*NURSING > QUESTIONS & ANSWERS > Med Surg Exam 2 PDF - Summary Brunner and Suddarth's Textbook of Medical-Surgical Nursing: Med-Surg. (All)
Med Surg Exam 2 PDF - Summary Brunner and Suddarth's Textbook of Medical-Surgical Nursing: Med-Surg. Study Guide Exam 2
Document Content and Description Below
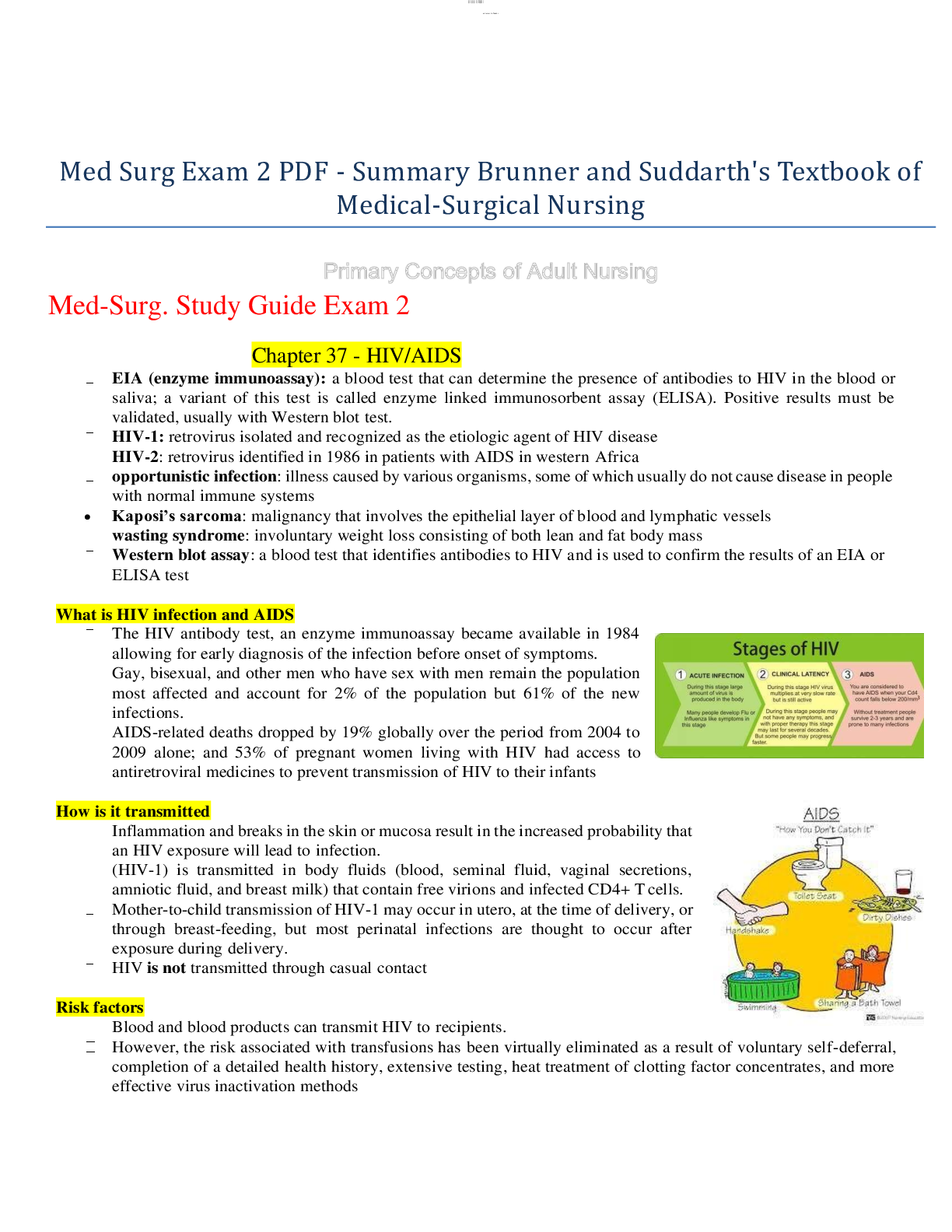
• EIA (enzyme immunoassay): a blood test that can determine the presence of antibodies to HIV in the blood or saliva; a variant of this test is called enzyme linked immunosorbent assay (ELISA). Posi... tive results must be validated, usually with Western blot test. What is HIV infection and AIDS • The HIV antibody test, an enzyme immunoassay became available in 1984 allowing for early diagnosis of the infection before onset of symptoms. How is it transmitted • Inflammation and breaks in the skin or mucosa result in the increased probability that an HIV exposure will lead to infection. Risk factors • Blood and blood products can transmit HIV to recipients. Health promotion • Nurses need to prevent HIV infection by educating how to eliminate or reduce risky behaviors All patients should be advised to: • Abstain from sharing sexual fluids (semen and vaginal fluid). • Reduce the number of sexual partners to one. Patients who are HIV seropositive should also be advised to: • Inform previous, present, and prospective sexual and drug-using partners of their HIV-positive status. Recommendations for standard precautions • ALWAYS follow standard precautions! • Standard precautions are designed to reduce the risk of transmission of blood-borne pathogens and of pathogens from moist body substances. HIV antibody test • When a person is infected with HIV, the immune system responds by producing antibodies against the virus, usually within 3 to 12 weeks after infection o Clinical manifestations • Patients with HIV/AIDS experience a number of symptoms related to the disease, side effects of treatment, and other comorbidities, o Candidiasis • Fungal infection, occurs in almost all patients with AIDS and immune depression. Oral candidiasis is characterized by creamy white patches in the oral cavity o Wasting Syndrome • AIDS wasting syndrome includes involuntary weight loss consisting of both lean and fat mass • The distinction between cachexia (wasting) and weight loss, is important, because the metabolic derangement o Kaposi’s Sarcoma • the most common HIV-related malignancy, is a disease that involves the endothelial layer of blood and lymphatic vessels. o Nursing process • Nursing assessment includes identification of potential risk factors, including a history of risky sexual practices or IV/injection drug use. Also, the pt.’s physical and psychological status are assessed o KEY TERMS • Allergen: Substance that causes manifestations of allergy. • Allergy: Inappropriate and often harmful immune system response to substances that are normally harmless. 3. Total Serum Immunoglobin E levels • High total serum IgE levels support the diagnosis of allergic disease. BUT a normal IgE levels does not exclude the diagnosis of an allergic disorder o What is the cause/Pathophysiology? • Caused by the interaction of a foreign antigen with specific IgE antibodies found on the surface membrane of mast cells and peripheral blood basophils KNOW DIFFERENCES BETWEEN LOCAL AND SYSTEMIC AND HOW TO TREAT THEM DIFFERENTLY o Non-allergic Anaphylaxis Reaction • Closely related to Anaphylaxis reaction o Clinical manifestations • Mild systemic reactions: Consist of peripheral tingling and a sensation of warmth, possibly accompanied by a sensation of fullness in the mouth and throat. Nasal o Common Causes of Anaphylaxis • Foods: Peanuts, tree nuts (e.g., walnuts, pecans, cashews, almonds), shell fish (e.g., shrimp, lobster, crab), fish, milk, eggs, soy, wheat o Medical management • Management depends on the severity of the reaction. Initially, respiratory and cardiovascular functions are evaluated o Nursing management • If a patient is experiencing an allergic response, the nurse’s initial action is to assess the patient for signs and symptoms of anaphylaxis o Rheumatoid Arthritis: Autoimmune disease of unknown origin. Affects more females than males. o Pathophysiology • The exact o Clinical Manifestations (She emphasized this) • The initial clinical manifestations of RA include symmetric joint pain and morning joint stiffness lasting longer than 1 hour. o Assessment and Diagnostic Findings • Several assessment findings are associated with RA: rheumatoid nodules, joint inflammation detected on palpation, and laboratory findings. o Medical Management • The goal of treatment at all phases of the RA disease process is to decrease joint pain and swelling, achieve clinical remission, decrease the likelihood of joint deformity, and minimize disability. Initial treatment delays have been implicated in greater long-term joint deformity. Aggressive and early treatment regimens are warranted. • Nutrition Therapy o Nursing Management • The most common issues for the patient with RA include pain, sleep disturbance, fatigue, altered mood, and limited mobility. The patient with newly diagnosed RA needs information about the disease to make daily self- management decisions and cope with having a chronic disease o Systemic Lupus Erythematosus • SLE is an inflammatory, autoimmune disorder that affects nearly every organ in the body. • Occurs more frequently in women than in men and occurs more in African American populations than among Caucasians o Pathophysiology • SLE starts with the body’s immune system inaccurately recognizing one or more components of the cell’s nucleus as foreign, seeing it as an antigen o Clinical manifestations • Systemic symptoms include fever, malaise, weight loss, and anorexia. o Assessment and diagnosis findings • Diagnosis of SLE is based on a complete history, physical examination, and blood tests. • The skin is inspected for erythematous rashes. Cutaneous erythematous plaques with an adherent scale may be observed on the scalp, face, or neck. o Medical management • Management of the more chronic condition involves periodic monitoring and recognition of meaningful clinical changes requiring adjustments in therapy. o Nursing management • The most common nursing diagnoses include fatigue, impaired skin integrity, body image disturbance, and deficient knowledge for self-management decisions. o Achalasia Chapters 44, 46, 47 Upper Gastrointestinal Disorders • Absent or ineffective peristalsis of the distal esophagus accompanied by failure of the esophageal sphincter to relax in response to swallowing o Hiatal Hernia • The opening in the diaphragm through which the esophagus passes becomes enlarged, and part of the upper stomach tends to move up into the lower portion of the thorax. o Clinical Manifestations • The patient with a sliding hernia may have heartburn, regurgitation, and dysphagia, but at least 50% of patients are asymptomatic. Sliding hiatal hernia is often implicated in reflux. o Management • Management for a hiatal hernia includes frequent, small feedings that can pass easily through the esophagus. • The patient is advised not to recline for 1 hour after eating, to prevent reflux or movement of the hernia, and to • Some degree of gastroesophageal reflux (GERD) (back flow of gastric or duodenal contents into the esophagus) is