*NURSING > STUDY GUIDE > C475_ CARE OF THE OLDER ADULT | CHAPTEER 2 - The Aging Population | (Gerontology, AGING, Senescence) (All)
C475_ CARE OF THE OLDER ADULT | CHAPTEER 2 - The Aging Population | (Gerontology, AGING, Senescence) | Complete Study Guide
Document Content and Description Below
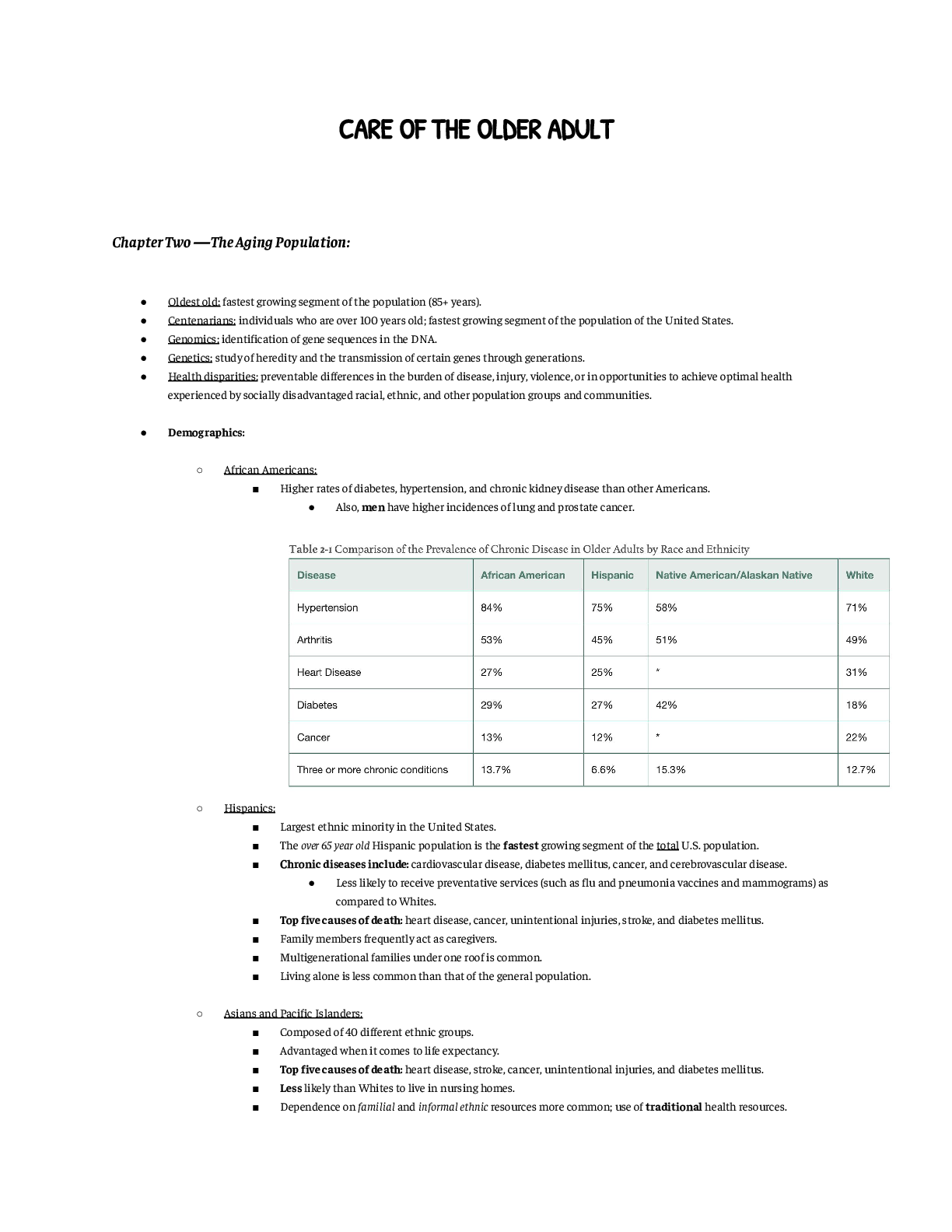
Chapter Two ― The Aging Population: ● Oldest old: fastest growing segment of the population (85+ years). ● Centenarians: individuals who are over 100 years old; fastest growing segment of ... the population of the United States. ● Genomics: identification of gene sequences in the DNA. ● Genetics: study of heredity and the transmission of certain genes through generations. ● Health disparities: preventable differences in the burden of disease, injury, violence, or in opportunities to achieve optimal health experienced by socially disadvantaged racial, ethnic, and other population groups and communities. ● Demographics: ○ African Americans: ■ Higher rates of diabetes, hypertension, and chronic kidney disease than other Americans. ● Also, men have higher incidences of lung and prostate cancer. ○ Hispanics: ■ Largest ethnic minority in the United States. ■ The over 65 year old Hispanic population is the fastest growing segment of the total U.S. population. ■ Chronic diseases include: cardiovascular disease, diabetes mellitus, cancer, and cerebrovascular disease. ● Less likely to receive preventative services (such as flu and pneumonia vaccines and mammograms) as compared to Whites. ■ Top five causes of death: heart disease, cancer, unintentional injuries, stroke, and diabetes mellitus. ■ Family members frequently act as caregivers. ■ Multigenerational families under one roof is common. ■ Living alone is less common than that of the general population. ○ Asians and Pacific Islanders: ■ Composed of 40 different ethnic groups. ■ Advantaged when it comes to life expectancy. ■ Top five causes of death: heart disease, stroke, cancer, unintentional injuries, and diabetes mellitus. ■ Less likely than Whites to live in nursing homes. ■ Dependence on familial and informal ethnic resources more common; use of traditional health resources. ■ Length of the family’s time in this country affects comfort and ease of resource use. ○ Native Americans and Alaskan Natives: ■ Comprised of 566 nations, tribes, bands, and native villages where 150 languages are used. ■ Larger families, less health insurance, and twice the level of poverty. ■ Population is younger than all other groups. ■ Life expectancy lags behind the national average. ■ Leading causes of death: heart disease, cancer, unintentional injuries, diabetes mellitus, and cerebrovascular disease. ■ Traditionally live in rural areas. ■ Higher rates of hypertension, diabetes mellitus, back pain, and vision loss; highest rates of diabetes in the U.S.; also has higher rates of obesity, substance abuse, and mental health issues. ● These are related to geographic isolation, economic factors, and traditional spiritual beliefs. ● More than two in five elders has diabetes mellitus. ■ Disability is one of the strongest predictors of the need for nursing home admission in older adults. ○ Living Arrangements: ■ Independent living: living alone or with their spouse only. ● Far more common in developed countries. ■ Living arrangements are linked to: income, health status, culture, and the availability of caregivers. ○ U.S. Veterans: ■ Three cohorts: ● Those who served in World War II. ● Those who served in the Korean War. ● Those who served in Vietnam. ● Mortality and Morbidity: ○ Chronic Diseases: ■ Six of the seven leading causes of death among older Americans are chronic diseases such as heart disease, stroke, cancer, and diabetes. ● Gender component; older women report higher incidence of hypertension and arthritis, whereas men report more heart disease and cancer. ■ Obesity. ■ Sensory impairments and oral health problems. ■ Decline in memory, particularly short-term memory. ○ Causes of Death: ■ The leading cause was diseases of the heart, followed by malignant neoplasms, chronic lower respiratory diseases (CLRD), accidents, cerebrovascular diseases, Alzheimer’s disease, diabetes, and influenza and pneumonia. ■ Death rates among older males were higher than among females for heart disease, cancer, CLRD, diabetes, stroke, and unintentional injuries. ■ Death rates for Alzheimer’s disease were lower among males than females. ● Globally, heart disease is followed by a cause of death by stroke, pulmonary disease, HIV/AIDS, diabetes, Alzheimer’s disease, diarrheal diseases, tuberculosis, and injury. Chapter Three ― Theories of Aging: ● Psychosocial Theories of Aging: ○ Focus on changes in behavior, personality, and attitude as we age. ○ Sociological Theories of Aging: ■ Activity Theory: ● Retirees remain active in their communities. ● Published by Havighurst and Albrecht. ○ Staying occupied and involved is necessary to having a satisfying late-life. ● Maddox suggested that leisure time in retirement presents new opportunities for community service that may be more consistent with physical, economic, and resource limitations. ● Birren and Schroots assert that roles assumed by older adults are highly influenced by societal expectations so that older adults may be limited in what activities they can choose. ● Central theme is that remaining active in old age is desirable. ○ Older adults viewed the quality of activity is more important than the quantity. ● Type of activity matters; activities that connect people socially are more likely to improve life satisfaction. ■ Disengagement Theory: ● Published by Cumming and Henry. ● Aging is characterized by gradual disengagement from society and relationships. ○ This separation is desired by society and older adults and it serves to maintain social equilibrium. ○ By disengaging, they are freed from social responsibilities and gain time for internal reflection. ○ The outcome is a new equilibrium that is ideally satisfying. ● Rapkin and Fisher challenged this theory. ○ Demographic disadvantaged and age-related transitions were related to a greater desire for disengagement, support, and stability. ○ Elders who were married and healthy were more likely to report a desire for an energetic lifestyle. ● Adams supported this theory. ○ Instrument to measure change in activity among older adults. ● One example of the restrictions society can pose on older adult activity is the Social Security laws that reduce payment to older adults who make more than a set income. ■ Subculture Theory: ● Theorized by Rose. ○ Older adults form a unique subculture within society to defend against society’s negative attitude toward aging and the accompanying loss of status. ○ Older adults prefer to interact among themselves. ○ Social status is determined more by health and mobility than occupation, education, or income. ■ Older adults have a social disadvantage regarding status and associated respect because of the functional decline that comes with aging. ■ Continuity Theory: ● Theorized by Havighurst. ○ Personality influences the roles we choose and how we enact them; this in turn influences satisfaction with living. ○ Personality is well developed by the time we reach old age and tends to remain consistent throughout time. ○ Four personality types: integrated, armored-defended, passive-dependent, unintegrated. ■ Integrated: have adjusted well to aging, as evidenced by activity engagement that may be broad (reorganizers), more selected (focused), or disengaged. ■ Armored-defended: tend to continue the activities and roles held during middle age. ■ Passive-dependent: either highly dependent or exhibit disinterest in the external world. ■ Unintegrated (least well-adjusted): fail to cope with aging successfully. ○ Adjusting to physical, financial, and social decline; contemplating death; and