*NURSING > QUESTIONS and ANSWERS > Pediatric ATI Practice Exams, quizzes, finals | (All you need to pass the exams) | Download To Score (All)
Pediatric ATI Practice Exams, quizzes, finals | (All you need to pass the exams) | Download To Score An A
Document Content and Description Below
Pediatric ATI Practice Exams, quizzes, finals ❖ Abstraction- abstract thought demonstrated by the ability to draw a conclusion from various pieces of information. ❖ Abuse and neglect- Crosses ... all ethnic backgrounds. Parents might say, “this child is very different from my other children”. This warrants further clarification. A child that has several unexplained scars and bruises, indicates additional assessment is needed. Dark urine indicates a complication from burns. Children will have an underweight appearance, ringed appearing nails. o A nurse in an ED is caring for an adolescent who reports painful urination. Behaviors that suggest possible child maltreatment? Uses mood-elevating substances. A charge nurse in an ED is preparing an in-service for a group of newly licensed nurses on the clinical manifestations of child maltreatment. Which of the following clinical manifestations should the charge nurse include as suggestive of potential physical abuse? Symmetric burns of the lower extremities. A nurse is evaluating a toddler and the family dynamics of the child's family, in which abuse is suspected. What behavior is expected? The child cringes when approached. The child has unexplained healed injuries. The child lies still while surveying the environment. A nurse is admitting a toddler brought to the hospital for circumferential burns. The history given and burn markings do not correlate, therefore, child abuse is suspected. Which of the following should the nurse consider the most important to include in the documentation? A description of the burns. A community health nurse is assessing an 18-month-old toddler in a community day care. Which findings should the nurse identify as a potential indication of physical neglect? Poor personal hygiene. ❖ Acrocyanosis- crying can cause cyanosis in full term babies, appear transient, and have a blue color to hands & feet after birth. ❖ Airway obstruction- to check for obstruction the parent’s should push on the child’s abdomen to assess, listen over the child’s mouth for sounds of breathing, and will use 1 finger to check in the child’s mouth for objects. ❖ Ambiguous genitalia- prepare the child for surgery, obtain a detailed family history, refer the family for genetic counseling, explain the need for a chromosomal analysis. ❖ Anaphylactic reaction- reaction S/S are urticaria, rash, angioedema, and wheezing. A school nurse is assisting a child who has been stung by a bee. The child's hand is swelling and the nurse notes that the child has allergies to insect stings. Which of the following manifestations should the nurse recognize with anaphylaxis? Nausea, urticarial, stridor. A nurse is teaching the parent of an infant about food allergens. Which of the following foods should the nurse include as being the most common food allergy in children? Cow's milk. A nurse is performing an assessment on a child at the clinic. When performing this assessment, the nurse should? have the child sit in the parent's lap, auscultate the heart and lungs, and the examine the ears and throat. ❖ Apgar score- crying vigorously (2), limbs flexed (2), heart rate 120 (2), trunk pink (2), hands and feet are cyanotic (1)= score of 9. ❖ Appendectomy- encourage semi-fowler’s position after procedure. ❖ Appendicitis- A nurse in the ED is caring for an adolescent who has severe abdominal pain due to appendicitis. Which of the following locations should the nurse identify as McBurney's point? (Hotspot) the lower R. quadrant of the abdomen between the umbilicus and the anterior iliac crest. A nurse in an emergency department is caring for a school-age child who has appendicitis and rates his abdominal pain at 7 on a 0 to 10 scale. Which of the following actions should the nurse take? Give morphine 0.05mg/kg IV. A nurse is assessing a school-age child who has appendicitis with possible perforation. The nurse should identify which of the following as a manifestation of peritonitis? abdominal distention. Appendix- when assessing a school-age child immediately postop following a perforated appendix repair Absence of peristalsis, is an expected finding. Semi-fowler’s for appendectomy. ❖ Asthma- risk factors are family history of asthma or allergies, exposure to smoke, and low birth weight. Indications of deterioration are wheezing, retraction of sternal muscles, and nasal flaring. Albuterol is used as needed before exercise and to treat acute asthma attacks. For these children it is important to monitor oxygen saturation, place the child in an upright position, and administer Bronchodilator’s. Peak Flow Meter- zero the meter before each use, perform and document 3 attempts, and use the best attempt as the baseline. o A nurse is auscultating the lungs of an adolescent who has asthma. The nurse should identify the sound as which of the following? Tachypnea. A nurse is providing discharge teaching to the parent of a school-age child who has moderate persistent asthma. Which of the following instructions should the nurse include? "Pulmonary function tests will be performed every 12-24 months to evaluate how your child is responding to therapy." A nurse is providing teaching to the parent of a preschooler about ways to prevent acute asthma attacks. Which of the following statements by the parent should the nurse identify as understanding the teaching? "I should keep my child indoors when I mow the yard.” A nurse is teaching an adolescent who has asthma about how to use a peak expiratory flow meter (PEFM). Which of the following responses by the adolescent indicates an understanding of the teaching? I will record the highest reading of three attempts. A nurse in an emergency department is assessing a school-age child who is experiencing an acute asthma exacerbation. Which of the following findings is the priority for the nurse to report to the provider? Sudden decrease in wheezing. A nurse is caring for a toddler who has asthma. The parents are concerned about the toddler's reaction to the hospitalization. Which of the following nursing actions should the nurse perform to decrease the stress experienced by the toddler? Encourage rooming-in. ❖ Attention deficit hyperactivity disorder (ADHD)- may be caused by prenatal exposure to alcohol, history of head trauma. Child will exhibit inappropriate behaviors. Integrate learning into movement activities, sit the child in front of the room to help focus their attention and reduce the distraction from other activities, provide verbal and written instructions regarding homework assignments, use consistent class rules, schedule exams in a room that provides privacy and minimal stimulation, and give these children regular breaks. ❖ Authoritarian-“My son better do as I say!” ❖ Authoritative- sets rules, and explains the reason behind them, fair parenting. ❖ Autism- if admitted to a hospital, adjust environment by ensuring that staff visits are kept short ❖ Bacterial endocarditis- A nurse is caring for a child with bacterial endocarditis. The child will receive long-term antibiotics and will require a peripherally inserted central catheter. Which of the following statements would be appropriate for the nurse to state to the child’s parent? The PICC line will last several weeks with proper care. ❖ Biliary atresia- yellow sclera, abdominal distention, dark urine. ❖ Bites- prevent insect bites by avoiding areas of tall grass, wear insect repellent, check house pets frequently. ❖ Bone marrow aspiration- A nurse is caring for a child who is undergoing a bone marrow aspiration. Which response indicates to the nurse that the teaching has been effective? I'll have to lie on my belly while it's done. A nurse is teaching a school-age child who is to undergo a bone marrow aspiration. Which of the following statements should the nurse make? I will place a pressure dressing over the areas following the procedure. ❖ Bronchiolitis- administer humidified oxygen, suction the nasopharynx as needed. o A nurse is caring for a child with bronchiolitis. Assessment findings indicate wheezing, oxygen saturation of 100%, respiratory rate of 40/min, and a heart rate of 92/min. The child is receiving oxygen at 2 LPM. An order is written to wean oxygen maintaining oxygen saturation 95% or greater. Which of the following actions is most appropriate for the nurse to take? Lower oxygen to 1 L/min, check the oxygen sat, and reassess the child. ❖ Burns- Antimicrobial ointment is used to prevent infection. Nurse should administer tetanus toxoid if it has been more than 5 years since the prior dose. A clean-dry dressing of fine mesh gauze & a light gauze dressing should be applied that restricts movement to prevent injury to wound. Ice impairs circulation & increase tissue damage. Administer Morphine Sulfate IV via continuous infusion for severe pain. Grafts- infection indicated by unstable body temperatures, subeschar hemorrhage, change in skin color around affected area. o A nurse is creating an educational plan to teach parents about protecting their children from sunburns. Instructions to be included? "Choose a waterproof sunscreen with an SPF of at least 15." A nurse is caring for a preschooler who is scheduled for hydrotherapy treatment for wound debridement following a burn injury. Appropriate action to take prior to the procedure? Administer an analgesic to the child. o 1st degree= Superficial minor burn- damage to epidermis. Appearance is pink to red in color, no blisters, and blanches with pressure. Painful, heals in 3-7 days, no scarring. ▪ A nurse in the emergency department is caring for a school age child who has sustained a superficial minor burn from fireworks on his forearm. which of the following actions should the nurse take? use an antimicrobial ointment on the affected area. o 2nd degree= Superficial partial thickness burn- apply cool, wet compresses to the affected areas. Moderate burns mean initiating a high protein, high calorie diet. Damages the entire epidermis, and not the dermis. Appearance is painful,. Moist, red in color with blisters, mild to moderate edema, and no eschar. Blanches with pressure. Heals in less than 21 days, various scarring, sensitive to temperature changes, exposure to air, and light touch. Minor is less than 10% of TBSA. Moderate is 10%- 20% of TBSA. Severe is greater than 25% of TBSA. Deep partial-thickness burns- damage to the entire epidermis, some parts of the dermis, sweat glands and hair follicles intact. Appearance is mottled, red-white, blisters, moderate edema. Blanches with pressure. Painful, sensitive to temps, and light touch. Healing time can extend beyond 21 days, scarring is likely. ▪ A nurse in the ED is caring for a toddler who has partial-thickness burns on his right arm. Which action should the nurse take? Cleanse the affected area with mild soap and water. A nurse is caring for a child who adheres to a vegetarian diet, and has sustained superficial partial-thickness burns. The nurse would recommend which of the following food choices as having the highest protein content? ½ cup of peanut butter with apple slices. A nurse is caring for a child who has superficial partial-thickness burns over 50% of his body. In planning for the nutritional needs of the child, which of the following should to nurse recognize as an appropriate intervention? Perform dressing changes at least 1 hour before or after meals. A nurse is caring for a 4-year-old child who has superficial partial-thickness burns over 50% of his body. When planning for the nutritional needs of the child, which of the following actions should the nurse plan to take? Supplement feedings with enteral feedings. A nurse is caring for a child who is a vegetarian and has sustained superficial partial-thickness burns on her legs. Which diet choices would be appropriate for this child? Peanut butter and jelly sandwich. Deep partial-thickness burns plan of care is based on concerns related to the child's injury. 1.Impaired gas exchange. 2.Presence of pain. 3.Disturbed fluid balance. 4.Potential for infection. 5.Compromised body image. o 3rd degree= Full thickness- suspect possible septic shock with increased body temperature, altered sensorium, decreased urinary output. Damage to the entire epidermis, dermis, and possible subcutaneous tissue. Appearance is red-tan, black, brown, or waxy white. Dry and leathery. No blanching. As burn heals, painful sensations return and severity of pain increases. Heals within weekly to months. Scarring is present, and grafting is required. Minor can require 1-2 day admission. Moderate is admission to a hospital, preferably a burn clinic. Severe is admission to a burn center. ▪ A nurse is assessing the vital signs of a 10-year-old child following a burn injury. Clinical manifestation indicating early septic shock? Temp 39.1C (102.4F). To evaluate kidney function, the nurse must accurately measure the hourly urine output of a 1½-year-old toddler weighing 22 lb who has been admitted with extensive burns. What is the minimum safe output per hour for a child this age? 10-20. A nurse in an emergency department is caring for a 4-year-old child who has burns to the neck and face following a house fire. Which actions should the nurse take first? Determine the child's breathing pattern. o 4th degree= Deep partial thickness- damages all layers of the skin, extends to muscle, fascia, and bones. Appearance is variable in color, dull and dry, charring, possible visible ligaments, bones, tendons. No pain is present, heals within weeks to months, scarring is present, grafting is required, amputation may be necessary. ❖ Cardiac catherization- Site should be kept clean & dry for at least 3 days to reduce the risk for infection. Parents can remove the pressure dressing the day after the procedure and apply an adhesive bandage strip daily to the site for at least the next 2 days. Child can resume regular diet after the procedure & can attend school the following day, but strenuous activity should be avoided to prevent bleeding of the site. Check for iodine or shellfish allergy prior to the procedure. o A nurse is teaching a school-age child and his parent about postoperative care following cardiac catheterization. Which of the following instructions should the nurse include? "Wait 3 days before taking a tub bath”. A toddler undergoes cardiac catheterization as part of a diagnostic workup for pulmonic stenosis. In which part of the cardiovascular system should the nurse expect an increase in pressure? Right ventricle. A nurse is caring for a 4 month old infant who is admitted with a ventricular septal defect (VSD) and undergoing a cardiac catheterization. Post catheterization, which manifestations should alert the nurse to a potential complication? Groin