*NURSING > STUDY GUIDE > NURS 4341 OB Exam 2 Study Guide - University of Texas, Arlington (All)
NURS 4341 OB Exam 2 Study Guide - University of Texas, Arlington
Document Content and Description Below
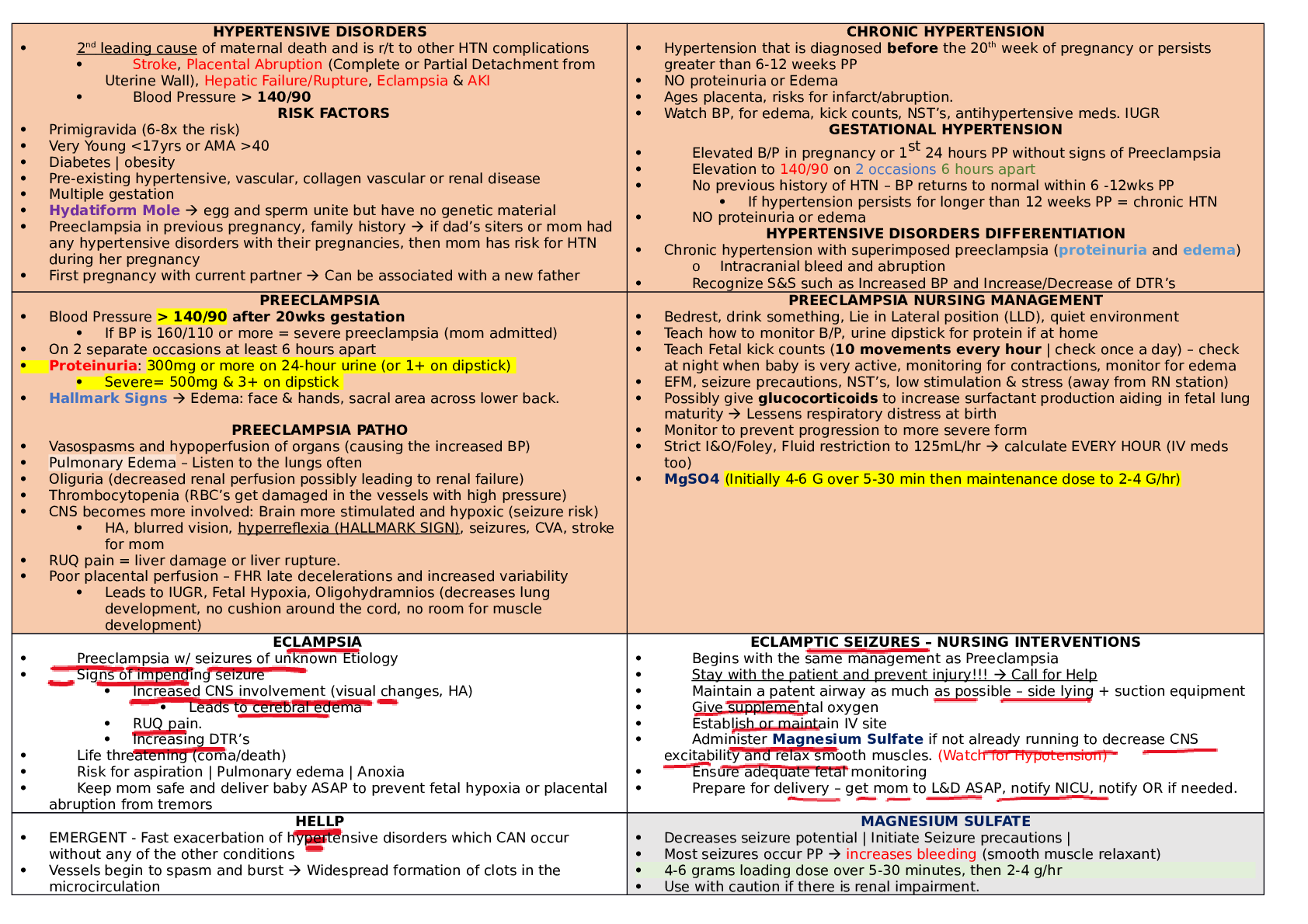
NURS 4341 OB Exam 2 Study Guide - University of Texas, Arlington HYPERTENSIVE DISORDERS 2nd leading cause of maternal death and is r/t to other HTN complications Stroke, Placental Abruption... (Complete or Partial Detachment from Uterine Wall), Hepatic Failure/Rupture, Eclampsia & AKI Blood Pressure > 140/90 RISK FACTORS Primigravida (6-8x the risk) Very Young <17yrs or AMA >40 Diabetes | obesity Pre-existing hypertensive, vascular, collagen vascular or renal disease Multiple gestation Hydatiform Mole egg and sperm unite but have no genetic material Preeclampsia in previous pregnancy, family history if dad’s siters or mom had any hypertensive disorders with their pregnancies, then mom has risk for HTN during her pregnancy First pregnancy with current partner Can be associated with a new father CHRONIC HYPERTENSION Hypertension that is diagnosed before the 20th week of pregnancy or persists greater than 6-12 weeks PP NO proteinuria or Edema Ages placenta, risks for infarct/abruption. Watch BP, for edema, kick counts, NST’s, antihypertensive meds. IUGR GESTATIONAL HYPERTENSION Elevated B/P in pregnancy or 1st 24 hours PP without signs of Preeclampsia Elevation to 140/90 on 2 occasions 6 hours apart No previous history of HTN – BP returns to normal within 6 -12wks PP If hypertension persists for longer than 12 weeks PP = chronic HTN NO proteinuria or edema HYPERTENSIVE DISORDERS DIFFERENTIATION Chronic hypertension with superimposed preeclampsia (proteinuria and edema) o Intracranial bleed and abruption Recognize S&S such as Increased BP and Increase/Decrease of DTR’s PREECLAMPSIA Blood Pressure > 140/90 after 20wks gestation If BP is 160/110 or more = severe preeclampsia (mom admitted) On 