developing a personal and meaningful perspective on the end of life are the t asks of older adulthood. ■ Identifying with one’s age group, finding a living environment that is compatible with physical functioning, and learning new societal roles postretirement. ● These provide clues as to how one will adjust to changes in health, environment, or socioeconomic conditions, and in what activities they will engage. ● First sociological theory to acknowledge that responses to aging differ among people. ■ Age Stratification Theory: ● Examined the interdependence between older adults and society. ● Riley theorized this theory. ○ Society is stratified into different age categories that are the basis for acquiring resources, roles, status, and deference from others in society. ○ Age cohorts are influenced by the historical context in which they live and can vary among generations. ■ People born in the same cohort have similar experiences, ideologies, orientations, attitudes, and values as well as expectations regarding the timing of life transitions. ● Highlighted the importance of cohorts and the associated socioeconomic and political impact on how individuals age. ■ Person-Environment-Fit Theory: ● Theorized by Lawton. ○ Capacity to function in one’s environment is an important aspect of successful aging, and that function is affected by ego strength, motor skills, biologic health, cognitive capacity, and sensori-perceptual capacity., as well as external conditions imposed by the environment. ■ Functional capacity influences the ability to adapt to the environment. ● Those functioning at lower levels can tolerate fewer environmental demands. ■ Gerotranscendence Theory: ● Theorized by Tornstam. ○ Aging individuals undergo a cognitive transformation from a materialistic, rational perspective toward “oneness” with the universe. ○ Characteristics of a successful transformation: ■ A more outward or external focus. ■ Accepting impending death without fear. ■ An emphasis on substantive relationships. ■ A sense of connectedness with preceding and future generations. ■ Spiritual unity with the universe. ○ Social disengagement is not a necessary and natural development. ■ Activity and participation must be the result of one’s own choices and that control over one’s life in all situations is essential for successful adaptation to aging. ○ Psychological Theories of Aging: ■ Human Needs Theory: ● Theorized by Maslow. ○ Hierarchy of five needs motivates human behavior: ■ Physiologic. ■ Safety and security. ■ Love and belonging. ■ Self-esteem. ■ Self-actualization. ○ More basic needs such as physioligcal functioning or safety take precedence over personal growth needs (love and belonging, self-esteem, self-actualization). ○ Movement is multidirectional. ○ Failure to grow leads to feelings of failure, depression, and the perception that life is meaningless. ■ Theory of Individualism: ● Theorized by Jung. ● Is not specific to aging. ○ Our personality develops over a lifetime and is composed of an ego or self-identity that has a personal and collective unconsciousness. ○ Personal unconsciousness is the private feelings and perceptions surrounding important persons or life events. ■ The collective unconscious is shared by all persons. ● It contains latent memories about human origin. ● The collective unconscious is the foundation of personality on which the personal unconsciousness and ego are built. ○ People tend to view life through either their own “lens” (introverts) or the lens of others (extroverts). ○ One ages successfully when they accept the past, adapt to physical decline, and cope with the loss of significant others. ■ Stages of Personality Development Theory: ● Theorized by Erikson. ● SEE BOOK PAGE 48. ■ Life-Course (Life Span Development) Theory: ● The concept “life course,” in which life, which is unique to each individual, is divided into stages with predictable patterns. ● Is concerned with