*NURSING > STUDY GUIDE > College of New Rochelle - NURSING 328Chapter 7 Lowdermilk (All)
College of New Rochelle - NURSING 328Chapter 7 Lowdermilk
Document Content and Description Below
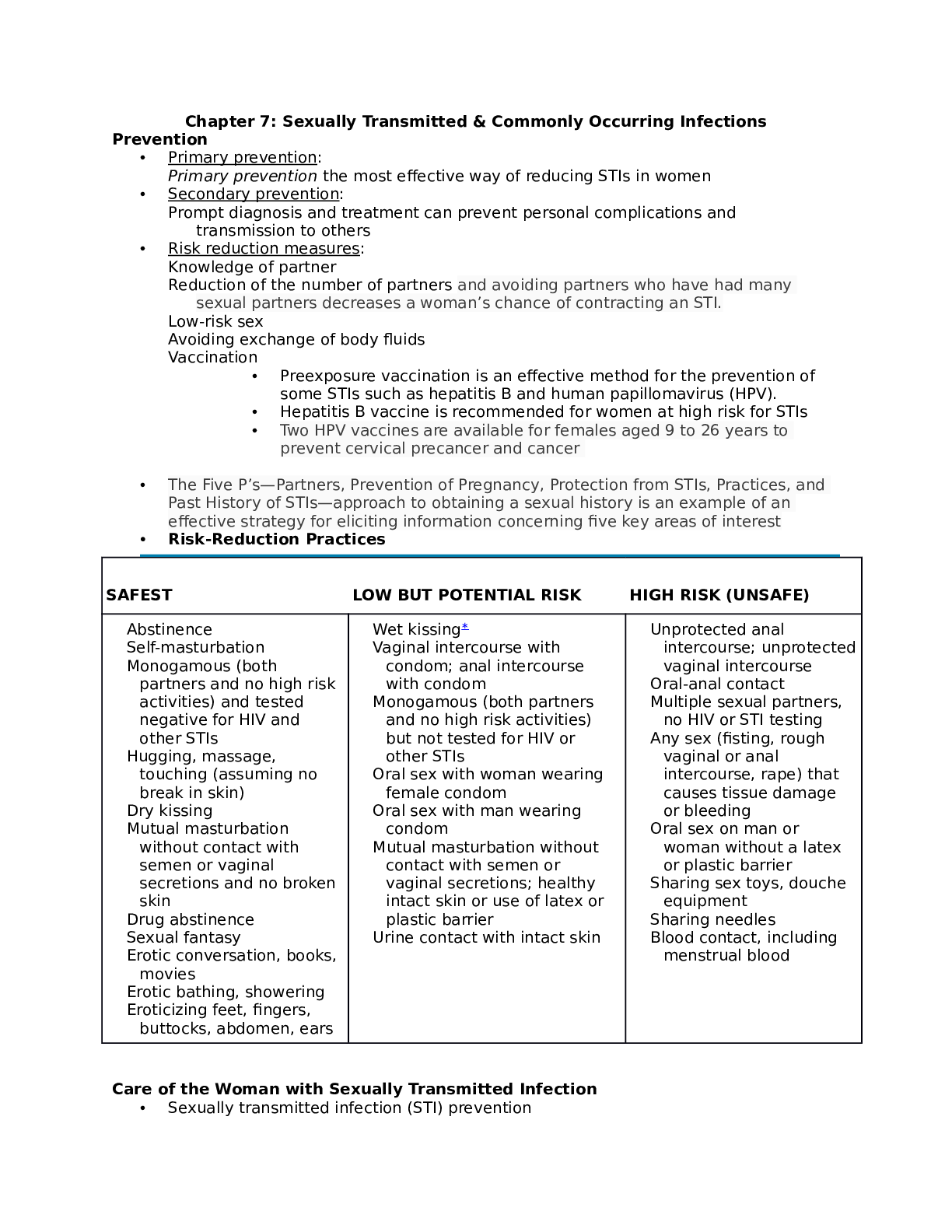
Chapter 7: Sexually Transmitted & Commonly Occurring Infections Prevention • Primary prevention: Primary prevention the most effective way of reducing STIs in women • Secondary prevention: Pr... ompt diagnosis and treatment can prevent personal complications and transmission to others • Risk reduction measures: Knowledge of partner Reduction of the number of partners and avoiding partners who have had many sexual partners decreases a woman’s chance of contracting an STI. Low-risk sex Avoiding exchange of body fluids Vaccination • Preexposure vaccination is an effective method for the prevention of some STIs such as hepatitis B and human papillomavirus (HPV). • Hepatitis B vaccine is recommended for women at high risk for STIs • Two HPV vaccines are available for females aged 9 to 26 years to prevent cervical precancer and cancer • The Five P’s—Partners, Prevention of Pregnancy, Protection from STIs, Practices, and Past History of STIs—approach to obtaining a sexual history is an example of an effective strategy for eliciting information concerning five key areas of interest • Risk-Reduction Practices SAFEST LOW BUT POTENTIAL RISK HIGH RISK (UNSAFE) Abstinence Self-masturbation Monogamous (both partners and no high risk activities) and tested negative for HIV and other STIs Hugging, massage, touching (assuming no break in skin) Dry kissing Mutual masturbation without contact with semen or vaginal secretions and no broken skin Drug abstinence Sexual fantasy Erotic conversation, books, movies Erotic bathing, showering Eroticizing feet, fingers, buttocks, abdomen, ears Wet kissing∗ Vaginal intercourse with condom; anal intercourse with condom Monogamous (both partners and no high risk activities) but not tested for HIV or other STIs Oral sex with woman wearing female condom Oral sex with man wearing condom Mutual masturbation without contact with semen or vaginal secretions; healthy intact skin or use of latex or plastic barrier Urine contact with intact skin Unprotected anal intercourse; unprotected vaginal intercourse Oral-anal contact Multiple sexual partners, no HIV or STI testing Any sex (fisting, rough vaginal or anal intercourse, rape) that causes tissue damage or bleeding Oral sex on man or woman without a latex or plastic barrier Sharing sex toys, douche equipment Sharing needles Blood contact, including menstrual blood Care of the Woman with Sexually Transmitted Infection • Sexually transmitted infection (STI) preventionPrevention and control based on Education, counseling on safer sexual behavior Identification Effective diagnosis and treatment Evaluation, treatment counseling, education for sex