dressing with small amount of blood noted. A nurse is assessing a 6-month-old infant following a cardiac catheterization. Which findings should the nurse report to the provider? BP 86/40 mm Hg. ❖ Car seats- "I should secure the car seat using lower anchors and tethers instead of the seat belt." Indicated understanding of teaching about car seat use. ❖ Casts- A toddler has just had a cast applied for a fractured wrist. The wrist and elbow are immobilized. What information should the nurse include in the home care instructions before discharge? Report swelling of fingers. Elevate casted arm when the child is standing. Fiberglass cast- A nurse is providing teaching to an adolescent who has a fiberglass are cast. Which of the following instructions should the nurse include in the teaching? Place a plastic bag over the cast when showering or bathing. A nurse is assessing an adolescent who sustained a broken tibia. Following the application of a fiberglass cast, the adolescent complains of pain and a tingling feeling in the limb. Which of the following actions should the nurse take first? Assess for manifestations of circulatory impairment or swelling. Lower leg cast- A nurse is providing discharge teaching to the parents of a Caucasian toddler who had a lower leg cast applied 24 hour ago. The nurse should instruct the parents to report which of the following findings to the provider? Restricted ability to move the toe. Plaster cast- apply moleskin to the edges of the cast. Spica cast- A nurse is teaching a mother how to care for her toddler who is in a Spica cast. In what position should the nurse suggest that the mother place the toddler during a feeding? Semi-Fowler on a padded, adjustable tilt board. ❖ Celiac disease- gluten free diet. Needs to avoid barley, bouillon cubes, wheat, rye. Fruits (canned, fresh, frozen)m corn tortillas, rice cakes, peanut butter, nuts, and plain rice are acceptable. o A nurse is assessing a pt. who has a new diagnosis of celiac disease. Expected clinical manifestations? Steatorrhea. A nurse is providing dietary teaching to the parent of a school-age child who has celiac disease. The nurse should recommend that the parent offer which of the following foods to the child? Rice pudding. The health care provider is assessing a 2-year-old child for the presence of celiac disease. For what specific signs and symptoms should the nurse be alert? Steatorrhea, distended abdomen, Iron-deficiency anemia. A nurse is providing nutritional teaching to an adolescent client who has celiac disease. Which of the following breakfast foods should the nurse recommend? Scrambled eggs. A nurse observes an adolescent with celiac disease ordering a gluten free breakfast tray. The nurse should know that the client understands the diet when the client orders which of the following items? Eggs and orange juice. ❖ Cellulitis- administer oral antibiotics. ❖ Cerebral palsy- decrease neuromuscular impairment by using manual jaw control during feedings. Baclofen & Diazepam are given to TX painful muscle spasms. The nurse will need to evaluate the toddler’s need for an evaluation of their hearing ability. o A nurse is caring for a toddler who has spastic (pyramidal) cerebral palsy. Expected clinical manifestations? Ankle clonus, exaggerated stretch reflexes, Contractures. A nurse notes that a child is exhibiting signs of cerebral palsy. At what age are these signs usually first noticeable? 12months. A nurse is caring for a child who has cerebral palsy who is scheduled for orthopedic surgery. Which of the following strategies should the nurse plan to include in the initial plan of care? Facilitate communication with the child by their usual means. A nurse is educating the parent of a 9-month-old infant who has recently been diagnosed with cerebral palsy. Which of the following statements by the parent should indicate to the nurse that teaching has been effective? "I am hopeful that the early schooling will increase my child's ability for self-care." The nurse is assessing a 6 month old infant in the well child clinic. Which of the following assessments would indicate the infant needs further evaluation? legs stay crossed at the knees. A nurse is teaching the parents of a child who has cerebral palsy. Which of the following statements should the nurse make? Your child will need a botulinum toxin A injection to help with muscle spasticity. ❖ Cheiloplasty- Providing discharge teaching to the parents of a 3-month-old infant following Cheiloplasty. Appropriate instructions? Apply a thin layer of antibiotic ointment on baby's suture line daily for the next 3 days. ❖ Chemo- HGB that is below the expected reference range for a 6-year-old, this puts the child at risk for anemia d/t chemotherapy effects on the blood forming cells of the bone marrow. Teach patient and family about the manifestations of infection, bleeding precautions, and hand hygiene. Instruct the child to use a soft sponge toothbrush when brushing her teeth. o A nurse is reviewing the laboratory report of a 6-year-old child who is receiving chemotherapy. Which laboratory values should the nurse report to the provider? HGB 8.5. A nurse is assessing a toddler who has leukemia and is receiving his first round of chemotherapy. Which of the following findings is the priority for the nurse to report to the provide? urticaria. A nurse is caring for a school-age child who is receiving chemotherapy and is severely immunocompromised. Which of the following actions should the nurse take? Screen the child's visitors for indications of infection. A nurse is caring for a 6-year-old child who is receiving chemotherapy. The child has a platelet count of 20,000/mm3. Which of the following should the nurse recognize as the appropriate intervention for a child with this platelet count? Encourage quiet play. A nurse is providing discharge teaching to the parent of a school-age child who has leukemia and is receiving chemotherapy. Which of the following statements by the parent indicates an understanding of the teaching? I will inspect my child's mouth every day for sores. A nurse is reviewing the laboratory report of a toddler who is receiving chemotherapy for leukemia. Which of the following laboratory values should the nurse report to the provider? Hgb 6 g/dL. A nurse is creating a plan of care for a child who has leukopenia secondary to chemotherapy. Which of the following interventions should the nurse include in the plan? Monitor the child for increased temperature. A nurse is caring for a child receiving chemotherapy. The white blood cell count is 1,200/mm^3. In planning the child's care, the nurse should prepare to do which of the following? Maintain protective isolation and monitor for fever. A nurse is caring for a child who is receiving chemotherapy with anorexia and nausea. Which interventions should the nurse recognize as the most appropriate for the child experiencing these symptoms? Allow the client to eat whatever the client wants, at any time. ❖ Classification- ability to organize and group objects based on characteristics. ❖ Cleft lip and palate- after surgery place the child in an upright position. o A mother asks why her 2-year-old toddler's cleft palate was not repaired at the same time that the cleft lip was repaired. What is the best response by the nurse? "The palate usually is repaired before a child starts to speak. Some surgeons prefer to wait up to 2 years." A nurse is caring for an infant following surgical repair of a cleft lip and palate. Which of the following actions should the nurse take? Suction the infant gently with a bulb syringe PRN. A nurse is caring for an 18-month-old toddler who has been admitted following surgical repair of a cleft palate. Postoperatively, the child complains of thirst. The nurse should provide fluids using which of the following? Cup. ❖ Coarctation of the aorta- weak femoral pulses, cool skin of the lower extremities, heart failure, & high BP are manifestations. ❖ Colostomy- A nurse is providing education to a parent whose child has had a colostomy. Which of the following is an appropriate method to determine understanding of teaching? Observe parents while they perform the procedure. For an infant with a colostomy, teach parent’s to apply paste to the back of the wafer on their child’s appliance. ❖ Communicable disease- obtaining immunizations as scheduled is the best way to prevent these. o Measles- presents commonly as a red rash. o Mononucleosis- common manifestations are fever, fatigue, swollen lymph nodes, sore throat, sore upper abdomen. Teach adolescent to drink plenty of fluids, avoid strenuous exercise, allow for periods of rest, take aspirin as needed for fever and discomfort, gargle with salt water every 2-3 hours, antivirals will be prescribed. A nurse is teaching a group of parents about infectious mononucleosis. Which of the following statements by a parent should the nurse identify as understanding the teaching? Mononucleosis is caused by an infection with the Epstein-Barr virus. A school nurse is assessing a child who returned to school following a case of mononucleosis. The child has a note from his primary care provider excusing him from gym class. What should the nurse recognize as the most appropriate reason for this excuse? Sustaining abdominal trauma. o Mumps- complications are orchitis, encephalitis, meningitis, oophoritis, mastitis, deafness, enlarged lymph nodes. o Pertussis- runny nose, mild fever, cough with whopping sound are common manifestations. A nurse at an urgent care clinic is assessing an adolescent client who has an upper respiratory tract infection. Which of the following findings should the nurse recognize as a manifestation of pertussis? Dry, hacking cough. A nurse is admitting a school-age child who has pertussis. Which actions should the nurse take? Initiate droplet precautions for the child. o Pneumonia- can be caused by rubeola (measles), pertussis (whooping cough), varicella (chicken pox). o Rotavirus- fever, vomiting, watery stools, foul smell are common manifestations. The nurse is reviewing the medical record of a 2-month-old infant who has rotavirus. The nurse notes a hemoglobin level of 12g/dl and a hematocrit of 51%. Which of the following statements by the nurse indicates an understanding of the laboratory values? The infant may be dehydrated. o Rubella- complications from a birth defect in the fetus of a mom infected during pregnancy. What clinical signs should lead a nurse to suspect that a 1-year-old child has rubella (German measles)? Enlarged posterior cervical & postauricular nodes. o Rubeola- A nurse is caring for a 2-year-old child who has not received any immunizations. During assessment, the child is noted to have maculopapular rash and fever. The child's parent tells the nurse that the child has been exposed to rubeola. Which of the following assessment findings should the nurse expect? Koplik spot. o Varicella- A nurse in a provider's office is caring for a school-age child who has varicella. The parent asks the nurse when her child will no longer be contagious. Appropriate response by the nurse? When your child's lesions are crusted, 6 days after they appear. A nurse is caring for a child who has a vesicular rash. The parent asks the nurse what illness can cause the rash. Which is the most appropriate response for the nurse to give? Varicella. ❖ Concussion- amnesia, bradycardia, respiratory depression, and confusion are common findings. ❖ Congenital heart disease- A 1-year-old child has a congenital cardiac malformation that causes right-to-left shunting of blood through the heart. What clinical finding should the nurse expect? Increased hematocrit. A nurse is caring for four children who have congenital heart disease. Based on the pathophysiology of the disorders, which of the following should the nurse recognize would present with cyanosis? Transposition of great vessels. ❖ Congestive heart failure- to meet nutritional needs allow 30 minutes to complete feedings, increase caloric density of formula slowly, use a soft preemie nipple or regular nipple with slit in tip, provide gavage feedings if RR exceeds 80 breaths/minute. ❖ Conjunctivitis- assess inferior surface of eye. ❖ Conservation- ability to understand that quantity does not change if the shape changes. ❖ Contact precautions- Gastroenteritis, caused by Salmonella (confusion). ❖ Creatinine is a byproduct of protein metabolism and is excreted by the body through the kidneys. An elevated creatinine level (3.0) is an indication that the kidneys are not functioning, which may indicate rejection of the kidney. ❖ Croup- A 3-year-old boy in respiratory distress is treated in the emergency department. A diagnosis of acute spasmodic laryngitis (spasmodic croup) is made. At the time of discharge, the mother asks how to handle another attack at home. What should the nurse recommend? Placing him near a cool-mist humidifier. A 30-month-old toddler is brought to the emergency department in acute respiratory distress, and a diagnosis of laryngotracheobronchitis (viral croup) is made. What is the most important equipment for the nurse to have available when the child is admitted to the pediatric unit? tracheostomy set. A nurse is caring for a toddler in acute respiratory distress precipitated by laryngotracheobronchitis. The child has a temperature of 103° F (39.4° C). What is the priority nursing intervention? Monitoring respiratory status continuously. A nurse is caring for a 3-year- old child with acute laryngotracheobronchitis. The child has severe dyspnea and a temperature of 104.0º F (40.0° C) and is receiving cool mist by way of a facemask. The mother asks why her child is not receiving warm mist. The nurse explains that cool mist: Facilitates reduction of mucosal edema. ❖ Cyanotic cardiac defect- 3 year old that cries when parents leave the room. Cyanosis and dyspnea worsen. To achieve relief place child in the knee chest position. ❖ Cystic fibrosis- mucus is thick because, Cystic Fibrosis interferes with how your glands excrete mucus. An indication of CF is a sweat chloride content of 85 mEq/L. Medications used for treatment are Tobramycin, fat-soluble vitamins, Albuterol, and Dornase Alfa. Expected findings are wheezing, clubbing of the fingers and toes, barre-shaped chest. These children need pancreatic enzymes administered with meals and snacks. o A nurse is providing dietary teaching to the parent of a school-age child who has cystic fibrosis. Appropriate statement to make? "You should offer your child high-protein meals and snacks throughout the day." A 30-month-old boy with cystic fibrosis is admitted to the pediatric unit with a severe upper respiratory infection. The toddler is small for his age. What pathological process does the nurse know is the cause of his small stature? An absence of pancreatic enzymes. A nurse is planning care for a preschooler who has cystic fibrosis. Which of the following interventions should the nurse include in the