*NURSING > STUDY GUIDE > NUR Med Surg 2 Assessment of neuro system/ Study guide/ Download to Score A+ (All)
NUR Med Surg 2 Assessment of neuro system/ Study guide/ Download to Score A+
Document Content and Description Below
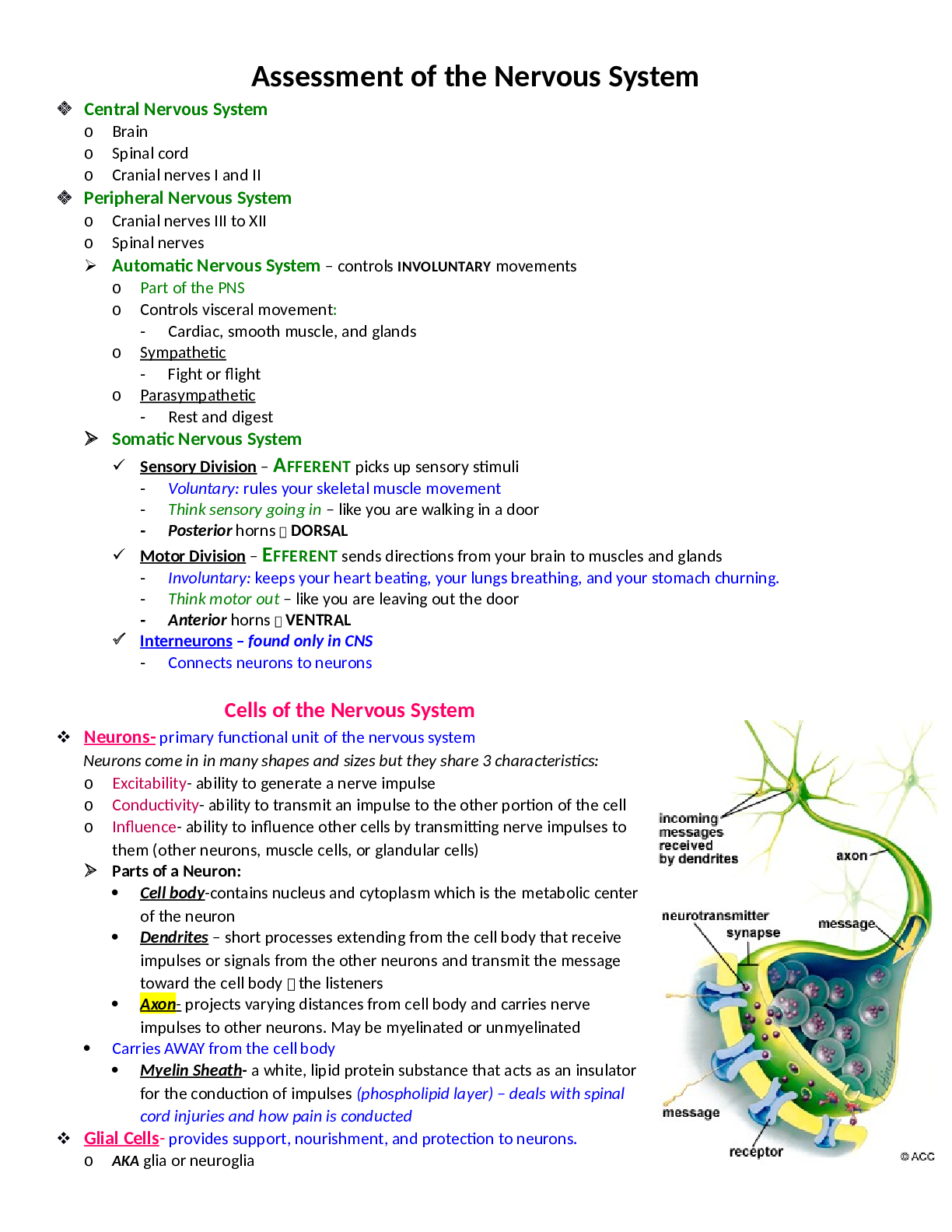
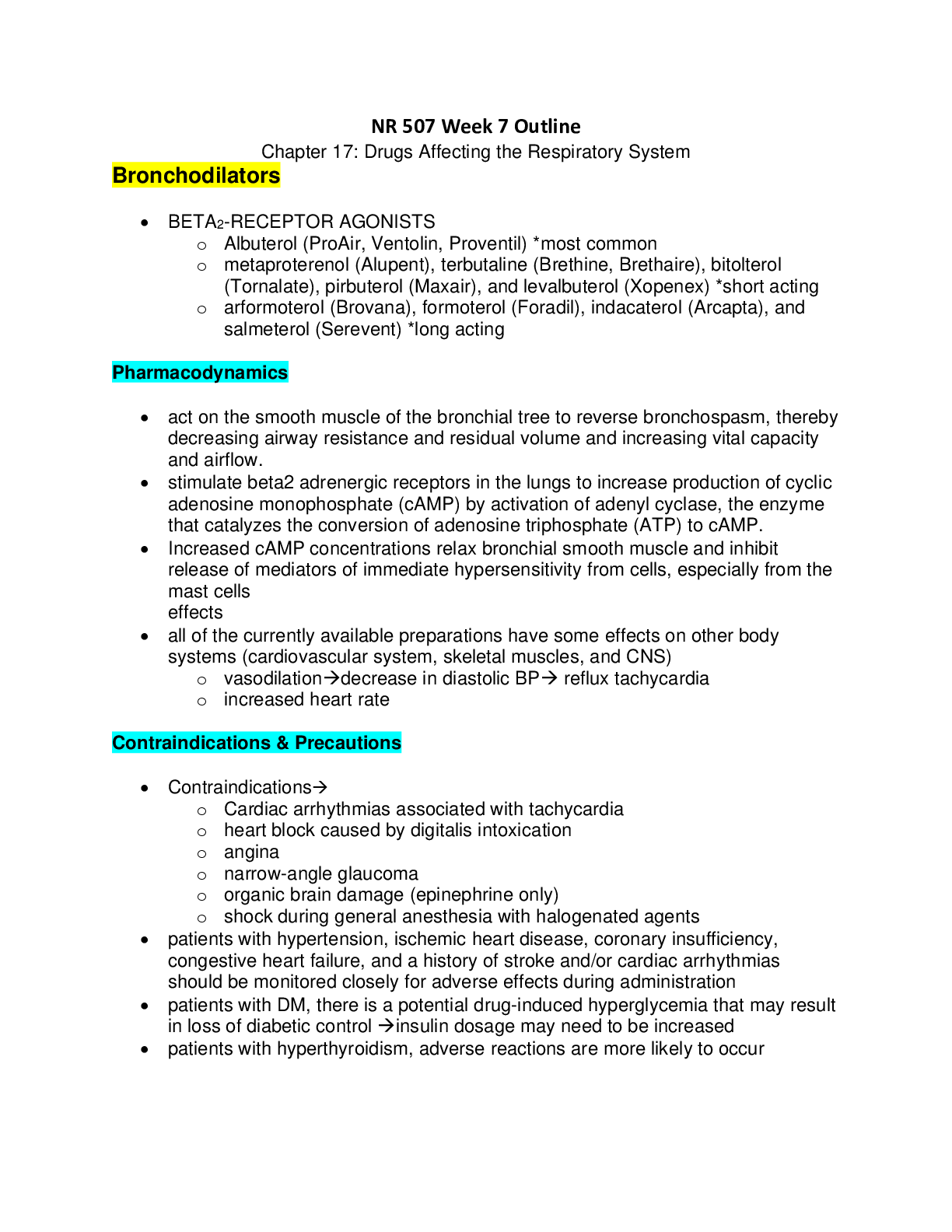
Assessment of the Nervous System ❖ Central Nervous System o Brain o Spinal cord o Cranial nerves I and II ❖ Peripheral Nervous System o Cranial nerves III to XII o Spinal nerves ➢ Automa... tic Nervous System – controls INVOLUNTARY movements o Part of the PNS o Controls visceral movement: - Cardiac, smooth muscle, and glands o Sympathetic - Fight or flight o Parasympathetic - Rest and digest ➢ Somatic Nervous System ✓ Sensory Division – AFFERENT picks up sensory stimuli - Voluntary: rules your skeletal muscle movement - Think sensory going in – like you are walking in a door - Posterior horns DORSAL ✓ Motor Division – EFFERENT sends directions from your brain to muscles and glands - Involuntary: keeps your heart beating, your lungs breathing, and your stomach churning. - Think motor out – like you are leaving out the door - Anterior horns VENTRAL ✓ Interneurons – found only in CNS - Connects neurons to neurons Cells of the Nervous System ❖ Neurons- primary functional unit of the nervous system Neurons come in in many shapes and sizes but they share 3 characteristics: o Excitability- ability to generate a nerve impulse o Conductivity- ability to transmit an impulse to the other portion of the cell o Influence- ability to influence other cells by transmitting nerve impulses to them (other neurons, muscle cells, or glandular cells) ➢ Parts of a Neuron: • Cell body-contains nucleus and cytoplasm which is the metabolic center of the neuron • Dendrites – short processes extending from the cell body that receive impulses or signals from the other neurons and transmit the message toward the cell body the listeners • Axon- projects varying distances from cell body and carries nerve impulses to other neurons. May be myelinated or unmyelinated • Carries AWAY from the cell body • Myelin Sheath- a white, lipid protein substance that acts as an insulator for the conduction of impulses (phospholipid layer) – deals with spinal cord injuries and how pain is conducted ❖ Glial Cells- provides support, nourishment, and protection to neurons. o AKA glia or neuroglia o Constitute almost half the brain and spinal cord mass. o Mitotic and can replicate. o In general, when neurons are destroyed, the tissue is replaced by the proliferation of neuroglial cells. o Most primary CNS tumors involve glial cells. o Primary malignancies involving neurons are rare. Divided into: o Microglial cells- specialized macrophages capable of phagocytosis, protect the neurons - Mobile within the brain and multiply when the brain is damaged o Macroglial cells- include astrocytes, oligodendrocytes, and ependymal cells ▪ Astrocytes - Usually found in GRAY MATTER and provide structural support o Gray matter lower than white matter - Form the blood-brain barrier - Play a role in synaptic transmission - When brain is injured they act like phagocytes and clean up neuronal debris - Help restore the neurochemical milieu and provide support for repair - Proliferation of astrocytes contributes to the formation of scar tissue (gliosis) in the CNS ▪ Oligodendrocytes - Specialized cells that produce the myelin sheath of nerve fibers in the CNS - Found primarily in the WHITE MATTER of the CNS o White matter is faster than gray matter • Schwann cells- myelinate the nerve fibers in the periphery • Ependymal cells- line the brain ventricles and aid in the secretion of CSF Nerve Regeneration • Reconstruction and renewal of cell structure and function, generally restrict to the myelin • If the axon of the nerve cell is damaged, the cell attempts to repair itself • Damaged nerve cells attempt to grow back to their original destinations by sprouting many branches from the damaged ends of their axons • Axons in the CNS can’t regenerate as much as peripheral axons b/c they are outside of the brain & spinal cord. • Injured nerve fibers in the PNS can regenerate by growing within the protective myelin sheath of the supporting Schwann cells if the cell body is intact and the environment is optimal - The final result of nerve regeneration depends on the number of axon sprouts that join and restore • A subset of glial cells astrocytes proliferate (reproduce) after certain injuries in the CNS o Neurogenesis may occur from stem cells. Nerve Impulse – DON’T NEED TO KNOW IN DEPTH • The purpose of a neuron is to initiate, receive, and process messages about events inside and outside the body • Neuronal message= nerve impulse that involves a generation of an action potential o A series of action potentials travels along the axon until it reaches the end and is transmitted across the junction between the nerve cells by a chemical reaction involving neurotransmitters (synapse) • Many peripheral nerve axons have Nodes of Ranvier- gaps in the myelin sheath that allow action potential to travel much faster by jumping from node to node o Saltatory- hopping of nodes • Synapse- the structural and functional junction between two neurons, the location at which the nerve impulse is transferred o Essential structures of synaptic transmission are a presynaptic terminal, synaptic cleft, and receptor site on the postsynaptic cell • Neurotransmitters- chemicals that affect the transmission of impulses across the synaptic cleft o Excitatory