normal. o Management • Management begins with educating the patient to avoid situations that decrease lower esophageal sphincter pressure or cause esophageal irritation. Barrett’s Esophagus • Barrett’s esophagus is a condition in which the lining of the esophageal mucosa is altered. o Gastritis • Gastritis (inflammation of the gastric or stomach mucosa) is a common GI problem o Pathophysiology • In gastritis, the gastric mucous membrane becomes edematous and hyperemic (congested with fluid and blood) and undergoes superficial erosion o Clinical Manifestations • The patient with acute gastritis may have a rapid onset of symptoms, such as abdominal discomfort, headache, lassitude, nausea, anorexia, vomiting, and hiccupping, which can last from a few hours to a few days. o Assessment and Diagnostic Findings • Gastritis is sometimes associated with achlorhydria (lack of hydrochloric acid [HCl], hypochlorhydria (low levels of HCl), or hyperchlorhydria (high levels of HCl). o Nursing Management • Reducing Anxiety: If the patient has ingested acids or alkalis, emergency measures may be necessary. • Promoting Fluid Balance: The nurse must always be alert to any indicators of hemorrhagic gastritis, which include hematemesis (vomiting of blood), tachycardia, and hypotension. All stools should be examined for the presence of frank or occult bleeding. o PUD • A peptic ulcer may be referred to as a gastric, duodenal, or esophageal ulcer, depending on its location. o Pathophysiology • Peptic ulcers occur mainly in the gastroduodenal mucosa because this tissue cannot withstand the digestive action of gastric acid (HCl) and pepsin. o Clinical Manifestations • Symptoms of an ulcer may last for a few days, weeks, or months and may disappear only to reappear, often without an identifiable cause o Assessment and Diagnostic Findings • A physical examination may reveal pain, epigastric tenderness, or abdominal distention. o Medical Management • Recurrence may develop; however, peptic ulcers treated with antibiotics to eradicate H. pylori have a lower recurrence rate than those not treated with antibiotics. SHE SAID NOT TO FOCUS TOO MUCH ON THIS, JUST TO KNOW THAT IF THE PATIENT’S STOLL WAS BRIGH RED THEN IT WAS LOWER GI AND IF IT WAS BLACK THEN IT WAS UPPER GI • Hemorrhage Gastritis and hemorrhage from peptic ulcer are the two most common causes of upper GI tract bleeding. Hemorrhage, the most common complication NOT TOO MUCH FOCUS ON BARIATRIC SURGERY OR OBESITY Obesity o Bariatric Surgery • Bariatric surgery, or surgery for obesity, is performed only after other nonsurgical attempts at weight control have failed. o Clinical Manifestations • Vague epigastric or periumbilical pain (i.e., visceral pain that is dull and poorly localized) progresses to right lower quadrant pain (i.e., parietal pain that is sharp, discrete, and well localized) and is usually accompanied by a low-grade fever and nausea and sometimes by vomiting. o Assessment and Diagnostic Findings • CBC: elevated WBC, elevated neutrophils. (Normal 4.500 to 11000) • Abdominal x- ray films, ultrasound studies, and CT scans may reveal a right lower quadrant density or localized distention of the bowel. o Medical Management • Immediate surgery if appendicitis is diagnosed • Conservative nonsurgical medical management for uncomplicated appendicitis (i.e., absence of perforation of the appendix, empyema or abscess formation, or fecal peritonitis o Nursing Management • Goals include relieving pain, preventing fluid volume deficit (give IV fluids), reducing anxiety, eliminating infection due to the potential or actual disruption of the GI tract, maintaining skin integrity, and