*NURSING > STUDY GUIDE > EXAM 2 STUDY GUIDE PATHOPHISIOLOGY – CV, Resp, Musculoskeletal (All)
EXAM 2 STUDY GUIDE PATHOPHISIOLOGY – CV, Resp, Musculoskeletal
Document Content and Description Below
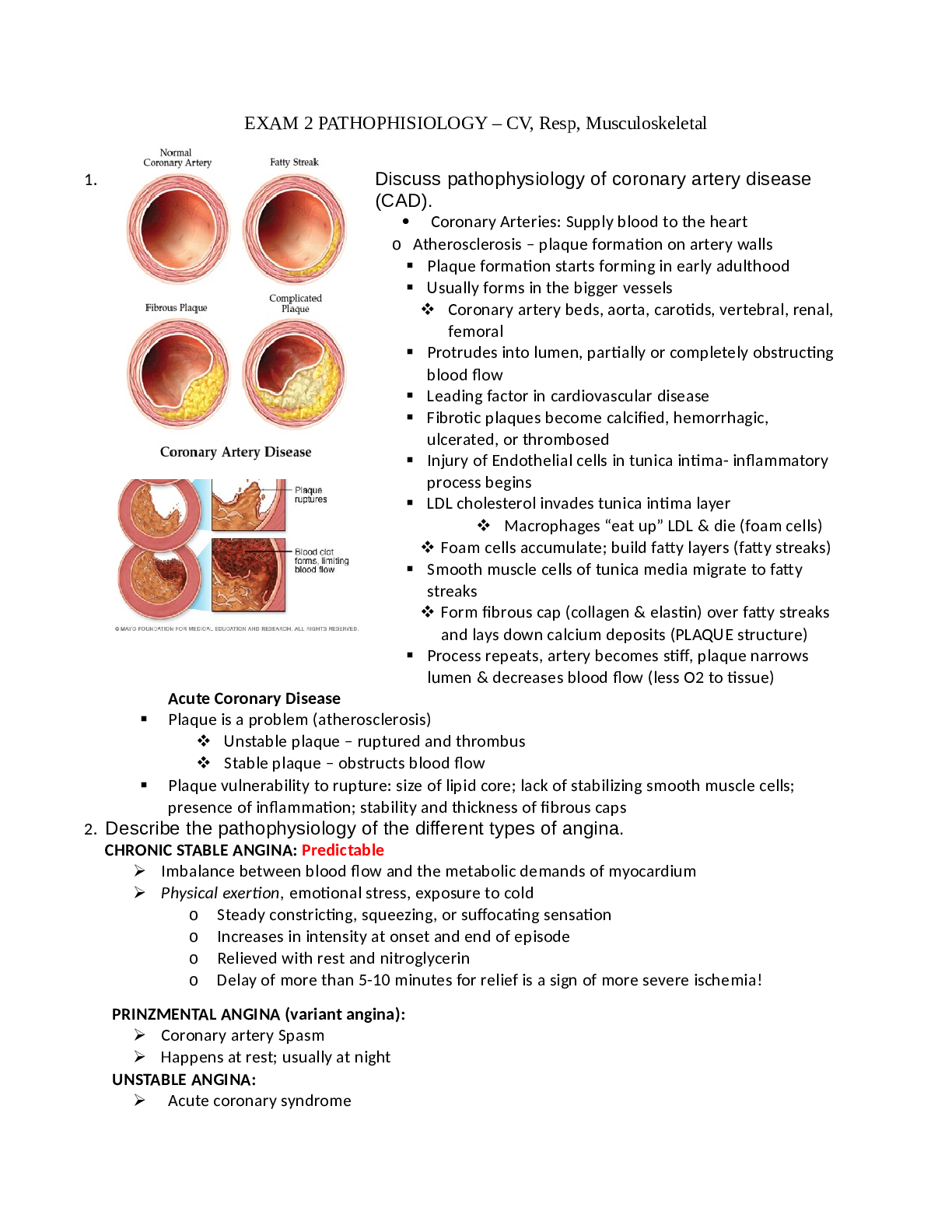
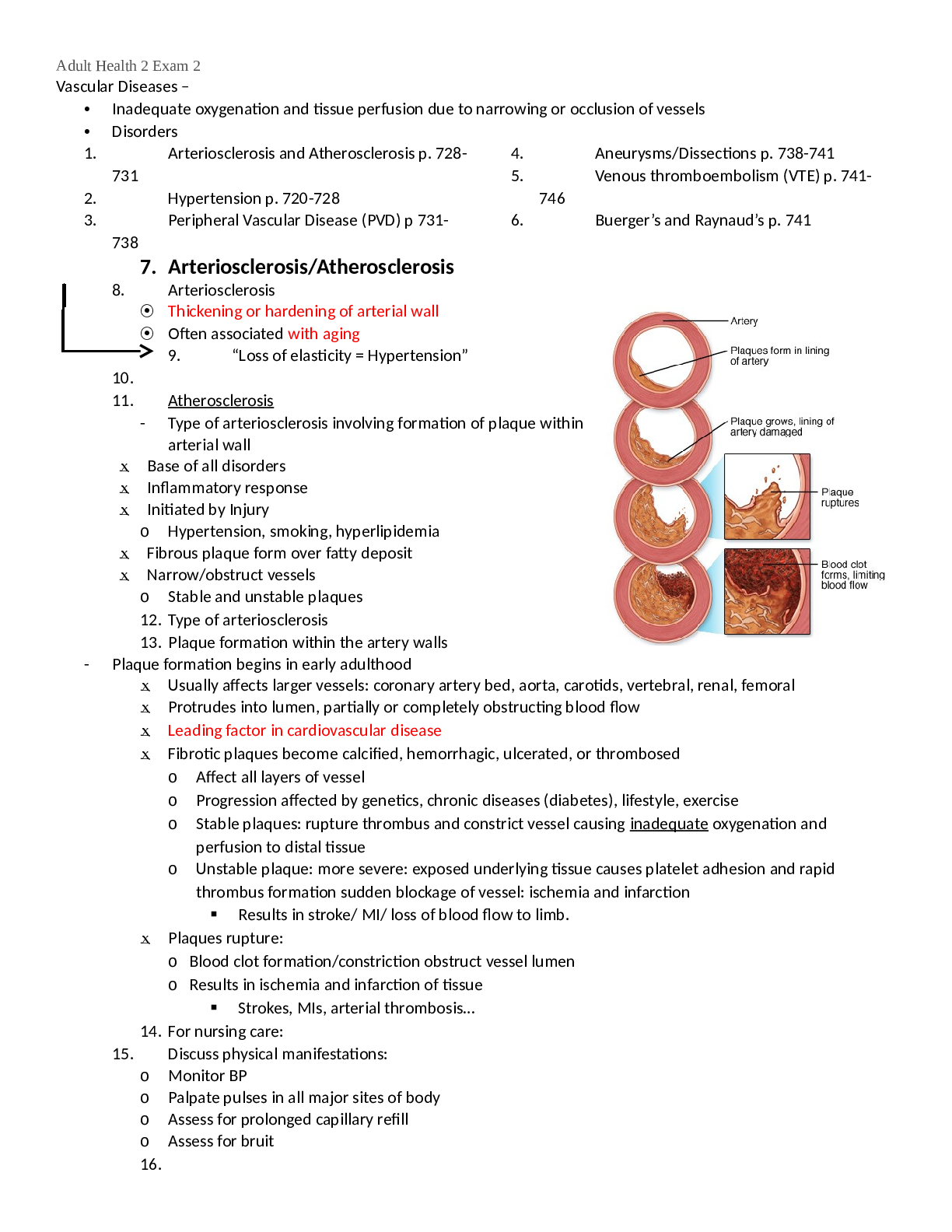
EXAM 2 PATHOPHISIOLOGY – CV, Resp, Musculoskeletal 1. Discuss pathophysiology of coronary artery disease (CAD). Coronary Arteries: Supply blood to the heart o Atherosclerosis – plaque form... ation on artery walls Plaque formation starts forming in early adulthood Usually forms in the bigger vessels Coronary artery beds, aorta, carotids, vertebral, renal, femoral Protrudes into lumen, partially or completely obstructing blood flow Leading factor in cardiovascular disease Fibrotic plaques become calcified, hemorrhagic, ulcerated, or thrombosed Injury of Endothelial cells in tunica intima- inflammatory process begins LDL cholesterol invades tunica intima layer Macrophages “eat up” LDL & die (foam cells) Foam cells accumulate; build fatty layers (fatty streaks) Smooth muscle cells of tunica media migrate to fatty streaks Form fibrous cap (collagen & elastin) over fatty streaks and lays down calcium deposits (PLAQUE structure) Process repeats, artery becomes stiff, plaque narrows lumen & decreases blood flow (less O2 to tissue) Acute Coronary Disease Plaque is a problem (atherosclerosis) Unstable plaque – ruptured and thrombus Stable plaque – obstructs blood flow Plaque vulnerability to rupture: size of lipid core; lack of stabilizing smooth muscle cells; presence of inflammation; stability and thickness of fibrous caps 2. Describe the pathophysiology of the different types of angina. CHRONIC STABLE ANGINA: Predictable Imbalance between blood flow and the metabolic demands of myocardium Physical exertion, emotional stress, exposure to cold o Steady constricting, squeezing, or suffocating sensation o Increases in intensity at onset and end of episode o Relieved with rest and nitroglycerin o Delay of more than 5-10 minutes for relief is a sign of more severe ischemia! PRINZMENTAL ANGINA (variant angina): Coronary artery Spasm Happens at rest; usually at night UNSTABLE ANGINA: Acute coronary syndrome May occur more frequently, occur more easily at rest, feel more severe, or last longer 3. Compare acute and chronic coronary syndromes. Unstable Angina • Ischemia (lack of blood flow) to cause symptoms, no signs of heart damage (Can also occur at rest) Non-ST-Elevation Myocardial Infarction (NSTEMI) • Ischemia severe to cause symptoms and raise cardiac markers (labs) ST-Elevation Myocardial Infarction (STEMI) • Ischemia severe to cause symptoms, raise cardiac markers (labs), and result in EKG changes (ST-elevation) • Necrosis of myocardial tissue 4. D escribe the pathophysiology of the pericardial disorders. - Acute Pericarditis Pericardial inflammation lasting less than 2 weeks o Inflammatory response Causes: viral (majority), bacterial (Rheumatic fever), connective tissue diseases, post-MI, post cardiac surgery, neoplasms Clinical manifestations: chest pain (worse with inspiration and coughing; decreases when sitting up and leaning forward); ausculatory pericardial friction rub (leathery sound); EKG changes; fever Disease severity varies self-limiting to death o Complications: pericardial effusion and cardiac tamponade - Pericardial Effusion Pericardial inflammation lasting less