neurotransmitters- activate the postsynaptic receptors that INCREASE the likelihood that an action potential will be generated (epinephrine, norepinephrine, glutamate) o Inhibitory neurotransmitters- activates postsynaptic receptors to DECREASE the likelihood of an action potential being generated. o Neurotransmitters can be affected by drugs and toxins which can modify their function or block their attachment to receptor sites on the postsynaptic membrane o Endorphins block pain transmission o Substance P makes nerves more sensitive to pain o A presynaptic cell that releases an excitatory neurotransmitter does not always cause the postsynaptic cell to depolarize enough to generate an action potential. o Can be affected by drugs and toxins – modify or block their function on the postsynaptic membrane Central Nervous System • Components include: Cerebrum (cerebral hemispheres), brainstem, cerebellum, and spinal cord ➢ The spinal cord is continuous with the brainstem and exits from the cranial cavity through the foramen magnum. • Surrounded my CSF o Series of spinal segments, one on top of another with no visisble boundaries. In addition to cell bodies, each segment contains a pair of DORSAL (afferent) sensory nerve fibers or roots and VENTRAL (efferent) motor fibers or roots. o Gray matter centrally located (H shape) surrounded by white matter ▪ Gray matter contains the cell bodies of VOLUNTARY motor neurons, preganglionic autonomic motor neurons, and association neurons (interneurons) ▪ White matter contains the axons of the ascending sensory and descending sensory motor neurons Ascending Tracts ▪ From body upward to brain – sensory (pain, touch, joint position, skin temp) ▪ Information comes from special sensory receptors in the skin, muscles, and joints, viscera, and blood vessels and enters the spinal cord by way of the dorsal roots of the spinal nerves. ▪ Fasciculus gracilis and fasciculus cuneatus (commonly called dorsal –upper side– or posterior columns) - Carry info concerned with touch, deep pressure, vibration, position sense, and kinesthesia – appreciation of movement, weight, and body parts ▪ Spinocerebellar tracts - Carry information about muscle tension and body position to the cerebellum for coordination of movement ▪ Spinothalamic tracts - Carry pain and temperature sensations Descending Tracts ▪ Descending from the brain down to initiate the movement and to control body functions ▪ Corticobullar and corticospinal tracts pyramidal tract (responsible for fine skilled movements) - These carry voluntary (volitional) impulses from the cerebral cortex to the cranial and peripheral nerves ▪ The motor output exits the spinal cord by way of the ventral (under side) roots of the spinal nerves Reflex Arc ▪ Involuntary response to stimuli. ▪ Important role in maintaining muscle tone, which is essential for body posture ▪ Monosynaptic reflex arc include: - Receptor organ, afferent neuron, effector neuron, and effector organ. Lower and Upper Motor Neurons ▪ Upper motor neurons originate in the cerebral cortex and project downward. - Corticobullar tract ends in the brainstem - Corticospinal tract descends into the spinal cord - These neruons influence skeletal muscle movement ✓ SPASTICITY & HYPERACTIVE reflexes are caused by upper motor neuron damage ▪ Lower Motor Neurons final common pathways through which descending motor tracts influence skeletal muscle - Cell bodies send axons to stimulate the skeletal muscles - These cell bodies and their axons make up the somatic motor components of cranial nerves ✓ Cell bodies of lower motor neurons are located in the spinal cord, damage to the neuron will DECREASE motor activity of the affected muscles. Regions 7 Cervical spine – allow for flexion, extension, bending & turning of the head 12 Thoracic spine – attached to the ribs, good for movement and rotation, also protects major organs 5 Lumbar spine – movement for bending forward and extending backwards 5 Sacrum – lower back pain, tailbone 4 Coccyx ➢ The Cerebrum is the largest part of the brain and is composed of right and left hemispheres. o Divided into 4 lobes – Frontal, Temporal, Parietal, and Occipital o Gray matter OUTER layer of the cerebral hemispheres and consists of unmyelinated nerve fibers o White matter INNER layer of the cerebrum and consists of myelinated nerve fibers o When you have a stroke it crisscross (right sided stroke deficient on the left side b/c of synapse) Four Lobes of the Brain • The cerebral hemispheres have distinct fissures, which divide the brain into lobes. • Each hemisphere has 4 lobes: o Frontal, temporal, parietal, and occipital • Each lobe may be divided, once again, into areas that serve very specific functions. • It’s important to understand that each lobe of the brain does not function alone. • There are very complex relationships between the lobes of the brain and between the right and left hemispheres. Frontal Lobe • Personality, behavior, emotions • Judgment, planning, problem solving, reasoning, memory • Speech- speaking, and writing (Broca’s area) - expressive language 1. Expressive aphasia partial loss of the ability to produce language (spoken, manual, or written) 2. Nursing Interventions: Be patient, pen and paper, boards in the room, express pain? Use the faces • Body movement (motor strip) – motor skills • Intelligence, higher level of cognition, concentration, self-awareness Parietal Lobe (middle) • Interprets language, words • SENSORY • Sense of touch, pain, temperature - Doesn’t feel certain pain (cant