attaining optimal nutrition. • The patient may be discharged on the day of surgery if the temperature is within normal limits, there is no undue discomfort in the operative area, and the appendectomy was uncomplicated. Discharge o Diverticular Disease • A diverticulum is a saclike herniation of the lining of the bowel that extends through a defect in the muscle layer. • Diverticula may occur anywhere in the small intestine o Clinical Manifestations • Chronic constipation often precedes the development of diverticulosis by many years. o Assessment and Diagnostic Findings • Diverticulosis is typically diagnosed by colonoscopy, which permits visualization of the extent of diverticular disease and biopsy of tissue to rule out other diseases. o Complications • Frequently, the inflammation is not localized, and the entire abdominal cavity shows evidence of widespread infection. o Medical Management • Fluid, colloid, and electrolyte replacement is the major focus of medical management. o Nursing Management • Intensive care is often needed. Monitor frequently BP, central venous pressure, or pulmonary pressure, I&O. • In addition, ongoing assessment of pain (nature of the pain, location, and any change in location), GI function, and F&E balance is important. o Crohn’s Disease (Regional Enteritis) • Crohn’s disease is usually first diagnosed in adolescents or young adults but can appear at any time of life. The incidence of Crohn’s disease has risen over the past 30 years. o Assessment and Diagnostic Findings • A procto-sigmoidoscopy is usually performed initially to determine whether the recto-sigmoid area is inflamed. • A stool examination is also performed; the result may be positive for occult blood and steatorrhea o Ulcerative Colitis • Ulcerative colitis is a recurrent ulcerative and inflammatory disease of the mucosal and submucosal layers of the colon and rectum. o Pathophysiology • Ulcerative colitis affects the superficial mucosa of the colon and is characterized by multiple ulcerations, diffuse inflammations, and desquamation or shedding of the colonic epithelium. o Clinical Manifestations • The clinical course is usually one of exacerbations and remissions. o Assessment and Diagnostic Findings • The patient should be assessed for tachycardia, hypotension, tachypnea, fever, and pallor. Other assessments address the level of hydration and nutritional status. o What is intestinal Obstruction? Intestinal obstruction exists when blockage prevents the normal flow of intestinal contents through the intestinal tract. Two types of processes can impede this flow: o Pathophysiology • Large bowel obstruction results in an accumulation of intestinal contents, fluid, and gas proximal to the obstruction o Clinical Manifestations • The symptoms of large bowel obstruction differ from the small that the symptoms develop and progress relatively slowly. o Medical Management • Restoration of intravascular volume, correction of electrolyte abnormalities, and nasogastric aspiration and decompression are instituted immediately. o Nursing Intervention • The nurse’s role is to monitor the patient for symptoms indicating that the intestinal obstruction is worsening and to provide emotional support and comfort. [Show More]
Last updated: 1 year ago
Preview 1 out of 28 pages
Instant download
Buy this document to get the full access instantly
Instant Download Access after purchase
Add to cartInstant download
Reviews( 0 )
Document information
Connected school, study & course
About the document
Uploaded On
Apr 24, 2020
Number of pages
28
Written in

Additional information
This document has been written for:
Uploaded
Apr 24, 2020
Downloads
0
Views
205