plan? Increase fat content in diet to 40% of total calories. A nurse is admitting a child who has an exacerbation of cystic fibrosis. The nurse should expect to find which of the following assessments? Oxygen saturation of 85%. A nurse is caring for a child who has cystic fibrosis. Which of the following assessments should the nurse recognize as a priority to report to the primary care provider? inability to clear secretions. A nurse is caring for a child with cystic fibrosis. In planning nutritional care for this child, the nurse should include which of the following actions? Increased protein intake. A nurse is providing dietary teaching to the parent of a child who has cystic fibrosis. Which of the following dietary recommendations should the nurse make? Increase the child's protein intake. A nurse is caring for a 2 year old child with cystic fibrosis. The nurse is planning to take the child to the playroom. Which activities would be the most appropriate for the child? building block towers. ❖ Dehydration- A nurse is providing discharge teaching to the parent of an 18-month-old toddler who has dehydration as a result of acute diarrhea. Statement by the parent that indicates and understanding of the teaching? "I will monitor my child's # of wet diapers". A nurse is reviewing the lab report of an infant who is receiving treatment for severe dehydration. The nurse should identify that which of the following lab values indicates effectiveness of the current treatment? Sodium 140 mEq/L. A nurse in an ED is assessing a 3-month-old infant who has rotavirus and is experiencing acute vomiting and diarrhea. Manifestations that indicate moderate to severe dehydration? Sunken anterior fontanel. A nurse is caring for a toddler with severe dehydration and its associated acid-base imbalance. What compensatory mechanism within the body is activated to counteract the effects of the child's acid-base imbalance? Increased respiratory rate. A toddler is admitted to the pediatric unit with diarrhea and severe dehydration. After several days of treatment, the child is evaluated. What clinical findings indicate that the child is rehydrated? Decreased hematocrit. Increase in daily weight. Decreased blood urea nitrogen level. A nurse is caring for a toddler who is experiencing acute diarrhea and has moderate dehydration. Which of the following nutritional items should the nurse offer to the toddler? Oral rehydration solution. A nurse is assessing a toddler who has gastroenteritis and is exhibiting manifestations of dehydration. Which of the following findings should the nurse address first? Tachypnea. The nurse manager of the infection control service is teaching a class for nurses on the care of young children with viral infection-related diarrhea. What therapy should the nurse manager recommend? Oral rehydration therapy until fluid balance is restored. A nurse is caring for a 2 year old child with vomiting and dehydration. Which of the following assessments should prompt the nurse to contact the primary care provider? Potassium 2.5 mEq/l. A nurse is caring for a child with dehydration. Which should the nurse recognize as an appropriate assessment to determine the child's response to parenteral fluids? Weighing the child at the same time every day. ❖ Depression- common signs are weight loss or gain, report of low self-esteem, and sleeping more than usual. ❖ Developmental learning and growing- their stage and age are important considerations when considering room selection, roommates. Developmental age is based on infant’s due date, a child born at 8 months (premature) will be developmentally at 6 months. This only applies to preterm babies. ◆ Infant (birth- 1 year)- Trust vs. mistrust. Posterior fontanel closes at 2-3 months, anterior at 12 months. • 3 months- provide metallic mirror. • 4 month- Introduce solids starts at 4-6 months (iron fortified cereals). IPV, PCV, RV are all given. The nurse is assessing a 4 month old infant in the well-baby clinic. Which assessments should prompt the nurse to conduct a further evaluation? head lag when pulled from a lying to sitting position. • 5 months- A nurse at a pediatric clinic is assessing a 5-month-old infant during a well-child visit. Which of the following findings should the nurse report to the provider? Head lags when pulled form a lying to a sitting position. • 6 month- Stimulate development by talking to them. Use non-nutritive sucking for comfort and sucking needs. Rattles stimulate motor development. To assess vision, move a toy in front of the child’s face, watching for eye movement. 6-12 months infants show readiness to wean, should be drinking 16-24 ounces/day of formula. o A nurse is performing a physical assessment on a 6 month old. Which of the following reflexes should the nurse expect to find at this age? Babinski, plantar grasp. • 8 month- two teeth. A nurse is performing hearing screenings for children at a community health fair. Which of the following children should the nurse refer to a provider for a more extensive hearing evaluation? An infant who is 8 months old and is not yet making babbling sounds. A nurse is providing anticipatory guidance to the parents of an 8-month-old infant during a well- child visit. Which of the following statements should the nurse make? "Your baby should be able to sit unsupported” A nurse is observing an 8 month old and parent playing peek a boo. The parent asks the nurse if this game has any developmental significance. The nurse should indicate to the parents that playing peek a boo will develop which concepts? object permanence. • 9 month- infant will turn away from nurse. A nurse is assessing a 9 month old infant for potential developmental delay. Which of the following observations should the nurse expect to find to support this condition? inability to sit without support. A nurse is assessing a 9-month-old infant during a well-child visit. Which findings indicates that the infant has a developmental delay? Inability to vocalize vowel sounds. • 10 month- grasp a rattle by the hands, use a crude pincher grasp. • 12 months- should be able to dump raisins out of a box, birth weight has doubled, have 6 teeth. ◆ Toddler (1-3)- Autonomy vs shame and doubt. Pushing a toy lawn mower. With a terminal illness, they will react to the parent’s anxiety and sadness. They need to avoid drinking more than 4-6 ounces/day of juice. These children play by having two toddlers seated together playing with separate stuffed animals. Allow this group to make simple decisions to facilitate development of a autonomy. Paralleled behaviors. When teaching the parents of toddlers, teach them to develop food habits that will prevent dental caries, expression of bedtime fears is common. Expect behaviors associated with negativism and ritualism, they experience separation anxiety (kicking a stranger), displays intense emotions, and exhibits regressive behaviors.. o Expected behavior characteristics of a toddler includes whether or not they express likes and dislikes. A major developmental milestone of a toddler is the achievement of autonomy. What should the nurse instruct the parents to do to enhance their toddler's need for autonomy? Teach the child to accept external limits. A nurse is teaching a group of assistants in a daycare center about toddlers' developmental milestones. What behavior should indicate to the assistants that one of the milestones has been achieved? Accepting external limits. When is the best time to prepare a toddler for impending surgery? Shortly before the procedure. A nurse is educating a parent of a toddler on development. which of the following would be an appropriate response by the nurse? your child will begin to scribble spontaneously using a crayon by 18 months. A nurse is teaching a group of parents of toddlers about growth and development. A parent asks, “Why does me child’s abdomen stick out?” Which of the following statements should the nurse make? "Toddlers do not have well developed abdominal muscles." A nurse is teaching a class to parents about keeping medications and household cleaning supplies out of the reach of toddlers. The nurse explains that this is necessary because toddlers? Have a high level of oral activity. • 15-month-old-walks independently. A nurse in the child life center is evaluating a 15-month-old toddler's ability to perform physical tasks. What behavior indicates to the nurse that the child's development is age appropriate? Drinking from a cup. Walking with a wide-based gait. Throwing toys around the room. • 18 months- verbal developmental characteristic with normal hearing is that child uses at least 10 words. Should be able to throw a ball overhand, use a spoon without rotation. • 2 years- should observe child engaging in play near other children. Child demonstrates the rigidity, ritualism, and determination to be in charge. Building a tower w/3 or 6 blocks. Ready to potty train when a child usually wakes up dry, it may be time to begin. Client can speak in complete sentences. Head circumference exceeds chest circumference warrant further assessment. Send the child’s favorite stuffed animal when they will be napping away from home. o A nurse is observing the growth and development skills of several 2-year-olds in the clinic playroom. The nurse determines that the child requiring further evaluation is the one who? Uses echolalia when speaking. During the second week of hospitalization for intravenous antibiotic therapy, a 2-year-old toddler whose family is unable to visit often smiles easily, goes to all the nurses happily, and does not express interest in the parent when the parent does visit. The parent tells the nurse, "I'm so happy he's adjusting, but should I be worried about his reaction to seeing me?" What is the best response by the nurse? The child is repressing feelings for the parent. A 2-year-old boy who has fallen from a tree tells his parents and the nurse, "Bad, bad tree." The nurse concludes that he is within the cognitive developmental norm of Piaget's Preconceptual operations. A parent tells the nurse, "Our 2½ -year-old child only uses two-word phrases when he's talking, and we can only understand him maybe a quarter of the time. We're really concerned." What should the nurse consider before responding? This seems to be slow language development for a 2½ -year-old. • 3-year-old- Should be playing with tea parties. To decrease withdrawal with hospitalization, encourage the parents to stay with the child. Assess appropriate development by saying, “can you tell me what color this ball is?” Stands on 1 foot. Rides a tricycle. o During a routine visit to the child health clinic the parent of a 3-year-old girl reports, "My daughter is still sucking her thumb." What is the nurse's best response? "She'll stop when she's ready. Several 3-year-old girls in the daycare center are having a tea party with their dolls. The center's nurse concludes that this behavior is: Appropriate make-believe play. The parents of a 3-year- old tell the nurse that their child is afraid to sleep alone because of monsters under the bed. They ask for suggestions. What should the nurse recommend? Leave a small light on at night and state, "Monsters aren't allowed in the house." A 3-year-old boy has been observed in the clinic waiting room taking toys from others, tearing pages out of books, and striking his mother. The nurse takes time when interviewing the mother to ask about television habits because: Viewing violent programs is positively correlated with the development of aggression. ◆ Preschooler (4-5)- Initiative vs guilt. Conservation should occur at this age. A child that thinks that 1 apple cut in ½ is 2 apples is an example. Promote independence by having the child use scissors to cut out a picture. 13-19 grams of complete protein a day. Hand puppets are appropriate for diversion. Psychosocial challenges of independence. Weight gain of 4-6 lbs.’ per year is expected for these children. Allow child to role play using miniature equipment. Only allow 30 minutes of TV before bedtime each night. Average caloric intake should be 1,800 calories per day. Portrays animism- needs to take her doll because, her doll is scared to be at home alone. This group relates their fears to magical thinking. • 4 year olds should be able to walk without tripping and falling down, skip around the room, hopping on one foot, ties shoes, catching the ball, button a shirt. With a terminal illness they may play out death experience with toys, and have the toys come back to life. Magical thinking. Will cope with the distress of hospitalization through the use of drawings. o A nurse is caring for a 4-year-old child who has pneumonia. The child’s mother left 2 hours ago and is currently experiencing the separation anxiety stage of despair. Which of the following findings should the nurse expect? Inactive and thumb sucking. A nurse is assessing a 4-year-old child at a well-child visit. Which of the following developmental milestones should the nurse expect to observe? Cuts a shape using scissor. A nurse is proving education for a group of parents. A parent is concerned about the development of her 4 year old child's fine motor skills. Which of the following should the nurse explain to be an expected skill for this age group? copying a square and circle. A nurse is caring for a hospitalized preschooler. The child's mother is going home for a few hours while another relative stays with the child. Statement that the nurse should make to explain to the child when her mother will return? "Your mommy will be back after you eat." A nurse is providing teaching about social development to the parents of a preschooler. Which play activities should the nurse recommend for the child? Playing dress-up. ◆ School age (5-12)- industry versus inferiority stage of development. Give factual info when describing procedures. Growth differences between boys and girls become evident at this age. Tach them to wear helmets when riding bikes or skateboarding, implement firearm safety, wear seat belts. 