feel burns, be careful w/ cooking) • Interprets signals from vision, hearing, motor, sensory and memory • Spatial and visual perception Occipital Lobe (back) • Interprets vision (color, light, movement) • Assess cranial nerves 3,4,6 PERRLA, EOM • Problem: Cant read! Temporal Lobe (lower) • Understanding written and oral language (Wernicke’s area)- receptive speech • Visual and auditory input for language comprehension. • Memory • Hearing sounds – auditory cortex • BALANCE - Romberg test • Sequencing and organization • Problem: tinnitus • Nursing Interventions: visual, flash cards, safety Right Brain – Left Brain • The right and left hemispheres of the brain are joined by a bundle of fibers called the corpus callosum that delivers messages from one side to the other. • Each hemisphere controls the opposite side of the body. o If a brain tumor is located on the right side of the brain, your left arm or leg may be weak or paralyzed. • Not all functions of the hemispheres are shared. • The LEFT hemisphere o Speech, comprehension, arithmetic, writing, logic, words, numbers, analysis, sequence • The RIGHT hemisphere o Controls creativity, spatial ability, artistic, musical skills, rhythm, wholeness, daydreaming, imagination ➢ The Cerebellum is located under the cerebrum and near the brainstem o Posterior cranial fossa inferior to the occipital lobe o Its function is to coordinate VOLUNTARY muscle movements and motor skills, maintain posture (trunk stability), and balance (equilibrium), as well as eye movement o Receives info from the cerebral cortex, muscles, joints, and inner ear o PROBLEM- lack of coordination – assessed by looking at the patient’s gait and the finger-to-nose test o Pronator drift!! ➢ The Brainstem includes the midbrain, pons, and medulla. o Located directly above the spinal cord o It performs many automatic functions such as breathing, consciousness, heart rate, body temperature, wake and sleep cycles, digestion, sneezing, coughing, vomiting, and swallowing. o Ascending and descending fibers to and from the cerebrum and cerebellum pass through the brainstem ▪ It acts as a relay center connecting the cerebrum and cerebellum to the spinal cord. o Midbrain smallest region of the brain – mediates pupillary reflexes and eye movements. Breathing station of auditory and visual information o Pons connects medulla to cerebellum. Helps regulate respirations, mediates chewing, taste, saliva secretion, hearing and helps coordinate movement on each side of body o Medulla Joins the spinal cord at the level of the foramen magnum. Influences respiratory, vasomotor (Blood Pressure), and cardiac function. It’s the center for vomiting, coughing, and hiccupping reflexes o Ten of the twelve cranial nerves originate in the brainstem CRANIAL NERVE 3 - 12 o Reticular Formation ▪ A diffusely arranged group of neurons and their axons that extends from the medulla to the thalamus and hypothalamus ▪ Reticular activating system (RAS)- a complex system that require communicating among the brainstem, reticular formation, and cerebral cortex. - Responsible for: regulating arousal in the sleep-wake cycle. Involved with motivation and alertness - attention Ventricles and Cerebrospinal Fluid • Ventricles are 4 fluid filled cavities deep within the brain that connect with the spinal canal • The lower portion of the fourth ventricle becomes the central canal in the lower part of the brainstem • Cerebrospinal fluid is produced largely in the choroid plexus of the brain within the ventricles • The choroid plexus- located in the walls inside the ventricles, ribbon-like structure that makes clear colorless cerebrospinal fluid o Produced at an average of 500mL/day o The ventricles and central canal are filled with an average of 150mL at any given time • CSF circulates in the subarachnoid space that surrounds the brain, brainstem, and spinal cord o Provides cushioning for the brain and spinal cord from physical shock o Helps cushion from injury w/ the environment o Stabilizes chemical environment o Allows fluid shifts from the cranial cavity to the spinal cavity o Carries nutrients o Removes waste from nervous tissue • CSF is absorbed through the arachnoid villi, then goes into the venous system - This circulating fluid is constantly being absorbed and replenished. o Excessive buildup of CSF is known as hydrocephalus • Analysis of CSF is useful diagnostic info related to certain nervous system diseases - It is measured in patients with actual or suspected intracranial injury • Herniation Syndrome- Increased ICP can force downward herniation of the brain and brainstem. DID YOU KNOW.. *Messages within the brain are carried along pathways. *Messages can travel from one gyrus to another, from one lobe to another, from one side of the brain to the other, and to structures found deep in the brain (e.g. thalamus, hypothalamus). Deep Structures in the Cerebrum Hypothalamus o Located just below the thalamus and slightly in front of the midbrain. o It is the master control of the autonomic system. o It plays a role in controlling behaviors such as hunger, thirst, sleep, and sexual response. o It also regulates body temperature, blood pressure, emotions, and secretion of hormones from the pituitary glands o Hormones regulated by hypothalamus: ▪ TSH, GH, LH, Prolactin-releasing hormone Pituitary gland o Lies in a small pocket of bone at skull base – sella turcica o The pituitary gland is connected to the hypothalamus of the brain by the pituitary stalk. Known as the “master gland,” it controls