than 2 weeks Inflammatory response Causes: viral (majority), bacterial (Rheumatic fever), connective tissue diseases, post-MI, post cardiac surgery, neoplasms Clinical manifestations: chest pain (worse with inspiration and coughing; decreases when sitting up and leaning forward); ausculatory pericardial friction rub (leathery sound); EKG changes; fever Disease severity varies self-limiting to death Complications: pericardial effusion and cardiac tamponade 5. Explain the pathophysiology of different types of valvular disorders. *Function of the heart valves are meant to promote unidirectional flow of blood through the chambers of the heart Valvular Heart Disease – dysfunction that can result from: Congenital defects Trauma Ischemia Degenerative Inflammation Stenosis RegurgitationoNarrowing of valve orifice oDoes not OPEN properly oNot enough blood flows through the valve Mitral Valve Stenosis Caused by Rheumatic fever Impair filling of left ventricle Leads to blood pooling in left atrium and thrombus formation o Distortion of valve o Does not CLOSE properly o Blood flows backwards Mitral Valve Regurgitation and Prolapse Blood leaks back into left atrium Leads to impairment of left ventricle, ↑ in atrial pressure, and pulmonary congestion Mitral Valve Prolapse: floppy mitral valve – balloons back into left atrium during systole With and without regurgitation [Show More]
Last updated: 1 year ago
Preview 1 out of 40 pages
Reviews( 0 )
Document information
Connected school, study & course
About the document
Uploaded On
Aug 14, 2021
Number of pages
40
Written in

Additional information
This document has been written for:
Uploaded
Aug 14, 2021
Downloads
0
Views
36
.png)

.png)

.png)