11-12 need TIV, MCV4, Tdap. o A charge nurse is preparing to make a room assignment for a newly admitted school-age child. Which of the following considerations is the nurse's priority when making a room assignment? Disease process. A nurse is planning an educational program for school-age children and their parents about bicycle safety. Which of the following information should the nurse plan to include? The child should be able to stand on the balls of her feet when sitting on the bike. • 5 years- explain procedure just prior to it. Play becomes associative, playing a simple game near another child. DTAP, MMR, IPV. • 6 years- A nurse is performing a physical assessment on a 6 year old child. Which of the following findings should prompt the nurse to conduct additional follow-up? sparse, fine pubic hair. Immunizations are MMR, IPV, Dtap, Varicella. Bedwetting can be caused by regression, which is a normal defense mechanism. Should be jumping rope. • 7 years- child who takes pride in bringing home school papers is showing industry versus inferiority. (7-9) chapter books are an appropriate diversional activity. • 8 years- preoperative education achieved by using a doll with tubes and an incision to help explain the surgery. Refusing to go to school after being sick. Have the child describe what things were like before not wanting to go to school. May be upset about upcoming surgery, the nurse can help by saying “let’s talk about what to expect after surgery.” A child stating, “my rock collection is bigger than yours.” o A nurse is assessing an 8 year old child's psychosocial development. Which of the following findings should the nurse recognize as requiring further evaluation? the child complains everyday about going to school. • 10 years- A nurse is planning developmental activities for a newly admitted 10-year-old child who has neutropenia. Which actions should the nurse plan to take? Provide the child with a book about adventure. ◆ Adolescent (13-18)- Identity (Ego) vs role confusion Sleep more r/t rapid growth. Girls stop growing about 2 years after menarche. 13 year olds need an assessment including BMI, weight, scoliosis. Testicular enlargement is the first sign of sexual maturation in boys. o A nurse is performing a yearly physical on an adolescent. The adolescent's parent asks about the adolescent's developmental needs. Which of the following statements by the parent should the nurse investigate further? "He spends several hours a day on the internet." A nurse is teaching to a group of adolescents about developmental needs. Which of the following statements by a parent should the nurse investigate further? My child spend 4 hours a day in internet chat rooms. ❖ Developmental dysplasia of the hip- Can apply harness over t-shirt and knee socks, return to the clinic for required harness adjustments, do not apply baby powder to the baby’s skin around the harness buckles every day. Hip dysplasia patients are frequently placed in a hip Spica cast, and the Pavlik harness is used for infant’s less than 6 months of age. Trendelenburg’s sign is an assessment the nurse will include with diagnosing. o A nurse is teaching the parent of an infant who has a Pavlik harness to treat developmental dysplasia of the hip. The nurse should identify that which of the following statements by the parent indicates an understanding of the teaching? "I will place my infant's diapers under the harness straps. o Diabetes Mellitus- sick day management includes monitoring the blood glucose levels every 3 hours, test urine for ketones, call the provider if blood glucose is greater than 240. Hypoglycemia- hunger, irritability, sweating, and pallor. A nurse is caring for a 3 year old child newly diagnosed with diabetes mellitus. When writing the care plan, the nurse includes this goal: The child will be provided with opportunities for therapeutic play. Which of the following would be the most appropriate toy to help meet this goal? doll and a syringe with no needle. A nurse is caring for a 6 year old child who is newly diagnosed with diabetes mellitus. The nurse is educating the child on how to do finger sticks for blood glucose checks. The nurse knows the most effective method to teach this skill will be? Allow the child to practice the skill on themselves or others. o Insipidus- 10-year-old child following a head injury. Findings that indicate the development of DI? Sodium 155. Insulin- you should give 4 or 5 injections in the same site for switching sites. A nurse is teaching a school-age child and his parents how to self-administer insulin. Which actions should the nurse take first? Demonstrate the injection technique on an orange. o Ketoacidosis- dehydration, mental confusion, fruity breath are common manifestations. A nurse is caring for a school-age child who has diabetes mellitus and was admitted with a diagnosis of diabetic ketoacidosis. Cardiac monitor showing a change in T- waves is concerning. When performing the respiratory assessment, which findings should the nurse expect? Deep respirations of 32/min. A nurse is caring for an adolescent with diabetes mellitus who has been admitted twice this year to the hospital with diabetic ketoacidosis. Which of the following tests should the nurse recognize as the best information to evaluate the client's compliance? Hemoglobin A1C. A nurse is caring for a child who is receiving treatment for diabetic ketoacidosis and has a current blood glucose level of 250mg/dl. Which of the following actions should the nurse take? Administer 5% Dextrose in 0.9% sodium chloride by continuous IV infusion. o Type 1- self-care involves drinking a glass of milk when child is feeling irritable. A nurse is teaching a school-age child who has a new diagnosis of type 1 diabetes mellitus. A vial of insulin can be used for 30 days. The nurse should identify which of the following statements by the child as understanding the teaching? "I will give myself a shot of regular insulin 30 minutes before I eat breakfast. A nurse is providing teaching to the parents of a school-age child how has type 1 diabetes mellitus about management of hypoglycemia. Which of the following responses by the parents indicates an understanding of the teaching? I will make sure my child drinks 240 mL (8 oz) of milk as soon as possible. A nurse is providing diabetic teaching to a 12-year-old child who appears apprehensive during the teaching. Which actions should the nurse recognize as appropriate in this situation? Teach the child to do her own fingersticks. ❖ Diaper dermatitis- allow buttocks to air dry, apply Zinc Oxide ointment to the affected area, superabsorbent diapers can be used to assist in keeping the baby dry. Avoid Talcum powder, commercial baby wipes. ❖ Diet- A nurse is caring for a 10-year-old child who is obese. Which of the following menu choices is the most appropriate for this child? A glass of skim milk, baked fish sandwich on whole wheat roll with lettuce, and a medium apple. A nurse is providing teaching to the parent of a 2-year-old toddler about nutrition. Which of the following statements by the parent indicates an understanding of the teaching? My child should consume 1,000 calories/ day. A nurse is teaching the parent of a 12-month-old infant about nutrition. Which of the following statements by the parent indicates a need for further teaching? My infant drinks at least 2 quarts of skim milk each day. A nurse is caring for a 10-year-old child who should reduce his fat intake. Which of the following menu choices should the nurse suggest? 3 oz. of baked chicken on a whole wheat roll. ❖ Down’s Syndrome- these children have a protruding abdomen, broad short feet and hands, hypotonia. Parents should place a cool mist humidifier in their rooms to help them breathe better at night. ❖ Ears- light reflex should be located around the 5 or 7 o’clock position. Tympanic membrane is pearly, pink, or gray color. Bony landmarks should be visible. The presence of cerumen bilaterally is normal. ❖ E-coli- bloody stools, severe abdominal cramping, it can lead to hemolytic uremic syndrome, it is a foodborne pathogen. ❖ Eczema- generalized distribution of lesions, ecchymosis in flexural areas, and crusting lesions are common findings. ❖ Egocentrism- seeing something only from one’s own point of view, inability to see other’s point of view. ❖ Electroencephalogram (EEG)- decaffeinated beverages should be offered on the morning of the procedure. ❖ Enterobius vermicularis- perform a tape test. ❖ Epiglottis- the nurse should suspect hoarseness and difficulty speaking, difficulty swallowing, drooling, and stridor. o A nurse in an ER suspects that a toddler has epiglottitis. Which of the following actions should the nurse take? Prepare the toddler for nasotracheal intubation. A nurse in the ED is caring for a school-age child who has epiglottis. Which actions should the nurse take? Monitor the child's O2 saturation. A nurse is preparing to suction an infant who has a tracheostomy. Which action should the nurse take? Suction for 5 seconds or less. A nurse in an emergency department is caring for a toddler who is in acute respiratory distress. Which findings should alert the nurse to the possibility of epiglottitis? Drooling. ❖ Epispadias- bladder exstrophy, widened pubic symphysis, broad, spade-like penis. ❖ Epistaxis- when experiencing a nosebleed have the child sit up and lean forward, press the nares together for at least 10 minutes, pack cotton or tissue into the naris that is bleeding. o A nurse is caring for a child who has epistaxis. Which of the following actions would be the most appropriate for the nurse to take? Apply a cold cloth to bridge of nose. A nurse is caring for a child who has epistaxis. Which of the following actions would be the most appropriate for the nurse to take? Apply continuous pressure to the child’s nose for at least 10 minutes. Use thumb and forefinger. Keep child calm. ❖ Erythema infectiosum- A school nurse is assessing a school-age child who has erythema infectiosum (fifth disease). Which of the following findings should the nurse expect? Facial rash. ❖ Extravasation of tissue- stop infusion, elevate the extremity, notify the provider, remove the IV line. ❖ Failure to thrive- A nurse is planning care for a 10-month-old infant who has suspected failure to thrive (FTT). Which of the following interventions should the nurse include in the plan of care? Observe the parents' actions when feeding the child. Maintain a detailed record of food and fluid intake. A nurse is caring for a 3 month old infant admitted with suspected non- organic failure to thrive. Which of the following statements is true regarding non-organic failure to thrive? disruption in the parent-child bond. These children will have a risk for? Developmental delays. ❖ Fine motor- nine month old unable to pass the cue from one and to another. ❖ Fractures- epiphyseal plate injuries can result in altered bone growth. Manifestations- crepitus, edema, pain, and ecchymosis. ❖ Gastroesophageal reflux- offer frequent feedings, thicken formulas with rice cereal, position baby upright after feedings. o A clinic nurse is providing teaching to the parent of a 1-month-old infant who has gastroesophageal reflux. Which of the following statements by the parent indicates an understanding of the teaching? I will add rice cereal to my baby's feedings. A nurses teaching the parents of a 4 month old infant who has gastroesophageal reflux. Which of the following statements by the parent indicates an understanding of the teaching? I will add 1 teaspoon of rice cereal per ounce to my baby’s formula. Longer intestinal tracts than adults, put the infant’s at higher risk for electrolyte imbalances when compared. ❖ Gastrointestinal disorders- initiate oral rehydration therapy for a child with watery diarrhea for over 3 days. ❖ Glomerulonephritis- serum creatinine 1.3 mg/dl needs to be reported to provider. Poststreptococcal glomerulonephritis- manifests as periorbital edema, ill appearance, hypertension. o A nurse is caring for an 8-year-old child who has acute glomerulonephritis. Which of the following findings should the nurse expect? Periorbital edema. A nurse is preparing to obtain an antistreptolysin O (ASO) titer from a child who has acute glomerulonephritis. The child's parent asks the… nurse to explain the purpose of the test. Which of the following responses should the nurse make? The test shows us if your child had a recent strep infection. A nurse is caring for an 8-year-old child who has acute glomerulonephritis. Which of the following should the nurse expect to find with this client? Elevated red blood cells. nurse is caring for a 7-year-old child diagnosed with glomerulonephritis. The child has decreased urinary output and a blood pressure of 160/78 mm Hg. The child is receiving hydralazine (Apresoline). Which of the following lunch choices should the nurse recognize as most appropriate? Grilled chicken on a roll, pear slices, and 4 oz. of apple juice. A nurse is caring for a child who has acute glomerulonephritis. Which of the following actions should the nurse recognize as appropriate in the care of this child? Monitoring blood pressure every 4 hour. A nurse is caring for a child who has acute glomerulonephritis. Which of the following actions should the nurse take? Check the child’s blood pressure every 4 hour. ❖ Gross motor- able to roll from back to stomach, sitting up without assistance. ❖ Growth Hormone Deficiency- child with short stature. This is diagnosed with CT scan of the head, bone age scan, GH stimulation test serum ICF-1. If this remains untreated it can result in a complication of delayed sexual development, premature aging, short stature. Injections for treatment are continued until there is evidence of epiphyseal closure. Proportional height-weight is an indication of growth hormone deficiency. ❖ Health screening- Planning care for a toddler who has a serum lead level of 4 mcg/dL. Appropriate action to take is to schedule the toddler for a yearly rescreening. A nurse is assessing a 12-month-old male infant's vital signs during a well-child visit. The infant is in the 90th percentile of height. Which of the following findings should the nurse report to the provider? Heart rate 175/min. A nurse is performing a physical assessment on a 30 month old toddler. Which of the following nursing assessments should the nurse not expect to find at this age? birth weight is tripled. A nurse in a pediatric clinic is assessing a toddler at a well child visit. which of the following actions should the nurse take? Minimize physical contact with the child initially. A nurse is assessing a 4-year-old child at a well-child appointment. The parent expresses concern over the child’s stuttering. The nurse provides teaching to the parent. Which of the following statements by the parent indicates a need for further teaching? "It may help if you encourage your child to stop and begin the word over." ❖ Hearing- indications of impairment are a child using monotone speech, speaking loudly, and appears shy. o A nurse is caring for a child who will be receiving PE tubes in the morning. The nurse is teaching the parents how to care for the tubes upon discharge. Which of the following statements should indicate to the nurse that the teaching was understood? "I will keep water out of my child's ears." ❖ Heart failure/ disease- cool extremities, peripheral edema, nasal flaring, tachycardia, decrease in urinary output. o A nurse is creating a plan of care for a school-age child who has heart disease and has developed heart failure. Which interventions should the nurse include in the plan? Provide small, frequent meals to the child. nurse receives the following laboratory values on a 2-month-old child who has cyanotic heart disease. The results are a hemoglobin of 17 g/dL and a hematocrit of 51%. Which of the following statements by the nurse reflects the most appropriate interpretation of this information? "The infant's body is compensating for tissue hypoxia by increasing. RBC production." ❖ Hemophilia- A 2-year-old child with previously diagnosed hemophilia is admitted to the pediatric unit for observation after a motor vehicle collision. The toddler has several bruises but no other apparent injuries. What is the nurse's specific concern regarding this child? Undetected injury. A home health nurse is developing a plan of care for the parents of a toddler who has hemophilia. Which of the following instructions should the nurse include in the plan? Inspect the toddler's toys for sharp edges. ❖ Hernia- A nurse is conducting postoperative teaching for the parent of a 3-month-old infant who is recovering from an umbilical hernia repair. Which of the following statements by the parent indicates an understanding of the teaching? "I will keep (fold) my baby's diaper away from the incision." ❖ Hirschsprung’s disease- prepare the family for surgery. ❖ HIV- transmitted through IV substance use. Obtain yearly influenza vaccinations, standard precautions. Mild symptomatic category- dermatitis, hepatomegaly, lymphadenopathy. Moderate symptomatic category- anemia, herpes, hepatitis, cardiomyopathy. Severe symptomatic category- Kaposi’s sarcoma, wasting syndrome, pulmonary candidiasis. ❖ Hospitalization- encourage optimal nutrition in the child by allowing the child to eat with others. o What behavior does a nurse expect from a toddler subjected to prolonged hospitalization with limited parental visits? Cheerful interactions with staff members. 