other endocrine glands in the body. - It secretes hormones that control sexual development, promote bone and muscle growth, respond to stress, and fight disease. Pineal gland o Is located behind the third ventricle. o It helps regulate the body’s internal clock and circadian rhythms by secreting melatonin. o It has some role in sexual development. Thalamus o Lies directly above the brainstem o Serves as a relay station for almost all information that comes and goes to the cortex plays a role in pain sensation, attention, alertness and memory. o Major relay center for sensory input from the body, face, retina, and cochlear and taste receptors Basal ganglia o Group of structures located centrally in the cerebrum and midbrain. Most of them are on both sides of the thalamus o Includes the caudate, putamen and globus pallidus. o These nuclei work with the cerebellum to coordinate fine motions, such as fingertip movements. o Function includes initiation, execution, and completion of voluntary movements, learning, emotional response, and automatic movements (swallowing, blinking, and swinging arms when walking) Limbic system o Located near the inner surface of the cerebral hemispheres o Is the center of our emotions, aggression, feeding behavior, sexual response, learning, and memory. o Included in this system are: the cingulate gyri, hypothalamus, amygdala (emotional reactions) and hippocampus (memory) Peripheral Nervous System Spinal Nerves – combination of motor and sensory nerves [31 PAIRS] o VOLUNTARY Motor System ▪ IN anterior horn of the spinal cord ▪ Gray matter ▪ LIFTING LEG UP o INVOLUNTARY (autonomic) Motor System ▪ IN anterolateral portion of the spinal cord ▪ Gray matter ▪ DIGESTION, BREATHING o Sensory Fibers ▪ Dorsal root ganglia just OUTSIDE the spinal cord o On exiting the spinal column, each spinal nerve divides into ventral and dorsal rami, a collection of motor and sensory fibers that eventually goes to peripheral structures (e.g skin, muscles, viscera) ❖ Dermatomes • An area of the skin innervated (stimulated) by the sensory fibers of a single dorsal root of a spinal nerve • Gives a general picture of somatic sensory innervation by spinal segments. ❖ Myotome a muscle group innervated by the primary motor neurons of a single ventral root. Cranial Nerves • The brain communicates with the body through the spinal cord and 12 PAIRS of cranial nerves • 10 out of 12 pairs of cranial nerves (3 to12) that control hearing, eye movement, facial sensations, taste, swallowing and movement of the face, neck, shoulder and tongue muscles originate in the brainstem. • The other 2 cranial nerves (1- 2) for smell and vision originate in the cerebrum. • All the cell bodies (nuclei) are in the brainstem o Except olfactory (nasal epithelium) and optic (retina) Autonomic Nervous System • Governs involuntary functio cardiac muscle, smooth (inv muscle, and glands • Divided into 2 components t function together to maintain balance ○ Sympathetic – “fight or flight” ▪ Preganglionic cell bodies located in the spinal segments T1-L2 adrenergic fibers is norepinephrine ▪ Neurotransmitter released by the postganglionic ▪ Neurotransmitter released by preganglionic cholinergic fibers is acetylcholine ○ Parasympathetic – “rest and digest” ▪ Preganglionic cell bodies located in the brainstem and sacral spinal segments S2-S4 ▪ Neurotrans. released @ BOTH pre/postganglionic cholinergic fibers is acetylcholine Cerebral Circulation Blood Supply • Blood is carried to the brain by TWO PAIRED ARTERIES - Supplies the pons and cerebellum (ischemic strokes) o Internal carotid arteries- ANTERIOR circulation ▪ Provides blood flow to the most anterior and middle portions of the cerebrum o Vertebral Arteries- POSTERIOR circulation ▪ Joins the ICA to form the basilar artery and provide blood flow to the brainstem, cerebellum, and posterior cerebrum • After passing through the skull, the right and left vertebral arteries join to form the basilar artery. o The Circle of Willis (green circle)- is formed by communicating arteries that join the basilar and internal carotid arteries o Basilar artery & INCA “communicate” with each other here. o The communication between the internal carotid and vertebral- basilar systems is an important safety feature of the brain. • If one of the major vessels becomes blocked, it is possible for collateral blood flow to come across the Circle of Willis and prevent brain damage. • Superior to the circle of Willis, THREE pairs of arteries supply blood to the left and right hemispheres 1. Anterior Cerebral Artery (ACA) - Feeds the medial and anterior portions of the frontal lobes - Feeds the frontal area, lower extremities, medial surface of frontal lobe, parietal lobe and part of the Corpus Callosum - Example: TOUCH LOWER EXTREMITIY – COLD 2. Middle Cerebral Artery (MCA) - Feeds the outer portions of the frontal, parietal, and superior temporal lobes - Feeds the brain which controls the face, head, and upper extremities - Example: TOUCH UPPER EXTREMITY - COLD 3. Posterior Cerebral Artery (PCA) - Feeds the medial portions of the occipital and inferior temporal lobes • Venous Blood o Drains from the brain through the Dural sinuses, which from channels that drain into the two jugular veins. • Blood-Brain Barrier o Physiologic barrier between blood capillaries and brain tissue o If we let everything in infection can occur!! o Protects the brain from harmful agents, while allowing nutrients and gases to enter o LIPID-SOLUBLE compounds enter the brain EASILY o