understanding age group norms and their characteristics. ● Encompass aspects of psychological theories such as tasks during different stages of personality development with sociological tenets regarding the interconnectedness of individuals and society. ● Central theme is that life occurs in stages that are structured according to one’s roles, relationships, internal values, and goals. ○ Goal achievement is linked to life satisfaction; people’s goals are limited by external factors. ○ Successful adaptation to life changes may require revising one’s beliefs to be consistent with society’s expectations. ■ Selective Optimization with Compensation Theory: ● Theorized by Baltes. ○ Individuals learn to cope with the functional losses of aging through the processes of selection, optimization, and compensation. ○ Adjust activities and roles as limitations present themselves; at the same time, they choose those activities and roles that are most satisfying (optimization). ○ Coping with illness and functional decline may lead to greater or lesser risk of mortality. ■ Ideally, selective optimization with compensation is a positive coping process that facilitates successful aging. ● Biological Theories of Aging: ○ Explain the physiologic processes that change with aging. ○ Some aging theorists divide the biological theories into two categories: ■ 1) A stochastic or statistical perspective, which identifies episodic events that happen throughout one’s life that cause random cell damage and accumulate over time, thus causing aging. ■ 2) The nonstochastic theories, which view aging as a series of predetermined events happening to all organisms in a timed framework. ○ Stochastic Theories: ■ Free Radical Theory: ● Aging is due to oxidative metabolism and the effects of free radicals. ● Emphasizes the significance of how cells use oxygen. ○ Free radicals react with proteins, lipids, DNA, and RNA causing cellular damage. ■ This damage accumulaets over time and is thought to accelerate aging. ● Free radicals cause: ○ Extensive cellular damage to DNA, which can cause malignancy and accelerated aging due to oxidative modification of proteins that impact cell metabolism ○ Lipid oxidation that damages phospholipids in cell membranes, thus affecting membrane permeability ○ DNA strand breaks and base modifications that cause gene modulation ● Cellular membrane damage causes other chemicals to be blocked from their regular receptor sites, thus mitigating other processes crucial to cell metabolism. ○ Mitochondrial deterioration due to oxidants causing a significant loss of cell energy and greatly decreases cell metabolism. ○ Ames and Harman suggested strategies to assist in delaying the mitochondrial delay, such as: ■ Decrease calories in order to lower weight ■ Maintain a diet high in nutrients, including antioxidants ■ Avoid inflammation ■ Minimize accumulation of metals in the body that can trigger free radical reactions ○ Older adult is more vulnerable to free radical damage because free radicals are attracted to cells that have transient or interrupted perfusion. ■ Oxidative damage increases with age. ■ Orgel/Error Theory: ● Over time, cells accumulate errors in their DNA and RNA protein synthesis that cause the cells to die. ● Aging would not occur if destructive factors such as radiation did not exist and cause “errors” such as mutations and regulatory disorders. ■ Wear and Tear Theory: ● Over time, cumulative changes occuring in cells age and damage cellular metabolism. ● Cells in the heart muscle, neurons, striated muscle, and the brain cannot replace themselves once being destroyed by wear and tear. ○ Excessive wear and tear caused by exercising may accelerate aging by increasing free radical production. ■ Connective Tissue Theory: ● Also referred to as the cross-link theory. ● Over time, biochemical processes create connections between structures not normally connected. ○ Several occur rapidly