10 month old infant has been hospitalized four times for a total of 42 days. The nurse notices that the infant does not seem upset when the parents leave. Which of the following should the nurse recognize as an appropriate explanation for this behavior? Experiencing detachment. A nurse is caring for a hospitalized 3 year old child who the parents report is toilet trained. Since admission to the hospital, the child has experienced bed wetting. Which of the following is an appropriate response by the nurse? "Let's get you cleaned up so you can go to the playroom." A nurse is caring for a 4 year old who has been admitted to the hospital. Which of the following would be the appropriate toy for the 4 year old? plastic stethoscope. A nurse is caring for a toddler who is scheduled for surgery. The parent asks the nurse for suggestions on how to prepare her child for the upcoming surgery. Which of the following would be an appropriate statement by the nurse to the parent? you could read books to your child about being hospitalized. A nurse on a pediatric unit is reviewing the health record of a client who is demonstrating increasing levels of stress after admission. The nurse should identify which of the following findings as a risk factor for a stress-related reaction to hospitalization? Male gender. nurse is preparing a 7 year old child for a tonsillectomy. Which of the following nursing actions would be appropriate in this preparation? Schedule the child for a preoperative visit to the hospital. ❖ Hydrocele- explain to the parents that this issue will resolve. ❖ Hyperbilirubinemia- when undergoing phototherapy for treatment, remove newborn’s eye mask during feeding. ❖ Hyperopia- this is always reported. ❖ Hypertrophic pyloric stenosis- manifestations are projectile vomiting, dry mucous membranes, constant hunger. ❖ Hypopituitarism- A nurse is caring for a newly-admitted school-age child who has hypopituitarism. Which of the following meds should nurse expect the provider to recommend to the parents for TX the child's condition? Recombinant growth hormone ❖ Hypospadias- A nurse is providing discharge teaching to the parents of a 6-month-old infant who is postoperative following hypospadias repair with a stent placement. Which of the following instructions should the nurse include in the teaching? "Allow the stent to drain directly into your infant's diaper.” A nurse is caring for a 3-year-old child who is in need of a hypospadias repair. Which of the following should the nurse recognize as a concern to this age group? Damage to body integrity. ❖ Hypothyroid- A nurse is teaching the parents of a newborn who has congenital hypothyroidism about care of their child. Which should the nurse recommend to the parents? Life-long administration of thyroid hormone. Congenital hypothyroidism- cool extremities, and a short neck. ❖ Immunizations- 2 month old will receive rotavirus, DTAP, HIB, PCV 13, IPV. 4 year old receives IPV, MMR, VAR, DTAP. o Administration- IM in the dorsogluteal. For infant administration ask the pharmacy to add flavoring to the medication, use the nipple of a bottle to administer the medication, hold the infant in a semi-reclining position. With toddlers we want to calculate the safe dosage, ask the toddler what toy he or she wants to hold, offer juice after administration. A nurse is preparing to administer an immunization to a 4-yo child. Which of the following actions should the nurse plan to take? Administer the immunization using a 24-gauge needle. Provide sucrose pacifier for comfort. o DTAP. 5 immunizations are given during childhood. An 18-month-old toddler who has received the appropriate immunizations on time is visiting the pediatric clinic for the next scheduled immunization. What vaccine should the nurse administer? Fourth diphtheria toxoid, tetanus toxoid and acellular pertussis (DTaP) vaccine. A nurse at a clinic is preparing to administer immunizations to a 5 year old child. Which of the following immunizations should the nurse plan to give? Diphtheria, tetanus, and pertussis (DTaP). A nurse at the immunization clinic is preparing to administer injections to a 5 year old child. Which of the following is the appropriate injection for the nurse to administer? Diphtheria. A nurse is working at an immunization clinic. Which of the following would be a contraindication to the pertussis immunization? known neurological or seizure disorder. o HIB. A nurse is caring for a 2 month old infant who is brought to the clinic for routine immunizations. Which of the following should the nurse administer? DTaP HIB, IPV, HBV. A nurse is preparing to administer recommended immunizations to a 2-month- old infant. Which of the following immunizations should nurse plan to administer? Haemophilus influenzae type B (Hib) & inactivated polio virus (IPV). o Influenza- place children in supine position w/administration. Oseltamivir is given within 48 hours of onset of symptoms. When administering immunizations to a toddler during a well-child visit, withhold the influenza vaccine. A nurse is providing teaching about immunizations to parents of a severely immunocompromised child who has HIV. Which statements should the nurse include in the teaching? The pneumococcal and influenza vaccines are recommended for your child. o MMR. A nurse is providing education to the parent of a toddler who is about to receive her first dose of the MMR (measles, mumps and rubella) immunization. Which of the following statements by the parent indicates an understanding of the teaching? I can give my child acetaminophen for discomfort associated with the immunization. o Meningococcal. A nurse is caring for an 18 year old adolescent who is going away to college. The adolescent will be living in the dorms. Which of the following is the most appropriate immunization to suggest that he receive? meningococcal polysaccharide. o Poliovirus. An 18-month-old child has received all required immunizations. What immunization should the nurse explain to a parent will be one of the vaccines required between 4 and 6 years of age? Inactivated poliovirus. A nurse is caring for a preschooler diagnosed with human immunodeficiency virus who is at the clinic to receive immunizations. Which statements about HIV immunizations is the most appropriate? The only immunization contraindicated for this client is the oral polio. o Tetanus. A nurse in an emergency department is caring for an 8-year old who is up-to-date with current immunization recommendations and has a deep puncture injury. Which should the nurse anticipate administering? Adult tetanus booster. o Varicella (VAR)- contraindicated with Corticosteroid medications. ❖ Impetigo- vesicular, honey colored, crusty region around nose and mouth. Teaching is to apply topical antibacterial to lesions, place burrow solution compresses over affected areas, trim and clean fingernails regularly while lesions are present. ❖ Increased intracranial pressure- report of headache, alteration in pupillary response, increased sleeping indicate increased ICP. The nurse’s actions are to maintain a quiet environment, administer a stool softener, maintain body alignment. o A nurse is assessing a school-age child who has an infratentorial brain tumor. Which of the following findings should the nurse identify as a manifestation of increased ICP? Decreased attention span. ❖ Intravenous fluids- A nurse is caring for a preschooler who has been receiving IV fluids via a peripheral IV catheter. When preparing to discontinue the IV fluids and catheter, which of the following actions should the nurse plan to take? Turn of the IV pump, Occlude the IV tubing, Remove the tape securing the catheter, Apply pressure over catheter insertion site. A nurse is planning care for a school-age child who has a tunneled central venous access device. Which interventions should the nurse include in plan? Use a semipermeable transparent dressing to cover the site. ❖ Intussusception- Vomiting related to the obstruction that occurs when a segment of the bowel telescopes within another. Lethargy r/t episodes of severe pain in which the infant cries leading to exhaustion and decreased nutritional intake. Bloody stools that are currant and jelly-like in appearance are an expected finding. o A nurse is admitting an infant who has intussusception. Which of the following findings should the nurse expect? vomiting, lethargy. A nurse is caring for a child who has a possible intussusception. The parents of the child ask the nurse how the diagnosis is made. Which of the following responses should the nurse make? An abdominal ultrasound will confirm the pocket in the intestine. A nurse is providing care to a child with a possible intussusception. The parents of the child ask the nurse how the diagnosis is made. Based on an understanding of the diagnostic evaluation for intussusception, which of the following statements should the nurse use? "A barium enema will be given to visualize the obstruction". A nurse is caring for a 6-month- old infant who has colic and vomiting who will be undergoing testing to rule out intussusception. Which of the following would be the appropriate treatment for intussusception? Barium enema. ❖ Iron deficiency anemia- liquid oral iron supplementation should be taken through a straw to decrease risk of staining teeth. When administering IM iron Dextran for iron deficiency anemia use the Z-track method with dose. o A nurse is reviewing the dietary choices of an adolescent who has iron deficiency anemia. The nurse should identify that which of the following menu items has the highest amount of iron? 1/2 cup of raisins. A nurse is reviewing the lab report of a school- age child who is experiencing fatigue. Which of the following findings should the nurse recognize as an indication of anemia? Hematocrit 28%. A 1-year-old child is found to have nutritional iron-deficiency anemia. What interventions are important in the care of an infant with iron-deficiency anemia? Conserving the infant's energy, Protecting the infant from infection, Teaching parents about nutrition. A nurse is caring for a child who has a diagnosis of iron deficiency anemia. Which of the following instructions would be appropriate for the nurse to give to the parents? "Give the iron between meals with orange juice." A nurse is teaching parents of a 10-year-old child who has iron deficiency anemia. Which of the following statements by a parent indicates an understanding of the teaching? I will administer the tablet with orange juice. ❖ Isolation precautions- A nurse is caring for an infant on droplet precautions. The nurse understands that she can best prevent the spread of droplet pathogens by doing which of the following? wearing a gown and mask when feeding the infant. A nurse is caring for a 15-month-old toddler who requires droplet precautions. Which of the following actions should the nurse take? Wear a mask when assisting the toddler with meals. ❖ Juvenile idiopathic arthritis- Perform morning stretching exercises to reduce pain and contractures. Provide extra time for completion of ADL’s, perform ROM exercises. o A nurse is providing teaching to the family of a school-age child who has juvenile idiopathic arthritis. Instructions to be included in the teaching? "Encourage child to perform independent self-care". ❖ Kawasaki- child will be irritable for a few weeks, keep record of child’s temp until no fever for several days. o A nurse in the emergency department is assessing a toddler who has Kawasaki disease. Which of the following findings should the nurse expect? Increased temperature, xerophthalmia, cervical lymphadenopathy. A toddler with a history of enlarged lymph nodes, prolonged fever that is unresponsive to antibiotics, erythema of the extremities, and a rash is admitted to the pediatric unit with a diagnosis of Kawasaki disease. What’s essential in confirming this diagnosis? A Combination of signs. ❖ Leg-Calve Perthes disease- diagnostic procedure is radiographs. Manifestations- hip stiffness, limited ROM, limp with walking. ❖ Leukemia- early manifestations are anorexia, petechiae, and an unsteady gait. o A nurse is obtaining a health history from the parents of a toddler who has recently been diagnosed with acute lymphocytic leukemia. Which early physiological changes does the nurse expect the parents to report? Pale skin, Eating less food. Purplish spots on the skin. A nurse is admitting a child who has a possible diagnosis of leukemia. Which of the following tests is the most appropriate for the nurse to consider when confirming a diagnosis of leukemia? Bone marrow aspiration. A nurse is admitting a child who has acute lymphocytic leukemia. Which lab values should the nurse expect? RBC 2.5. ❖ Loss- A nurse is discussing organ donation with the parents of a school-age child who has sustained brain death due to a bicycling accident. Which of the following actions should the nurse take first? Explore the parents' feelings and wishes regarding organ donation. A hospice nurse is caring for a preschooler who has a terminal illness. The father tells the nurse that he cannot cope anymore and has decided to move out of the house. Which of the following statements should the nurse make? "Let's talk about ways you have handled previous stressors in your life”. The mother of an 18-month-old toddler tells the nurse in the pediatric clinic