partners • Lowest risk – abstain from sexual intercourse • Monogamous relationship with partner Testing prior to sexual activity Bacterial Sexually Transmitted Infections • Chlamydia trachomatis Most common and fastest spreading STI Infections often silent and highly destructive Difficult to diagnose Sexually active women ages 15 to 24 years have the highest rates of infection, with women ages 18 to 20 years having the highest rates in that age group (CDC, 2012e). • Early identification of C. trachomatis is important because untreated infection often leads to acute salpingitis or pelvic inflammatory disease. Pelvic inflammatory disease (PID) is the most serious complication of chlamydial infections, and past chlamydial infections are associated with an increased risk of ectopic pregnancy and tubal factor infertility. • chlamydial infection of the cervix causes inflammation, resulting in microscopic cervical ulcerations, and thus may increase the risk of acquiring HIV infection • develop conjunctivitis or pneumonia after perinatal exposure to the mother’s infected cervix. • infectious cause of ophthalmia neonatorum Screening and diagnosis Asymptomatic and pregnant women • some women may experience spotting or postcoital bleeding, mucoid or purulent cervical discharge, or dysuria. Bleeding results from inflammation and erosion of the cervical columnar epithelium. • All pregnant women should have cervical cultures for chlamydia at the first prenatal visit. Screening late in the third trimester (36 weeks) may be carried out if the woman was positive previously, or if she is younger than 25 years, has a new sex partner, or has multiple sex partners Comparisons of diagnostic procedures • culture (expensive and labor intensive), • deoxyribonucleic acid (DNA) probe (relatively less expensive but less sensitive), • enzyme immunoassay (also relatively less expensive but less sensitive), and • nucleic acid amplification tests (NAATs) (expensive but has relatively higher sensitivity Management Doxycycline- treatment of urethral, cervical and rectal infections and Azithromycin- often prescribed when compliance may be a problem, because only one dose is needed; however, expense is a concern with this medication. Women who have a chlamydial infection and also are infected with HIV should be treated with the same regimen as those who are not infected with HIV. All exposed sexual partners should be treated. [Show More]
Last updated: 1 year ago
Preview 1 out of 18 pages
Instant download
Buy this document to get the full access instantly
Instant Download Access after purchase
Add to cartInstant download
Reviews( 0 )
Document information
Connected school, study & course
About the document
Uploaded On
Apr 12, 2021
Number of pages
18
Written in

Additional information
This document has been written for:
Uploaded
Apr 12, 2021
Downloads
0
Views
50