WATER-SOLUBLE and IONIZED DRUGS enter the brain SLOWLY Top view of the Circle of Willis • The internal carotid and vertebral-basilar systems are joined by the anterior communicating and posterior communicating arteries. • The venous circulation of the brain is very different from that of the rest of the body. • Usually arteries and veins run together as they supply and drain specific areas of the body. o So, one would think there would be a pair of vertebral veins and internal carotid veins. However, this is not the case in the brain. The major vein collectors are integrated into the dura to form venous sinuses - not to be confused with the air sinuses in the face and nasal region. • The venous sinuses collect the blood from the brain and pass it to the internal jugular veins. • The superior and inferior sagittal sinuses drain the cerebrum, the cavernous sinuses drain the anterior skull base. • All sinuses eventually drain to the sigmoid sinuses, which exit the skull and form the jugular veins. o These two jugular veins are essentially the only drainage of the brain. Three quarter view of the Dural covering of the brain depicts the two major Dural folds, the falx and tentorium along with the venous sinuses. Language • In general, the left hemisphere of the brain is responsible for language and speech and is called the "dominant" hemisphere. • In about one third of individuals who are left-handed, speech function may be located on the right side of the brain. • Left-handed individuals may need special testing to determine if their speech center is on the left or right side prior to any surgery in that area. o Aphasia is a disturbance of language affecting production, comprehension, reading or writing, due to brain injury – most commonly from stroke or trauma. o The type of aphasia depends on the brain area affected. • Broca’s area lies in the left frontal lobe o If this area is damaged, one may have difficulty moving the tongue or facial muscles to produce the sounds of speech. o The individual can still read and understand spoken language but has difficulty in speaking and writing (i.e. forming letters and words, doesn't write within lines) – called Broca's aphasia. • Wernicke's area lies in the left temporal lobe o Damage to this area causes Wernicke's aphasia. Memory o The individual may speak in long sentences that have no meaning, add unnecessary words, and even create new words. They can make speech sounds; however, they have difficulty understanding speech and are therefore unaware of their mistakes. • Memory is a complex process that includes three phases: encoding (deciding what information is important), storing, and recalling. • Different areas of the brain are involved in memory depending on the type of memory. • Short-term memory- o Also called working memory, occurs in the prefrontal cortex. o It stores information for about one minute and its capacity is limited to about 7 items. o For example, it enables you to dial a phone number someone just told you. o It also intervenes during reading, to memorize the sentence you have just read, so that the next one makes sense. • Long-term memory- o Is processed in the hippocampus of the temporal lobe o Is activated when you want to memorize something for a longer time. o This memory has unlimited content and duration capacity. o It contains personal memories as well as facts and figures. • Skill memory- o Is processed in the cerebellum, which relays information to the basal ganglia. o It stores automatic learned memories like tying a shoe, playing an instrument, or riding a bike. Protective Structures Meninges – DON’T NEED TO GO IN DEPTH • The brain and spinal cord are covered and protected by three layers of tissue called meninges. • The dura mater is a strong, thick, tough, flexible membrane that closely lines the inside of the skull and protects the brain from displacing itself (bump your head, your brain wont move) o There are two special Dural folds falx and the tentorium. o The falx cerebri – separates the right and left hemispheres of the brain o The tentorium cerebelli – separates the cerebral hemispheres from the posterior fossa contains brainstem and cerebellum (separates the cerebrum and cerebellum) • The arachnoid mater is a thin, web-like membrane that covers the entire brain b/w the dura and pia mater. Hugs brain and spinal cord, though not as precisely as the pia mater o The arachnoid is made of elastic tissue. o Between the arachnoid mater & the pia mater is filled w/ CSF o The space between the dura and arachnoid membranes is called the subdural space. • The pia mater inner surface of the brain following its folds and grooves. o The pia mater has many blood vessels that reach deep into the brain (most vascular innermost later of meninges) o Subarachnoid space ▪ Area between the arachnoid layer and pia mater ▪ It is here where the cerebrospinal fluid bathes and cushions the brain – filled with CSF ▪ Arteries, veins, and cranial nerves passing to and from the brain and skull must pass through ▪ Region of the 3rd and 4th lumbar vertebrae used to obtain CSF during lumbar puncture Skull o Protects the brain from external trauma o Composed of 8 CRANIAL BONES and 14 FACIAL BONES o Many ridges, prominences, and foramina (holes through which blood vessels and nerves enter the intracranial vault) o Foramen magnum largest hole through which the brainstem extends to he spinal cord. ▪ Offers the only major space for the expansion of brain during increased ICP Vertebral Column • Protects the