that her child is "unmanageable and into everything." What is the most important teaching to include during this clinic visit? Accidents are the leading cause of death and injury in this age group. A nurse is developing a plan of care for a school-age child who underwent a surgical procedure that resulted in a temporary loss of vision. Which of the following interventions should the nurse include in the plan of care? Explain sounds the child is hearing. ❖ Lumbar puncture- adolescent for lumbar puncture apply topical analgesic cream to the site 1 hour prior to the procedure. Retrain infant during procedure to prevent movement. ❖ Meckel’s diverticulum- abdominal pain, mucus, and bloody stools are common findings. ❖ Medication administration- A nurse is providing teaching to the parents of a toddler about the administration of prescribed eye drops and eye ointment. Instructions to include? "Administer the eye drops 3 minutes before the ointment." A nurse must administer a medication by means of injection to a 2-year-old whose parent is not present. What is the most therapeutic approach for the nurse to use? Warning the child about the injection just before administering it, saying that it is OK to cry, and then comforting the child. A nurse is preparing to administer an injection to a 2 month old infant. Which of the following is an appropriate site for the nurse to give the injection? Vastus lateralis. A nurse is caring for an infant who is crying. The nurse plans to administer a liquid medication. Which of the following administration methods should the nurse use? place a needless syringe in the buccal cavity. A nurse is preparing to administer a liquid medication to an infant. Which of the following actions should the nurse take? Give the medication at the side of the infant's mouth. A nurse is teaching a 12-year-old child how to use an steroid inhaler. The nurse should recognize that the teaching has been effective when the child makes which of the following statements? "I will use this medication every day even if I don't have any manifestations." A nurse is teaching the parent of a toddler about home safety. Which of the following statements by the parent indicates an understanding of the teaching? I lock my medications in the medicine cabinet. Education. A nurse is caring for an adolescent who is receiving pain medication via a PCA pump. When the nurse assess the client's pain at 0800, the client describes the pain as a 3 on a scale of 1 to 10. At 100, the client describes the pain as a 5. The nurse discovers the client has not pushed the button to deliver medication in the past 2 hr. Which of the following actions should the nurse take? Reinforce teaching with the client about how to push the button to deliver the medication. A nurse is caring for a 10-year-old child who is postoperative abdominal surgery and was medicated 6 hour ago. When assessing the child, the nurse finds the child quiet and not interacting with family. Which of the following is an appropriate nursing action? Assess the child's need for pain medication. o Digoxin- Treats cardiac anomalies. Give the correct dose off medications at regularly scheduled times. Providing teaching to the parents of a preschooler who has heart failure and who is beginning to take digoxin twice daily. Appropriate instructions to include? "Brush the child's teeth after giving the medication." A nurse is admitting a 4-month-old infant who has heart failure. Which findings are the nurse's priority? Episodes of vomit. The 3 episodes of vomiting can indicate digoxin toxicity. o Epinephrine- A nurse is teaching a school-age child who has a severe allergy to bee venom and his parent about epinephrine. Which of the following instructions should the nurse include in the teaching? Use a second dose if the first dose of epinephrine does not completely reverse the symptom. A nurse is caring for a school-age child who is receiving cefazolin via intermittent IV bolus. The child develops diffuse flushing of the skin and angioedema. After discontinuing the medication infusion, which of the following medications should the nurse administer first? Epinephrine. A nurse in an ED is caring for a school-age child who is experiencing an anaphylactic reaction. Priority action by the nurse? Administer IM epinephrine to the child. o Isotretinoin-prescribed for the treatment of acne. The nurse should plan to monitor cholesterol and triglycerides, these will be elevated as an adverse effect. o Mannitol- used to treat cerebral edema. Adverse effects are confusion, tachycardia, weight gain, urinary retention, diarrhea. o Nystatin- A nurse is providing teaching to the parent of a school-age child who has oral candidiasis and is to begin taking oral nystatin. Which instructions should the nurse include? "Shake the medication prior to administration”. o Polystryrene sulfonate enema- A nurse is assessing an adolescent who received a sodium polystryrene sulfonate enema. Which of the following findings indicates effectiveness of the medication? The adolescent's serum potassium level is 4.1 mEq/L. o Steroids- A nurse is caring for a school-age child who has primary nephrotic syndrome and is taking prednisone. Following 1 week of treatment, which of the following clinical manifestations indicates to the nurse that the medication is effective? Decreased edema. A 5-year-old child is brought into the clinic with lethargy, abdominal ascites, and peripheral and periorbital edema. The history indicates ongoing diarrhea and decreased urine output. The child is found to have nephrotic syndrome and started on corticosteroid therapy. The nurse informs the parents that after a week or two of medication therapy, they can expect the child to exhibit: diuresis. A nurse is caring for a child diagnosed with nephrotic syndrome who is receiving Predisone (Deltasone). Which of the following should the nurse recognize as a therapeutic response of the medication? Weight drops 500 g. In planning care for a child with severe reactive airway disease, the nurse knows that when chronic steroid use is indicated, inhaled steroids are preferred over oral steroids for which reason? Oral steroids can slow linear growth in children. o Succimer (Chemet)- A toddler with lead poisoning is started on chelation therapy. Succimer (Chemet) is ordered. What information should the nurse give the parents concerning the administration of this medication? The contents of the capsules may be sprinkled on food. o Tobramycin (Ototoxic medication)- A nurse is interviewing the parent of an 18-month-old toddler during a well-child visit. The nurse should identify that which of the following findings indicates a need to assess the toddler for hearing loss? The toddler received tobramycin during a hospitalization 2 weeks ago. o Tylenol- pallor with overdose can appear as early as 2 hours after ingestion. A nurse is caring for a child who has been brought to the ER after ingesting a bottle of acetaminophen (Tylenol). Which medications should the nurse anticipate administering? Acetylcysteine (Mucomyst). A nurse is caring for a child who has cellulitis and a rectal temperature of 102.2° F (39° C). The child has an order for acetaminophen (Tylenol) 280 mg by mouth. The label on the bottle reads 160 mg/5 mL. Which of the following is the correct dose the nurse should dispense to the child? 8.8 mL. acetaminophen can be given for minor discomforts like a low- grade fever of muscle aches after a vaccination. A parent calls a primary care provider's office and says her child has a respiratory infection and a temperature of 39° C (102.2° F). The nurse instructs the parent to give the child 240 mg of acetaminophen (Tylenol). The label on the bottle reads 160 mg/5 mL. The nurse should instruct the parent to administer which of the following doses? 1 1/2 tsp o Zidovudine- A 1-year-old infant is receiving zidovudine (AZT) for management of HIV infection. The nurse determines that the infant is exhibiting signs of life-threatening zidovudine toxicity. What finding supports this conclusion? Bruises over the body o Zinc oxide- a nurse is providing teaching to the parent of an infant who has diaper dermatitis. The nurse should teach the parent to apply which of the following to the affected area? Zinc oxide. ❖ Meningitis- a child with decreased level of consciousness, and suspected meningitis, will be placed on NPO status. These children will have a high pitched cry. At 1 am a 28-month-old toddler is admitted to the pediatric unit with suspected meningitis. At 3 am, after the child is settled in, the mother tells the nurse, "I have to leave now, but whenever I try to go my child gets upset and then I start to cry." What is the best action by the nurse? Staying with the child while the mother leaves. o Bacterial meningitis- pneumococcal conjugate vaccine (PCV) and Haemophilus influenza type B (HIB) vaccine decreased the incidence of bacterial meningitis in children. A nurse is reviewing the lumbar puncture results of a school-age child suspected of having bacterial meningitis. Which of the following results should the nurse identify as a finding associated with bacterial meningitis? Increased protein concentration. When creating a plan of care for a newly-admitted adolescent who has bacterial meningitis, the nurse should plan to maintain the adolescent on droplet precautions for 24 hr. following initiation of antimicrobial therapy. A 2½-year-old toddler is admitted with a fever of 103º F (39.4° C), stiffness of the neck, and general malaise. The diagnosis is acute bacterial meningitis. What is the priority nursing intervention for this child? Instituting droplet precautions. A 13-month-old child is undergoing lumbar puncture for confirmation of a diagnosis of bacterial meningitis. During the procedure the nurse notes that the spinal fluid is cloudy. What does finding indicate? Increased white blood cell (WBC) count. A 13-month-old child is admitted with a tentative diagnosis of bacterial meningitis, and the practitioner schedules a lumbar puncture. What is the most important action the nurse should take in preparation? Asking the parents what they were told about the test. o Meningococcal meningitis- presents with elevated temperature, nuchal rigidity, and vomiting. The client will be isolated for 24- 72 hours after the start of antibiotic therapy. Not transmitted after this time period r/t not being in communicable form. o Viral meningitis- indicated with negative gram stain, normal glucose content, normal protein content. ❖ Metered dose inhaler- shake inhaler while holding it in upright position, position the mouthpiece in the mouth, slowly inhale the medication, hold breath for 5-10 seconds. Shake the device prior to use, rinse and expectorate after administration, inhale slowly with medication administration. ❖ Muscular dystrophy- expected findings are muscular weakness in lower extremities, unsteadiness, wide based or waddling gait. ❖ Myelomeningocele- with repair, priority intervention is to measure head circumference. Apply a sterile, moist dressing on sac. A nurse is planning care for a 2-day-old infant who has a myelomeningocele. Which of the following nursing measures should take highest priority in the immediate postoperative period? Measure the head circumference every shift. A nurse is teaching a newly hired nurse about the care of an infant who is postoperative following myelomeningocele repair. The nurse should teach the newly hired nurse to monitor the infant for which of the following complications? Hydrocephalus. A nurse is caring for a 2- day-old infant who has a myelomeningocele. Which actions should the nurse take? Monitor the infant’s head circumference. ❖ Myopia- findings are headaches, difficulty reading, poor school performance. ❖ Nebulized aerosol therapy- used for bronchodilator medications. The nurse should obtain vital signs prior to the procedure, tell the child to take slow, deep breaths, determine if the child should wear a mask, attach the device to an air source. ❖ Necrotizing enterocolitis- risk factor is gestational age of 36 weeks. ❖ Nephrotic syndrome- appropriate nursing interventions are to provide meticulous skin care. Fluid restriction, protein, sodium, and fat restriction may also be necessary. Report a serum protein level of 5.0 g/dl. S/S- facial edema, edema in the ankles, hyperlipidemia, anorexia, weight gain, reduced urine output, swelling that is worst in the morning, and decreases as the day progresses. Chronic renal failure- leads to delayed growth. o A nurse is creating a plan of care for a toddler who has minimal change nephrotic syndrome (MCNS) and 3+ pitting edema. Interventions included in the plan of care? Administer corticosteroids to the toddler. A nurse is providing discharge teaching to the parents of a child who has nephrotic syndrome. Which of the following instructions should the nurse include in the teaching? Keep child away from people who have an infection. A nurse is caring for a child who has suspected nephrotic syndrome. Which of the following laboratory values should the nurse expect? Serum cholesterol 700 mg/dl. ❖ Nephrectomy- A nurse is caring for a 3 year old child who is scheduled for a nephrectomy. When preparing preoperatively, which of the following actions should the nurse recognize as appropriate? Explain the procedure to the child in simple sentences just before administering the preoperative sedation. ❖ Neuroblastoma- a metastasis from the primary site will appear as bone pain, periorbital ecchymosis, proptosis, and a ill appearance. ½ of these kids have metastatic disease, will need a bone marrow biopsy, and surgery for resection of the tumor. ❖ Neuropathy- signs are constipation, foot drop, jaw pain. ❖ Obstructive uropathy- urinary tract infections, hydronephrosis are expected findings. ❖ Operant conditioning- behavioral changes occur when desired behaviors are rewarded. ❖ Oral mucositis- offer soft foods, use a soft disposable toothbrush for oral care, encourage gargling w/warm saline mouthwash. ❖ Orchiopexy- A 2-year-old boy born with cryptorchidism is to undergo orchiopexy. What should the nurse tell the parents about the anticipated outcome of this surgery? damage to the undescended testicle will be prevented. ❖ Osteomyelitis- An Erythrocyte sedimentation rate value, that is above the reference range, is an indication of osteomyelitis. This test is used to screen for osteomyelitis. There is no cure, symptoms are treated with antibiotics. o A nurse is teaching the parents of a school-age child who has a new diagnosis of osteomyelitis of the tibia. The nurse should identify that which of the following statements by the parents indicates an understanding of the teaching? "My child will receive antibiotics for several weeks". A nurse is reviewing laboratory results of a school-age child who is 1 week postoperative following an open fracture repair. Which of the following values should the nurse identify as an indication of a potential