between 30 and 50 years of age. ● Elastin dries up and cracks with age; hence, skin with less elastin tends to be drier and wrinkled. ● Over time, because of decreased extracellular fluid, numerous deposits of sodium, chloride, and calcium build up in the cardiovascular system. ○ Nonstochastic Theories: ■ Programmed Theory: ● As people age, more of their cells start to decide to commit suicide or stop dividing. ● The Hayflick phenomenon, or the human fibroblast replicative senescence model. ○ Cells divide until they can no longer divide, whereupon the cell’s infrastructure recognizes this inability to further divide and triggers the apoptosis sequence of the cell. ● Cells have a finite doubling potential and become unable to replicate after they have done so a number of times. ● Human cells age each time they replicate because of the shortening of the telomere. ○ Normal human cells do not have telomerase. ■ Gene/Biological Clock Theory: ● Each cell, or perhaps the entire organism, has a genetically programmed aging code that is stored in the organism’s DNA. ● Slagboom theorized this theory. ○ Theory described as comprising genetic influences that predict physical condition, occurrence of disease, cause and age of death, and other factors that contribute to longevity. ● Theory indicates that there may be genes that trigger youth and general well-being as well as other genes that accelerate cell deterioration. ■ Neuroendocrine Theory: ● Describes a change in hormone secretion, as with the releasing hormones of the hypothalamus and the stimulating hormones of the pituitary gland, which manage the thyroid, parathyroid, and adrenal glands, and how it influences the aging process. ● The following major hormones are involved with aging: ○ Estrogen decreases the thinning of bones, and when women age, less estrogen is produced by the ovaries. As women grow older and experience menopause, adipose tissue becomes the major source of estrogen. ○ Growth hormone is part of the process that increases bone and muscle strength. Growth hormone stimulates the release of insulin-like growth factor produced by the liver. ○ Melatonin is produced by the pineal gland and is thought to be responsible for coordinating seasonal adaptations in the body. ● There is a higher chance of excess or loss of glucocorticoids, aldosterone, androgens, triiodothyronine, thyroxine, and parathyroid hormone when the hypothalamus-pituitary-endocrine gland feedback system is altered. When the stimulating and releasing hormones of the pituitary and the hypothalamus are out of synch with the endocrine glands, an increase in disease is expected in multiple organs and systems. Of significance are the findings of Rodenbeck and Hajak, who cited that, with physiological aging and also with certain psychiatric disorders, there is increased activation of the hypothalamus-pituitary-adrenal axis, which causes increased plasma cortisol levels. The increased cortisol levels can be linked with several diseases. ■ Immunologic/Autoimmune Theory: ● Normal aging process of humans and animals as being related to faulty immunological function. ○ There is decreased immune function in elderly due to: ■ The thymus gland shrinking. ■ Altered lymphocyte function. ■ Decreased cell mediated and humoral immune response. ○ There is loss of T-cell differentiation, so body incorrectly perceives old, irregular cells as foreign bodies and attacks them. ○ There is an increase in certain autoantibodies such as rheumatoid factor and a loss of interleukins. ● Implications for Nursing: ○ Nursing Theories of Aging: ■ Functional Consequences Theory: ● Developed to provide a guiding framework for older adults with physical impairment and disability. ● Created by Miller. ○ Aging adults experience environmental and biopsychosocial consequences that impact their functioning. ● Nurse’s Role is To: ○ Assess age-related changes and accompanying risk factors. ○ To