spinal cord, supports head, and provides flexibility • Made up of 33 INDIVIDUAL vertebrae o 7 Cervical o 12 Thoracic o 5 Lumbar o 5 Sacral (fused into 1) o 4 Coccygeal (fused into 1) • Held together by ligaments • Intervertebral discs occupy the spaces between vertebrae – allowing movement of the column Effects of Aging on the Nervous System o Loss of neurons occur in certain areas of the brainstem, cerebellum, and cerebral cortex ▪ It is a gradual process that begins in early adulthood o Loss of neurons lead to: ▪ Widening/enlarging of the ventricles ▪ Decreased brain weight ▪ ↓ cerebral blood flow ▪ ↓ CSF production ▪ Cerebral atrophy ▪ Pathologic abnormalities o In the PNS, degeneration of myelin ▪ ↓ in nerve conduction o More likely to experience orthostatic hypotension ▪ Coordinated neuromuscular activity such as the maintenance of BP gets altered with aging o Less able to adapt to extreme environmental temperatures ▪ ↑ risk for hypo/hyperthermia o ↓ Memory, vision, hearing, taste, smell, vibration and position sense, muscle strength, and reaction time o Sensory changes ▪ ↓ taste and smell perception - May lead to ↓ dietary intake ▪ ↓ hearing and vision - Can result in perceptual confusion o Problems with balance and coordination – risk for falls Assessment of the Nervous System Subjective Data: • Pain, headaches, dizziness (problem w/ cerebellum) • Past health HX- o First – determine if a medical emergency exists ▪ Ex: Is this patient showing signs of a decreased LOC ▪ Consider if the pt is a reliable source to obtain the info from o Second – the mode of onset and course of illness are the next important aspect of the HX. ▪ Obtain data about the characteristics and progression of the symptoms, any important birth hx (ex: cerebral palsy because of hypoxia), or any other neurological injuries (stroke, degenerative disease, traumatic brain injury) • Medications o Obtain a careful med hx, especially use of sedatives, opioids, tranquilizers, and mood-elevating drugs. o Also ask the patient to describe their med regimen (to determine med adherence) • Surgery or other Treatments o Ask about any surgery involving the nervous system like the head, spine, or other sensory organs o Inquire about any growth and development abnormalities • Functional Health Patterns o Ask a patient with a neurological problem those questions Function Patterns being assessed: ❖ Health-Perception Management Pattern: o A pt. with a neuro problem may have problems w/ self-care. o Ask about health practices related to the nervous system – substance abuse, smoking, adequate nutrition, BP management, safe participation in physical and recreational activities, nd use of helmets/seat belts o Ask someone close to the pt if they have noticed any mental or physical changes in the pt, because the patient may not be aware of it. ❖ Nutritional-Metabolic: o Neuro problems may affect the ability to chew or swallow, and it may be difficult for the pt to ingest adequate calories and nutrients o Thiamine (B1), Niacin, and Pyridoxine are essential for maintenance and health of CNS o Deficiencies in these vitamins can result in nonspecific complaints (depression, apathy, neuritis, weakness, confusion, irritability) o Untreated, cobalamin deficiency (Vitamin B12) –can cause mental function ❖ Elimination Pattern: o Bowel and bladder problems are usually associated w/ problems like stroke, MS, spinal cord injury, and dementia o Determine if there was previously a bowel or bladder problem (to plan appropriate interventions) o Urinary retention and incontinence are the most common problems ❖ Activity-Exercise pattern: o Can cause problems in pt’s mobility, strength, and coordination. o Neuro problems can cause a change in a person’s usual activity, it could also result in falls o Assess the person’s activities of daily living ❖ Sleep-Rest Pattern: o Can be a cause and response to a neuro problem. (chronic vs, acute) o Pain or hallucinations can interrupt sleep ❖ Cognitive- Perceptual Pattern: o Many disorders affect a person’s cognitive thought processes, and sensory integration o Ask the patient hypothetical questions, assess their memory, and language, calculation ability, and problem- solving ability. o Appropriate responses are a useful indicator of cognitive and perceptual ability. o Assess their ability to understand info related to their disease process, and o Carefully assess their pain because it is usually the reason a patient will seek care. o Delirium is acute and transient disorder that can be seen at any time in a person’s illness, an early indicator of various illnesses. ❖ Self-perception & Self-Concept pattern: o Neuro diseases can drastically alter a patient’s control over life and creates dependency on others o Their physical appearance and emotional control can be affected o Inquire about the patient’s evaluation of self-worth, perception, of abilities, body image, and general emotional pattern. ❖ Role-relationship pattern: o Neuro problems can change a person’s previous roles that may dramatically affect the patient or family. ▪ Weakness and paralysis o Family members or caregivers should participate in decision making when needed. ❖ Sexuality- Reproductive Pattern: Assess the patient’s ability to participate in sexual activity. o Cerebral lesions- can inhibit reflex responses of excitement phase o Brainstem and spinal cord lesions- may interrupt the desire or ability to have intercourse o Neuropathies and spinal cord lesions- may prevent reflex activities of the sexual response