complication? Erythrocyte sedimentation rate 18 mm/hr. ❖ Osteosarcoma- spend time with teens to answer any questions they may have. ❖ Otitis media- Speech pattern development is delayed with frequent ear infections. Young children and infants are more at risk for ear infections than older children because, structural differences between Eustachian tubes. Priority is to administer Analgesics to relieve pain. Risk factors are attending daycare, history of cleft palate repair, parents that smoke. Manifestations are tugging on the affected ears, loss of appetite, rolling their head side to side, and crying. Effusion- orange colored tympanic membrane, rhinorrhea, diarrhea, rhinitis, and cough. These children will experience transient hearing loss. o A nurse is caring for a toddler who has acute otitis media and a temperature of 40º C (104º F). After administering acetaminophen, which of the following actions should the nurse plan to take to reduce the toddler's temperature? Dress the toddler in minimal clothing. A nurse is providing preoperative teaching to the parents of a toddler who is to undergo myringotomy. The nurse explains that the type of infection most common in children that are prone to otitis media is: bacterial. A nurse is caring for a 4 month old child who has acute otitis media and a fever of 38.3”C (101`F). which of the following medications should the nurse administer? Amoxicillin. A nurse is caring for a 3-year-old child who has persistent otitis media. When taking the history of the child from her parent, which of the following would be the most appropriate for the nurse to ask regarding the child's recurrent otitis media? "Does anyone smoke around, or in the same house as, the child?" A nurse is providing teaching to the parents of an infant who has acute otitis media about how to administer antibiotic eardrops. Which of the following instructions should the nurse include? Massage the anterior area of the infant's ear following administration. A nurse is caring for a 4 month old infant with otitis media. The nurse is educating the child's parent on how to prevent reoccurrences. Which of the following statements by the parent should the nurse recognize as an understanding of the teaching? I will make sure my baby is sitting upright when drinking a bottle. ❖ Oxygen- for a patient who’s O2 sensor is reading low, 1st action is to ensure proper placement of the sensor probe. Hypoxemia- an early indication is cyanosis. Unconsciousness indicates oxygen toxicity. ❖ Pain management- A nurse is assessing the pain level of a 3-yr-old toddler. FLACC scale used for assessing the infant. Administer IV analgesics around the clock for a child recovering from surgery. Loud cry, lowered eyebrows, rigid body all are indications of pain in an infant. To offer pain relief to infants offer a pacifier, use swaddling, encourage kangaroo care. Atraumatic care- explain procedure using child’s favorite toy, allow the child to make one choice regarding the procedure, apply Lidocaine and Prilocaine cream to three potential insertion sites. o Appropriate pain assessment scale to use? FACES pain rating scale. A nurse is caring for a 2-week-old infant who is breastfeeding and requires a heel stick. Which of the following actions should the nurse take to minimize the infant's pain? Administer sucrose to the infant prior to the procedure. A nurse is caring for a 2½-year-old child who is expressing pain. What is the most reliable indicator of this child's pain? Changes in behavior. A nurse is planning to implement relaxation strategies with a young child prior to a painful procedure. Which of the following actions should the nurse take? Rock the child in long rhythmic movements. A nurse is assisting a provider during a femoral venipuncture on a toddler. The nurse should place the child in which of the following positions? Supine. ❖ Parallel play- child plays independently when in a group. ❖ Pediculosis capitis- use an OTC medication containing 1% Permethrin. ❖ Peripheral edema- A nurse is caring for a school-age child who has peripheral edema. Following assessments that confirm peripheral edema? Palpate the dorsum of the child's feet ❖ Phenylketonuria (PKU)- client will undergo testing of phenylalanine levels twice a week throughout pregnancy. ❖ Pinworms- A nurse in the pediatric clinic is advising the mother of a toddler who has a pinworm infestation. What should the nurse teach the mother about caring for her child during and after treatment? Strategies to prevent reinfestation. The need for medication for the entire family. The importance of handwashing before eating. A nurse is teaching the parent of a preschool-age child about the treatment for pinworms. Which of the following statements by the parent indicates an understanding of the teaching? I will give my child a dose of Mebendazole (Vermox) today and again in 2 weeks. ❖ Plagiocephaly- characterized by the development of a flat spot on the back or side of the head. Sometimes referred to as “flat head.” The baby will need to wear a prescribed helmet 23 hours a day. ❖ Poisoning- Prevention for parents is to teach them to put all cleaning supplies in a locked cabinet. o Cleaning chemicals- prepare for intubation with a cuffed endotracheal tube. A toddler who swallowed drain cleaner is hospitalized for observation because of the risk for vomiting and aspiration. Over the next 24 hours the child does not exhibit any respiratory distress and does not vomit. At discharge the nurse emphasizes that the parents should monitor their child for the onset of: Gagging and vomiting. A nurse in the emergency department is caring for a 2-year-old child who was found by his parents crying and holding a container of toilet bowl cleaner. The child's lips are edematous and inflamed, and he is drooling. Which of the following is the priority action by the nurse? Check the child's respiratory status. A nurse is caring for a 12 year old adolescent who has ingested 60 mL of bleach. Which of the following statements by the nurse would indicate an understanding of this ingestion? the severity of alkaline burn depends of the pH of the substance. In case of poisoning from a bottle of cleaning liquid, save the bottle of cleaning liquid, call the poison control center for instructions. A nurse is providing anticipatory guidance about accidental ingestion of a toxic substance to the parents of a toddler. Which is an appropriate teaching point for the nurse to give the parents? call the poison control center. o Lead poisoning- A nurse is caring for a 3 year old child who has a lead level of 15 g/dL. When teaching the toddler's parents about nutrition and the correlation with lead poisoning, which of the following suggestions is appropriate for the nurse to state? drink fluids of any kind. A nurse is caring for an 18 month old who has been admitted for lead poisoning. An order for a urine specific gravity is written. Which of the following would be the appropriate way for the nurse to collect the urine? applying a pediatric urine collector. A nurse in a pediatric clinic is caring for a 3-year-old child who has a blood lead level of 3 mcg/dL. When teaching the toddler's parents about the correlation of nutrition with lead poisoning, which of the following information is appropriate for the nurse to include in the teaching? Ensure the child's dietary intake of calcium and iron is adequate. o Poison Ivy- remove the clothing over the rash, apply calamine lotion to the skin. ❖ Post-traumatic stress disorder (PTSD)- children can benefit from psychotherapy, this may manifest as a phobia, development of PTSD follows a traumatic event. ❖ Priority- Receiving change-of-shift report on 4 children. Which should be assessed 1st? A toddler who has a concussion and an episode of forceful vomiting. A nurse is planning care for a preschool-age child who has autism and is being admitted to the facility. Which actions should the nurse plan to take? Encourage the parent’s to bring in the child’s stuffed animal. ❖ Pyloromyotomy- A nurse is caring for a 6-week-old infant following a pyloromyotomy. Which of the following forms of feeding should the nurse anticipate for the infant 6 hour after the procedure? Small, frequent bottle feedings of electrolyte solution. ❖ Respiratory and breathing- respiratory distress manifests as tachycardia, diaphoresis, restlessness. Substernal retractions in a 2- wk-old infant is a priority to report to the provider. o A nurse is assessing an infant who has pneumonia. Which of the following findings is the priority for the nurse to report to MD? Nasal flaring. A nurse is assessing a 3-yo toddler at a well-child visit. Which of the following manifestations should the nurse report to the MD? Respiratory rate 45/min. A nurse is monitoring the oxygen saturation level of an infant using pulse oximetry. The nurse should secure the sensor to which of the following areas on the infant? Great toe. A toddler who was admitted in acute respiratory distress is now resting quietly. The parents tell the nurse that they must leave. What should the nurse suggest that the parents do? Plan to visit the child as frequently as possible. ❖ Reye’s Syndrome- risk factor is a recent episode of gastroenteritis, aspirin use. ❖ Rhabdomyosarcoma- manifestations are enlarged lymph nodes, pain, epistaxis, pain, palpable masses. ❖ Rheumatic fever- erythema marginatum (rash), elevated C-reactive protein are common manifestations. o A nurse is caring for a school-age child who has acute rheumatic fever. Which of the following actions should the nurse take? Maintain the child on bed rest. A parent tells the nurse in the emergency department, "My 3-year-old has had a fever for several days and has been vomiting." After prescribed measures to reduce the fever have been instituted, what nursing action is most important? Preventing shivering. A nurse is caring for a child who is admitted with swollen, painful joints and is diagnosed with rheumatic fever. When educating the child's parent about rheumatic fever, which of the following statements by the nurse would be appropriate? "It is preceded by a streptococcal infection." A nurse is teaching the parents of a child who has rheumatic fever. Which of statements by a parent indicates an understanding of the teaching? My child may take aspirin for joint pain. ❖ Safety- A nurse is teaching the parent of an infant about home safety. Which of the following information should the nurse include? Position the car seat so it is rear-facing. Secure a safety gate at the top and bottom of the stairs. Maintain the water heater temperature at 49 C (120 F). A nurse is planning care for a child who is autistic. Which of the following goals is of primary importance in the care of this child? To be protected from self-injury ❖ Salmonella- common cause of food poisoning. 1st sign will be confusion. This is a bacterial infection, bloody diarrhea is common, transmission can be from house pets. ❖ Scabies- the nurse will expect pencil-like marks on hands, blisters on the soles of the feet, pimples on the trunk. ❖ Scoliosis- these patient’s will receive spinal instrumentation as treatment for scoliosis. They will need to receive blood. o A school nurse is assessing an adolescent who has scoliosis. Which of the following findings should the nurse expect? a unilateral rib hump. A nurse is caring for a child with a Milwaukee brace for scoliosis. After educating the adolescent, the nurse evaluates the client understands the proper application and use of the brace. Which of the following statements should indicate to the nurse that the adolescent understands the use of the brace? I can take my brace off for about an hour to shower daily. A nurse is conducting a yearly health assessment of a 14 year old girl. The nurse should understand which of the following findings will require further evaluation? there is a lateral curvature to her spine. A nurse is providing teaching to an adolescent who has scoliosis and a new prescription for a Boston brace. Which of the following responses by the adolescent indicates an understanding of the teaching? I can take my brace off for about an hour daily to shower. ❖ Seborrheic Dermatitis- affects the scalp. You can use petroleum to help soften and remove patches from your infant’s scalp. ❖ Seizures and precautions- risk factors are febrile episodes, hypoglycemia, sodium imbalances. o Absence seizures- loss of consciousness, appearance of daydreaming, dropping help objects are expected findings. Generalized seizure- priority action is to maintain the child in a side-lying position. Implement seizure precautions for the infant when creating a plan of care for an infant who has an epidural hematoma with a skull fracture. An 18-month-old toddler who stepped on a rusty nail 4 days ago shows signs of generalized tetanus, including neck and jaw stiffness and facial muscle spasms. The toddler is receiving intravenous diazepam (Valium) as a muscle relaxant every 4 hours. What response to the medication does the nurse anticipate? Control of hypertonicity and prevention of seizures. A nurse is planning care for a school-age child who is in the oliguric phase of acute kidney injury (AKI) and has a sodium level of 129 mEq/L. Which of the following interventions should the nurse include in the plan? Initiate seizure precautions for the child. Tonic-clonic seizure- A nurse is caring for a school-age child who has experienced a tonic-clonic seizure. Which actions should the nurse take during the immediate postictal period? Place the child in a lateral position, on left side. When a child starts to experience a tonic-clonic seizure, the most appropriate action 1st is to assist child to side-lying position (sim’s) on the floor. Treatment- vagal nerve stimulator, additional antiepileptic medications, corpus callosotomy, focal resection. ❖ Shock- A nurse is assessing an 8-year-old child who has early indications of shock. After establishing an airway and stabilizing the child's respirations, which of the following actions should the nurse take next? Initiate IV access. ❖ Siblings- A mother in the postpartum unit expresses concern that her 3-year-old daughter will be jealous of her new brother. What should nurse suggest? Bring home a new doll for daughter when her baby brother is brought home. ❖ Sickle cell anemia- to decrease the risk of a vasooclusive crisis, provide adequate fluid intake throughout the day. Hemoglobin electrophoresis is performed to distinguish if the infant has the trait of the disease. o A nurse is preparing to collect a sample from a toddler for a sickle-turbidity test. Appropriate action to take? Perform a finger stick. Which of the following signs are indications of hydration status during a sickle cell crisis? Turgor of tissue, Texture of mucous membranes. A charge nurse is assigning rooms for admissions. An 8 year old child who is admitted with sickle cell anemia and is dehydrated. Which of the following is an appropriate room assignment for this child? 