( 0 )
Document information
Connected school, study & course
About the document
Uploaded On
Feb 02, 2021
Number of pages
74
Written in

Additional information
This document has been written for:
Uploaded
Feb 02, 2021
Downloads
0
Views
186