or affect sensation and decrease desire ❖ Cooping-Stress tolerance: o Often the problem is chronic, and the patients must learn new coping skills ❖ Value-Belief Pattern: Determine if any religious or cultural beliefs could affect the treatment. Objective Data: o FIRST thing you assess LOC, well groomed? (Do they take care of themselves or do they neglect), facial symmetry, is she able to move her arm and legs? VITAL SIGNS o Abnormal mentation status (LOC) may be described as dull or depressed, disoriented, stuporous, or comatose Physical Exam o Assesses 6 Categories: ▪ Mental status ▪ Cranial nerve function ▪ Motor function ▪ Sensory function ▪ Cerebellar function ▪ Reflexes ➢ TOOLS - Cotton, Flashlight, Opthalmoscope, Otoscope, Reflex hammer, Safety pins, Snellen cart, Tongue depressor, Tuning fork, Peppermint vial, Coffee, vinegar, Hot/cold water 1. Mental Status: o Assesses cerebral function and gives a general impression of how the pt. is functioning o Involves determining complex and high-level cerebral function o Assess language and memory when asking the pt. for details of the illness and past significant events **Consider age, cultural background, and level of education when evaluating** ▪ General Appearance & Behavior- includes level consciousness (awake, asleep, comatose), motor activity, body posture, dress and hygiene, facial expressions, and speech pattern. Assess language and speech! - A pt who has self-care deficits probably has other cognitive deficits ▪ Cognition- Note to orientation (time, place, person, situation), as well as memory, general knowledge, insight, judgement, problem-solving, and calculation - “Does a rock float on water” - “Who were the last 3 presidents?” o Note the presence of cognitive impairment, hallucinations, delusions and dementia ▪ Mood and Affect- note any agitation, anger, depression, euphoria, and appropriateness of these states. ▪ Is she neglecting one side of your body? (stroke) 2. Cranial Nerves: CHART Pg 1305 ▪ Olfactory Nerve • Rhinitis, sinusitis, heavy smoking may decrease sense of smell • A tumor may disturb ability to smell • Anosmia- loss of smell (early sign of Parkinson’s and Lewy body dementia) ▪ Optic Nerve- • Visual field defects may arise from lesions, optic chiasm, or tracts that extend through temporal, occipital, and parietal lobes. • Assess: peripheral and acuity • Visual field changes resulting from brain lesions include: • Hemianopsia- one half of visual field is affected • Quadrantanopia- one fourth is affected • Bitemporal hemianopsia- bilateral peripheral vision is affected • Monocular vision – both eyes are used separately ▪ Trigeminal – 3 division I. Ophthalmic branch II. Maxillary branch III. Mandibular branch ▪ Oculomotor, trochlear, and abducens nerves- • Any weakness or paralysis can cause the eyes not to move together, a disconjugate gaze, or nystagmus • Lack of pupillary constriction is an early sign of central herniation • PERRL or PERRLA is assessed • Ptosis- drooping of the eyelid can be caused by oculomotor damage 3. Motor System ▪ Assessment of strength, tone, coordination, and symmetry of the major muscle groups. ▪ Test muscle strength by having the patient push and pull against resistance of your arm, ask patient to offer resistance at the shoulders, elbows, wrists, hips, knees, and ankles. V 0: No visible muscle contraction V 1: Visible muscle contraction with no or trace movement V 2: Limb movement, but not against gravity V 3: Movement against gravity but not resistance V 4: Movement against at least some resistance supplied by the examiner 5: Full strength ▪ Pronator drift- Mild weakness of the arm seen by a downward drifting of the arm or pronation of the palm o Test is sensitive if the pt has a potential for vasospasm or increased edema in one hemisphere o Pt should close eyes and reach out like they’re holding a pizza and hold position for 30 SECONDS, if they drift downward that indicates a problem in the opposite motor cortex. ▪ Test muscle tone, Note any weakness or asymmetry in right and left sides o Hypotonia flaccidity o Hypertonia spasticity ▪ Note any involuntary movements o Tics, tremor, myoclonus (spasm of muscles), athetosis (slow, writhing, involuntary movements or extremities) ▪ Test cerebellar function by assessing balance and coordination by observing the patient’s posture and gait ▪ Finger to nose test (have pt alternately touch the nose, then touch the examiner’s nose) and heel-to-shin test (having the patient stroke the heel of one foot up and down the shin of the opposite leg) assess coordination and cerebellar fx ▪ Note any dysarthria or slurred speech b/c it is a sign of incoordination of speech muscles 4. Sensory System ▪ Each modality is carried by a specific ascending pathway in the spinal cord before it reaches the sensory cortex ▪ Perform the exam w/ the patient’s eyes closed and avoid giving the patient any clues ▪ Sensory testing of the anterior torso, posterior torso, and the four extremities ▪ If disturbance is identified in sensory fx of the skin, the boundaries of that dysfunction should be carefully delineated (described) along the dermatome (area of the skin supplied by nerves from a single spinal root) ▪ Light touch is tested w/ a cotton ball or light pinprick on each extremity ▪ Pain is assessed by using the dull and sharp end of a prick and asking the pt to identity which is which ▪ Extinction is assessed by simultaneously touching both sides of the body symmetrically. - An abnormal response occurs when the patient perceives