2 separate occasions at least 6 hours apart Proteinuria: 300mg or more on 24-hour urine (or 1+ on dipstick) Severe= 500mg & 3+ on dipstick Hallmark Signs Edema: face & hands, sacral area across lower back. PREECLAMPSIA PATHO Vasospasms and hypoperfusion of organs (causing the increased BP) Pulmonary Edema – Listen to the lungs often Oliguria (decreased renal perfusion possibly leading to renal failure) Thrombocytopenia (RBC’s get damaged in the vessels with high pressure) CNS becomes more involved: Brain more stimulated and hypoxic (seizure risk) HA, blurred vision, hyperreflexia (HALLMARK SIGN), seizures, CVA, stroke for mom RUQ pain = liver damage or liver rupture. Poor placental perfusion – FHR late decelerations and increased variability Leads to IUGR, Fetal Hypoxia, Oligohydramnios (decreases lung development, no cushion around the cord, no room for muscle development) PREECLAMPSIA NURSING MANAGEMENT Bedrest, drink something, Lie in Lateral position (LLD), quiet environment Teach how to monitor B/P, urine dipstick for protein if at home Teach Fetal kick counts (10 movements every hour | check once a day) – check at night when baby is very active, monitoring for contractions, monitor for edema EFM, seizure precautions, NST’s, low stimulation & stress (away from RN station) Possibly give glucocorticoids to increase surfactant production aiding in fetal lung maturity Lessens respiratory distress at birth Monitor to prevent progression to more severe form Strict I&O/Foley, Fluid restriction to 125mL/hr calculate EVERY HOUR (IV meds too) MgSO4 (Initially 4-6 G over 5-30 min then maintenance dose to 2-4 G/hr) [Show More]
Last updated: 11 months ago
Preview 1 out of 10 pages
Reviews( 0 )
Document information
Connected school, study & course
About the document
Uploaded On
May 01, 2023
Number of pages
10
Written in

Additional information
This document has been written for:
Uploaded
May 01, 2023
Downloads
0
Views
62