design interventions that minimize age-associated disability. ● Goal: maximize functioning in ways that improve patient safety and quality of life. ○ Quality of life, functional capacity and dependency are connected and that positive consequences are possible despite age-related limitations. ■ Theory of Thriving: ● Explains the experience of nursing home residents. ● Newbern and Krowchuk suggested that difficulty with social relationships (disconnectedness and inability to find meaning in life, give of oneself, or attach to others) and physical/cognitive dysfunction (consistent unplanned weight loss, signs of depression, and cognitive decline) were related to a failure to thrive. ■ Theory of Successful Aging: ● Flood proposed that aging well is defined by the extent to which older adults adapt to the cumulative physical and functional changes they experience. Moreover, a person’s perception about how well he or she has aged is fundamentally connected to believing that one’s life has meaning and purpose; thus, spirituality is a central ingredient of Floods theory. ● Flood proposed that: ○ Aging is a progressive process adaptation. ○ Aging may be successful or unsuccessful, depending upon a person’s ability to cope. ○ Successful aging is influenced by a person’s choices. ○ Aging people experience changes, which uniquely characterize their beliefs and perspectives in ways that differ from those of younger adults. ● According to this theory, aging successfully means remaining physically, psychologically, and socially engaged in meaningful ways that are individually defined. Achieving a comfortable acceptance of impending death is also a hallmark of successful aging. Chapter Five ― Teaching and Communication with Older Adults: ● Language for Improving Communication with Older Adults:: ○ Building Trust and Respect: ■ Avoiding elderspeak. ■ Pay attention to the nonverbal. ■ Partnering Communication Model: ● Tell the [patient] your name and your role as you sit at eye level. ● Ask the patient his or her priorities for the day so you can assist him or her in meeting these goals. ● Let the patient know what your practice needs are during your shift and look at integrating your needs and the patient’s needs for the day. ● Put your name, contact number [how to reach you], and partnered goals on the whiteboard [or other visible area]. ● Continue with the five Ps: ○ You did partnering already ○ Ask about the restroom needs—potty ○ Obtain a pain assessment ○ Make positioning adjustments. ○ Check the pump(s) to reduce potential noise distractions. ● Address pain or your first assessment of the day and do both soon. ● Before leaving, ask if there is anything he or she needs before you leave to finish your regular rounds. ■ Partnering Communication: ● Use first-person language. ● Include the patient. ● Speak slower and pause between phrases. ● Provide additional time for the person to respond. ● Simplify vocabulary and avoid jargon. ● Use short, direct, clear phrases. ● Use appropriate touch to communicate. ● Speak in the direction of the person. ● Speak into the ear with less or no hearing loss. ● Write out information. ● Provide written information in large, easy-to-read print. ● Request clarification. ● Encourage use of clues. ● Eliminate or minimize background noise. ● Limit the number of speakers. ● Position yourself in the person’s direct line of vision. ● Use gestures to aid in communication. ● Say names. ● Make sure any assistive devices are on and working. [Show More]
Last updated: 1 year ago
Preview 1 out of 10 pages
Instant download
Buy this document to get the full access instantly
Instant Download Access after purchase
Add to cartInstant download
Reviews( 0 )
Document information
Connected school, study & course
About the document
Uploaded On
May 25, 2021
Number of pages
10
Written in

Additional information
This document has been written for:
Uploaded
May 25, 2021
Downloads
0
Views
35