10-year-old male; postoperative appendectomy. A nurse is caring for an 8-year-old child who has sickle cell anemia. Which of the following actions should the nurse take? Give the child flavored popsicles. A nurse is caring for a child diagnosed with sickle cell anemia. The nurse should make which of the following recommendations to the client regarding sickle cell anemia? Increase fluid intake. A nurse on the pediatric unit is caring for four clients who all have assessments ordered in the morning. Which of the following values should the nurse report to a client's primary care provider immediately? Sickle cell anemia, urine specific gravity of 1.030. A nurse is reviewing the laboratory results of a child who has experienced diarrhea for the past 24 hr. Which of the following values for urine specific gravity should the nurse expect? 1.035. A nurse is planning care for an adolescent who has sickle cell anemia and is experiencing a vasoocclusive crisis. Which of the following interventions should the nurse include in the plan? Maintain the child on bed rest. Chronic vasooclusive crisis causes enlarged heart, enuresis, leg ulcers, retinal detachment. ❖ Skeletal Traction- Position a pressure reduction mattress under the back for a child in skeletal traction. A nurse is caring for a child in skeletal traction. At the change of shift, the nurse finds the client crying in pain, and the right foot is pale and pulseless. Which of the following should the nurse recognize as the appropriate explanation of this finding? This is a critically abnormal finding, and the primary care provider must be notified immediately. A nurse is caring for a child who is in skeletal traction. Which of the following actions is the nurse's priority? Encourage the child to use an incentive spirometer. A nurse is caring for an 8 year old who has fractured his femur. The child is in skeletal traction. To assist with the child's developmental needs, which of the following would be an appropriate action for the nurse to take? have the hospital tutor visit to assist the child with homework. Assess the client’s position frequently, assess pin sites every 4 hours, ensure the weights are hanging freely. o Buck's traction- A nurse is caring for a child who is in Buck's traction. Which of the following should the nurse recognize as an appropriate intervention to prevent complications? Provide small meals with high fiber. A nurse is caring for a child who has been in Buck's traction for 2 days. Which of the following actions should the nurse take to prevent complications? Check for pulses in the affected leg every 4 hours. ❖ Sleep- A nurse is taking a history during a routine physical exam. Which of the following would be appropriate to tell the parent? establish a set bedtime and follow a nightly routine. A nurse is providing teaching about promoting sleep with the parent of a 3- year-old toddler. Which information should the nurse include? Follow a nightly routine and established bedtime. ❖ Spinal fusion- I'll log roll the client every 2 hr. ❖ Strabismus- A nurse encourages parents to have their toddler's eyes tested especially for monocular strabismus. What should the nurse explain may occur if the condition is not corrected early? Amblyopia will progress in the weak eye. A nurse is assessing a 6-month-old infant at a well-infant visit. Which of the following findings should the nurse report to the provider? Presence of strabismus (should disappear at 3 to 4 months of age). ❖ Sudden infant death syndrome (SIDS)- A nurse is teaching the parent of a newborn about ways to prevent SIDS. Instructions to be included? "Give the infant a pacifier at bedtime." A nurse is providing anticipatory guidance to the parents of a 2-week-old infant about risk factors for sudden infant death syndrome (SIDS). Which of the following risk factors should the nurse include in the teaching? Covering the sleeping infant with a blanket ❖ Syndrome of inappropriate antidiuretic hormone secretion (SIADH)- A nurse is caring for a 15-year-old pt following a head injury. Which of the following findings should the nurse identify as an indication that the child is developing syndrome of inappropriate antidiuretic hormone secretion (SIADH)? Mental confusion. ❖ Teeth- A nurse is teaching the mother of a 6-month-old infant about teething. Which of the following statements should the nurse make? "Your baby may pull at her ears when she is teething.” A mother indicates to the nurse in the pediatric clinic that she is concerned that her 20-month-old son's bedtime thumb-sucking will cause his teeth to protrude. How should the nurse respond? "There is no reason to be concerned about the teeth protruding unless he keeps sucking his thumb after his permanent teeth have come in." ❖ Temper tantrums- can be reduced with the provision of a less stressful environment. Set limits and be consistent. ❖ Tension pneumothorax- respiratory distress, no breath sounds on one side, trachea that deviates away from the affected side. ❖ Terminal illness- impending death is evidenced by difficulty swallowing, Cheyne-Stokes respirations. Complicated grief- personal activities are affected when experiencing complicated grief. Preschool children perceive death as temporary. To maintain professional effectiveness with a dying child: remain in contact with the family after the loss, develop a professional support system, take time off from work. Assistive personal can say “I will listen and respond as the family talks about their child’s life.” A life threatening event warrants electroencephalogram, electrocardiogram, and blood cultures. o A nurse is caring for a preschool-age child who is dying. Which of the following findings is an age-appropriate reaction to death by the child? The child views death as similar to sleep. The child believes his thoughts can cause death. The child thinks death is a punishment. A nurse is caring for a child who is dying. The child's 4 year old sibling is visiting. Which of the following statements indicates a 4 year old's perception of death? death is the same as going to sleep, death is caused by magical thinking, death is the result of a wish, death is a punishment. ❖ Tetralogy of Fallot- knee-chest position decreases the return of desaturated venous blood from the legs & to direct more blood into the pulmonary artery by increasing systemic vascular resistance. o A nurse is caring for an infant who is receiving IV fluids for the treatment of Tetralogy of Fallot and begins to have a hypercyanotic spell. Which of the following actions should the nurse take? Place the infant in a knee-chest position. A nurse is caring for a child who has tetralogy of Fallot preoperatively. Which of following laboratory values should the nurse expect to find? Hematocrit of 58%. A nurse is caring for a child who has tetralogy of Fallot. Which of following laboratory values should the nurse expect to find? RBC 6.8 million. ❖ Thalassemia- A nurse is performing health screenings of toddlers in a culturally diverse neighborhood. Which child should the nurse consider at risk for β-thalassemia (Cooley anemia)? 2-year-old child of Greek descent with a large abdomen. A 2-year-old child is admitted to the pediatric unit with a diagnosis of thalassemia major (Cooley anemia). The parents are told that there is no cure but the anemia can be treated with frequent blood transfusions. The father tells the nurse he is glad that there is a treatment that "fixes" his child's problem. Before responding, the nurse should recall that blood transfusions: Correct the anemia but may cause other problems. A nurse is caring for a 6-month-old infant who has been diagnosed with thalassemia major. After providing a teaching plan, the nurse should recognize that the parent understands the disease process when the parent states which of the following? My infant will require frequent transfusions. ❖ Thought stopping- reduces painful stimuli by having child repeat memorized facts about the painful event. ❖ Thrombocytopenia- monitor for signs of bleeding, avoid peripheral venipunctures. ❖ Tinea Capitus- treat infected house pets, use Selenium Sulfide shampoo. Tinea pedis (athlete’s foot)- A nurse is providing teaching to an adolescent about how to manage tinea pedis. Which statements by the adolescent indicates an understanding of the teaching? "I should wear sandals as much as possible." ❖ Toilet training- A nurse is teaching the parents of a toddler who has cognitive impairment about toilet training. Instructions to include in the teaching? "Award the child with a sticker when he sits on the potty chair." When is a toddler considered ready for toilet training? When the child is able to sit, walk, and squat. When the child is capable of removing his or her own clothing. When the child is able to recognize the urge to defecate or urinate. A nurse plans to talk to the parents of a toddler about toilet training. What should the nurse tell the parents is the most important factor in the process of toilet training? Parents' attitude about it. During a nap, a 3-year-old hospitalized child wets the bed. What is the best response by the nurse? Change child's clothes without discussing the incident. ❖ Tonsillectomy- Activity should be limited to 10 days to decrease the risk of hemorrhage. Milk products (milkshakes) should be avoided because they coat the throat which can initiate the cough response and increase the risk of bleeding. Red & brown foods should also be avoided during the immediate postop period so that food and fresh or old bleed can be distinguished in the emesis. Administer analgesics on a schedule for the postoperative period. o A nurse is providing discharge teaching to the parent of a school-age child who has undergone a tonsillectomy. Which of the following statements by the parent should the nurse identify as understanding the teaching? "I will notify the doctor if I notice that my child is swallowing frequently. A nurse is caring for a child who has had a tonsillectomy. Which of the following findings should the nurse give the most attention to 8 hour after surgery? Frequent swallowing. ❖ Tracheoesophageal fistula- A nurse is caring for a newborn infant who is suspected of having a tracheoesophageal fistula (TEF). Which of the following nursing assessments would be consistent with this diagnosis? Copious oral secretions. A nurse is teaching about clinical manifestations of tracheomalacia to a parent of an infant who had tracheoesophageal fistula repair as a newborn. Which of the following findings should the nurse include in the teaching? Barking cough. ❖ Transfusions- A nurse is caring for a school-age child who is receiving a blood transfusion. Which manifestations should alert the nurse to a possible hemolytic transfusion reaction? flank pain (caused by breakdown of RBC's). ❖ Trauma care- following a motor vehicle crash, child is unresponsive, spontaneous respirations of 22/min, and a bleeding laceration on the forehead. The 1st action is to stabilize the child’s neck. ❖ Urinary tract infection- repeated cases indicates a need for parental education on cleaning of the perineal area carefully, at the time of each diaper change. To prevent UTI avoid bubble baths, empty bladder completely with each void, provide information about manifestations of infection, encourage frequent voiding. Enuresis- complication is emotional problems. Expected findings of UTI are irritability, vomiting, swelling of the face, pallor, fatigue, and fever. o A nurse is caring for a child who has frequent urinary tract infections. When educating the parent on the prevention of urinary tract infections, which of the following instructions should the nurse include in the teaching? Teach the child to wipe her perineum from front to back after urinating. A nurse is planning to collect a specimen from a male infant using a urine collection bag. Which of the following actions should the nurse take? Wash and dry the infant's genitalia and perineum thoroughly. ❖ Ventricular peritoneal shunt- The nurse is caring for a 3 year old post-op following revision of a malfunctioning ventricular peritoneal shunt. Which of the following would be an appropriate way for the nurse to determine if the child is in pain? use the FACES scale to rate the pain. A nurse is caring for a 4 year old child who has a malfunctioning ventricular peritoneal shunt. Following a new shunt placement, the nurse conducts a postoperative check. Which of the following assessments should the nurse immediately respond to? Sleepy, very difficult to arouse. ❖ Ventricular septal defect- a murmur is related to the left-to-right shunting of blood. A nurse is assessing an infant who has a ventricular septal defect. Which of the following findings should the nurse expect? Loud, harsh murmur. A nurse is caring for a 2 month old infant with a ventricular septal defect. Which of the following observations should indicate to the nurse that the child's condition is worsening? Weight gain of 275 g. A nurse is caring for a child with a ventricular septal defect. Which of the following should the nurse expect to assess in this child? Murmur best heard at the lower left sternal border. A nurse is assessing a 2-month-old infant who has a ventricular septal defect. Which of the following findings should the nurse report to the provider? Weight gain of 1.8 kg (4lb). A nurse is assessing a child who has a ventricular septal defect. Which of the following finding should the nurse expect? Murmur at the left sternal border. ❖ Vision- to perform a peripheral vison test on a child, have the child focus on an object while performing the test. ❖ Wheezes- high-pitched, musical or whistling like sounds heard primarily on expiration as air passes through and vibrates through narrow airways. Heard when auscultating the lungs of an adolescent who is experiencing dyspnea. ❖ Wilm’s Tumor- prepare these children for surgery which will occur within 48 hours of the patient being diagnosed. Further treatments will start immediately after surgery. NPO status is continued after surgery while there is absence of bowel sounds. o A nurse is creating a plan of care for a preschooler who has Wilm's tumor and is scheduled for surgery. Which of the following interventions should the nurse include? Avoid palpating the abdomen when bathing the child before surgery. A nurse is caring for a child who is diagnosed with Wilms' tumor. Which of the following interventions should the nurse do first? Place a sign over the bed that says "Do Not Palpate the Abdomen". [Show More]
Last updated: 1 year ago
Preview 1 out of 19 pages
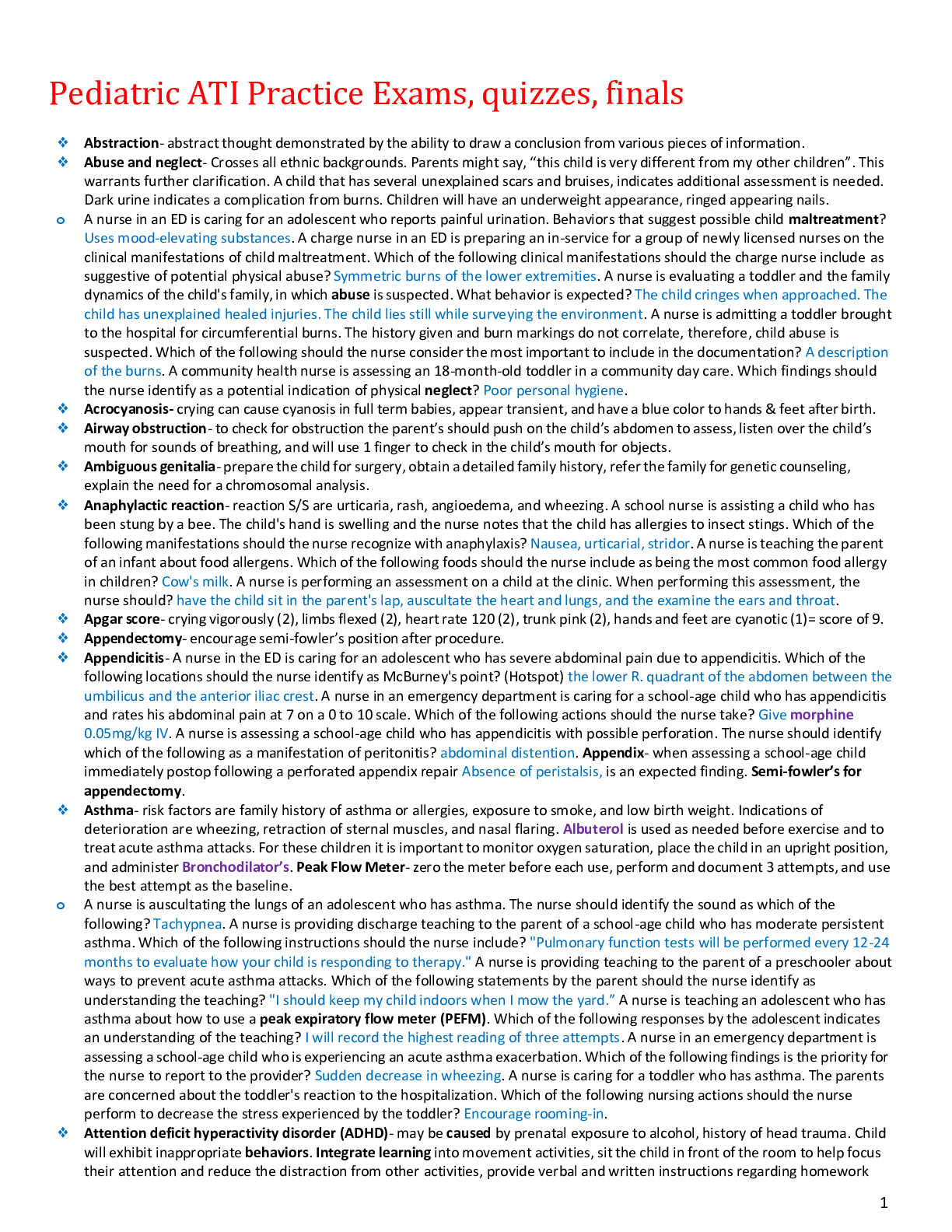
Reviews( 0 )
Document information
Connected school, study & course
About the document
Uploaded On
Jun 09, 2021
Number of pages
19
Written in

Additional information
This document has been written for:
Uploaded
Jun 09, 2021
Downloads
0
Views
117




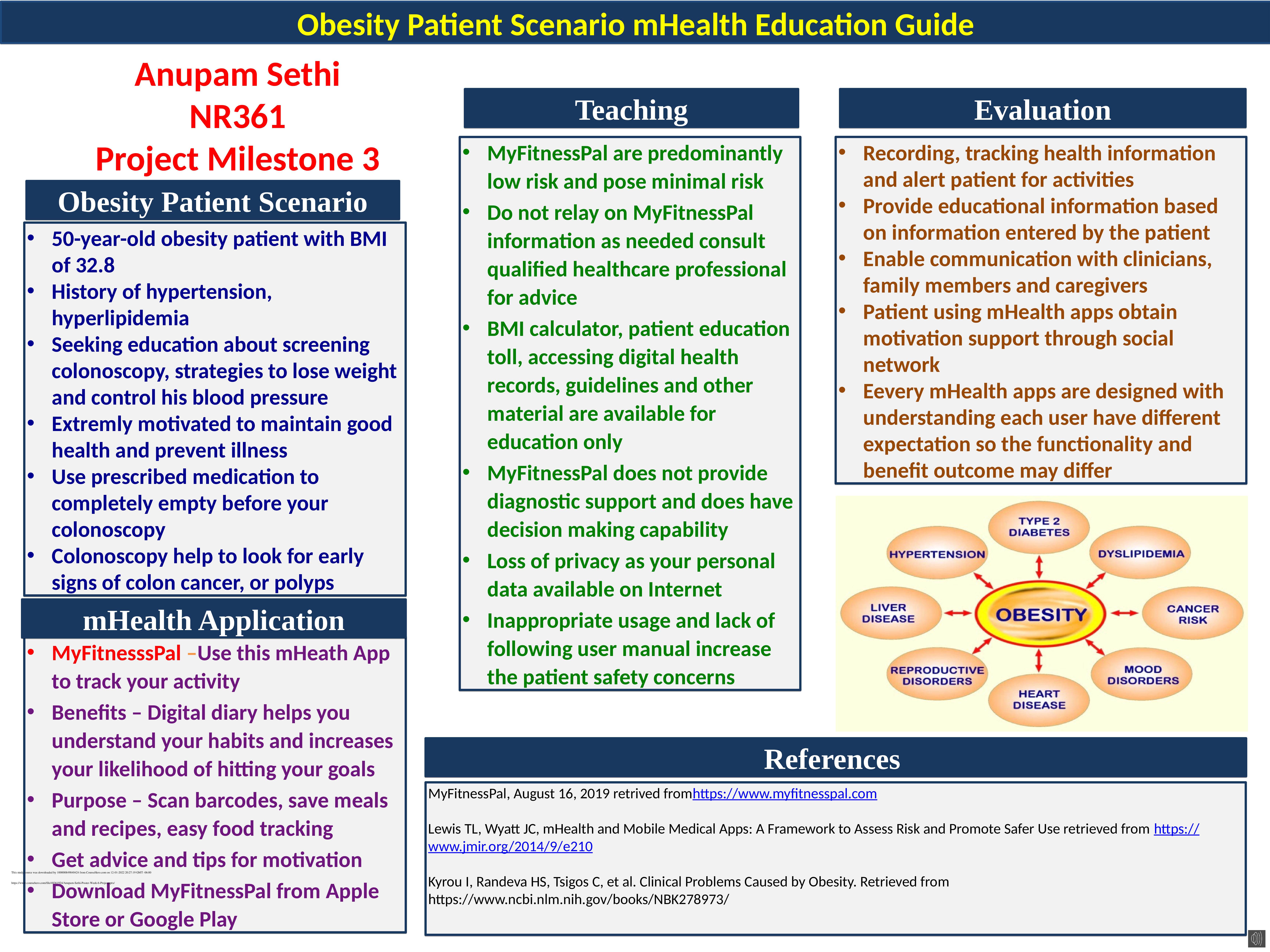

.png)


 (1).png)
.png)