the stimulus on only ONE side. - The other stimulus is extinguished ▪ Temp is only tested if an abnormal result for pain is obtained. Test by using hot and cold water to the skin and having the pt. identify which is which ▪ Vibration sense- assess vibration sense by applying a vibrating tuning fork to the fingernails and bony prominences and ask when the “buzz” is felt ▪ Position sense- o Romberg test = have the patient stand w/ their feet together and then close their eyes. If the patient can maintain balance w/ the eyes open but sways or falls w/ the eyes closed (Positive Romberg), vestibulocochlear dysfunction or disease in the posterior columns of spinal cord may be indicated o Nurse stands on their stronger side!! (you can hold onto them- if you stand on the weaker side most of the weight will fall onto you) ▪ Cortical sensory functions- o Two-point discrimination- by placing the two points of a calibrated compass on the tips of the fingers and toes, the minimum recognizable separation is 4-5mm in the fingertips and more separation elsewhere. o Graphesthesia- ability to feel writing on the skin o Stereognosis- ability to perceive the form and nature of objects 5. Reflexes ▪ A reflex contraction of the skeletal muscle occurs when the tendon is stretched ▪ Initiate a simple muscle stretch reflex by briskly tapping the tendon of a stretched muscle, usually w/ a reflex hammer ▪ The response is graded on a scale of 0-5 0= absent reflex 1= weak response, seen only w/ reinforcement 2= normal response 3= brisk response 4= hyperreflexia w/ nonsustained clonus 5= hyperreflexia w/ sustained clonus ▪ Clonus- an abnormal response, is a continued rhythmic contraction of the muscle w/ continuous application of the stimulus ▪ Deep Tender Reflex - Can be affected by: drugs, electrolytes (sodium/potassium), medication, dehydration, lesion and brain injury o How to test reflexes & the Normal Reponses: ▪ Biceps reflex- w/ the patient’s arm partially flexed and palm up, place your thumb over the biceps tendon in the antecubital space and strike the thumb w/ a hammer. Normal response is flexion of the arm at the elbow or contraction of the biceps muscle that cam be felt by your thumb ▪ Triceps reflex- striking the triceps tendon above the elbow while the patient’s arm is flexed. Normal response is extension of the arm or visible contraction of the triceps ▪ Brachioradialis reflex- by striking the radius 3-5 cm above the wrist while the patients arm is relaxed. The normal response is flexion and supination at the elbow or visible contraction of the brachioradialis muscle. ▪ Patellar reflex- strike the patellar tendon just below the patella. The patient can be sitting or lying if the leg being tested hangs freely. The normal response is extension of the leg w/ contraction of the quadriceps. ▪ Achilles tendon reflex- strike the Achilles tendon while the patient’s leg is flexed at the knee. The normal response is plantar flexion at the ankle. LECTURE DID YOU KNOWS.. ~ Gag reflex AKA pharyngeal reflexes ~ With a tuning fork above the head, which ear would you hear it the loudest? THE AFFECTED EAR! DIAGNOSTIC STUDIES CHARTS Pg 1310-1311 Cerebral Spinal Fluid • Lumbar Puncture - Pre-op: Consent, empty bladder, assess allergies to iodine b/c they have to prep the area w/ betadine - LONG-TERM complication: Herniation - If they have a headache DON’T DO LP [CT instead] ✓ Cause of h/a: fluid shift in spinal cord and can cause brain herniation - Afraid of infection - Long-term LP: they can have a headache ✓ Monitor for ICP, position them (30 degrees), GIVE IV FLUIDS (500-1000ml) Radiology • Skull and Spine x-rays • Cerebral angiography - Used to diagnose vascular problems. - Catheter is inserted into an artery (such as the femoral artery) – INVASIVE - Nurse should assess for bleeding after this procedure!! - Monitor for TIA (stroke) – slurred speech, weakness on one side, blood pressure, drooping of face • CT Scan – looking for structure (tumor, blood clot) - CT angiography (CTA) • MRI – looking at the tissue o Magnetic resonance angiography (MRA) - Look at the blood flow and arteries (e.g ACA, MCA) • Functional MRI (fMRI) • MR spectroscopy (MRS) Study • Positron emission tomography (PET) • Single-photon emission computed tomography • Myelogram Electrographic Studies • Electroencephalography (EEG) - Measures the electrical impulses of the brain - Seizure disorders are usually assessed using EEG testing. • Magnetoencephalography (MEG) • Electromyography (EMG) - Used to evaluate electrical innervation to skeletal muscle. • Electroneurography (nerve conduction studies) • Evoked potentials - Used for diagnosing problems with the visual or auditory systems Ultrasound • Carotid artery duplex scan - NOT invasive - Blockage? Perfusion is occluded - Get up abruptly they can pass out – dizziness!! - Monitor for TIA (stroke) ✓ COMPLICATION of surgery: a small particle can get dislodged and decrease blood flow • Transcranial Doppler • Biopsies (neurologic pathology) Anything with “gram” – use w/ contrast medium ✓ Check for allergies (iodine) [Show More]
Last updated: 1 year ago
Preview 1 out of 20 pages
Instant download
Buy this document to get the full access instantly
Instant Download Access after purchase
Add to cartInstant download
Reviews( 0 )
Document information
Connected school, study & course
About the document
Uploaded On
Jun 29, 2021
Number of pages
20
Written in

Additional information
This document has been written for:
Uploaded
Jun 29, 2021
Downloads
0
Views
47




.png)
.png)