*NURSING > CASE STUDY > NR 508 Week 3 Case Study Discussion: Case of Mr. Russell (Original Post & Responses) (All)
NR 508 Week 3 Case Study Discussion: Case of Mr. Russell (Original Post & Responses)
Document Content and Description Below
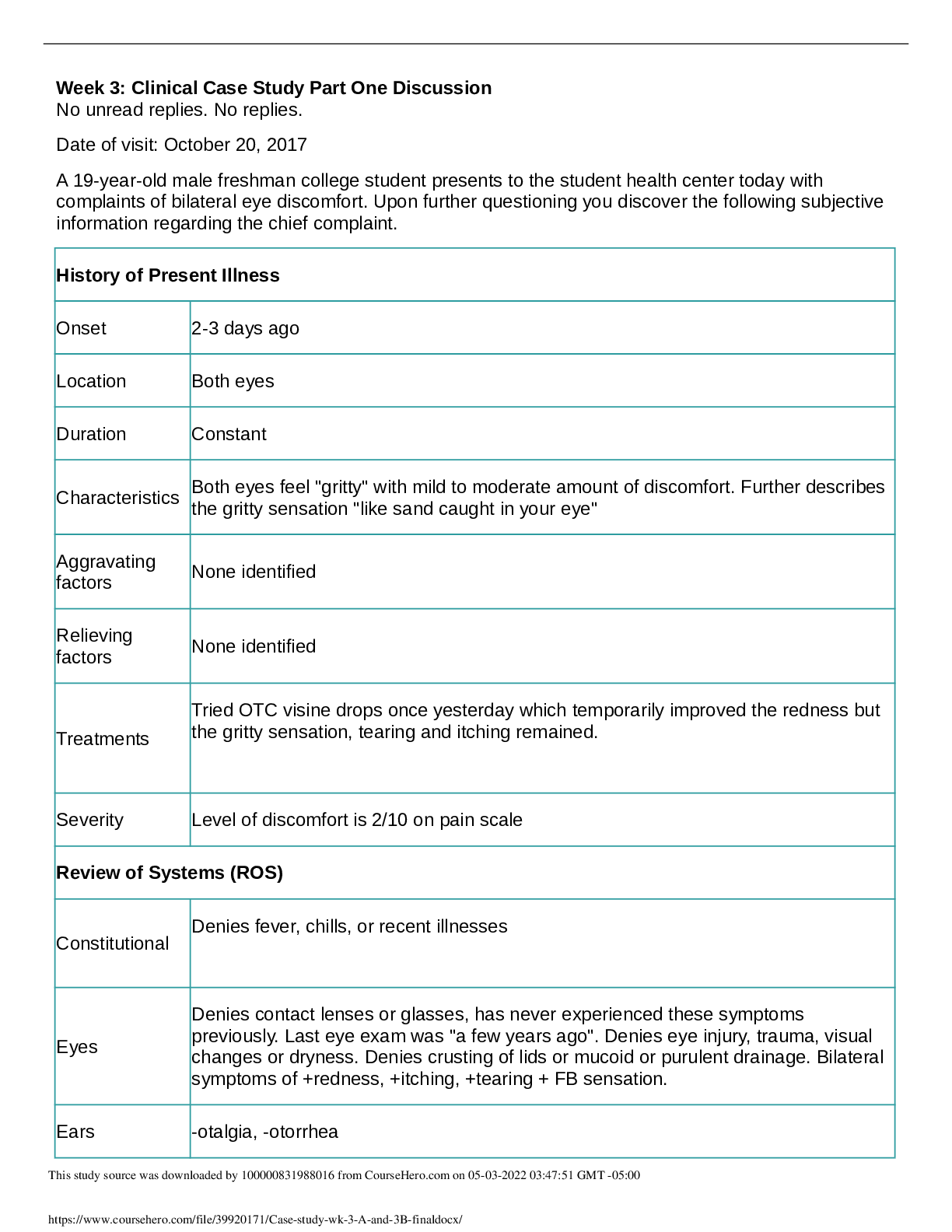
NR 508 Week 3 Case Study Discussion: Case of Mr. Russell (Original Post & Responses) Mr. Russell is a 73-year-old male who presents to your clinic with complaints heart palpitations and light... headedness on and off for the past 3 months. He has a history of hypertension and is currently prescribed HCTZ. He also is complaining of heartburn and belching after a large meal. Vital Signs: B/P 159/95, Irregular HR 88, Resp. 22, Weight 99 kilograms Lower extremities with moderate 3+edema noted in left leg, 2 + edema in right leg, ABD + BS, Neuro AOX3, Labs: NA 143mEq/L, CL 99 mmol/L BUN 18mg/dL, Hbg 15, TC 234 mg/dL, LDL 137 mg/dL, HDL 35 mg/dL, triglycerides 241mg/dL, ● What are your treatment goals for Mr. Russell today? ● What is your pharmacologic plan; please state your rationale for your plan? ● What are five key patient education points based on your plan? ● How would your plan change if your patient is African American? Dr. McMahon and class, Hypertension, or high blood pressure, is a serious common condition that affects one in every three Americans in the United States. While primary hypertension is often asymptomatic, long term hypertension increases the risk of developing a host of health complications, including coronary artery disease, heart failure, stroke, peripheral vascular disease, and vision loss (Woo & Robinson, 2016). Therefore, it is important to fully assess Mr. Russell and obtain pertinent information in regards to past medical history, family history, diet, exercise, and current medication regimen. What are the treatment goals for Mr. Russell? Complaints of heart palpitations and lightheadedness are important symptoms to carefully assess the underlying cause. In this case study, Mr. Russell has a history of hypertension and is currently taking HCTZ. According to the guidelines from the American College of Cardiology (2017), Mr. Russell’s current blood pressure reading is labeled as stage 2 hypertension with blood pressure greater than 130/90. If Mr. Russell is consistently taking his dose of HCTZ, our treatment goal is to lower his blood pressure to a targeted range within the next office visit. A reduction of blood pressure may help relieve the symptoms of heart palpitations and lightheadedness. It will also relieve the moderate edema that he is experiencing. Many of his laboratory results are borderline high, including high LDL/HDL and triglycerides, which indicate high cholesterol levels in the body. At this time, reviewing his past laboratory results to trend levels would be beneficial before deciding on an intervention. Education on proper diet and exercise to lower cholesterol would also be treatment goals for Mr. Russell. Lastly, it would be important to check potassium levels because hypokalemia is one of the side effects of HCTZ and can predispose patients to cardiac arrhythmias. An EKG would benefit Mr. Russell as well. What is the pharmacologic plan for Mr. Russell? If Mr. Russell is consistently taking HCTZ for hypertension treatment, it is a rational plan to either increase the dose of the existing medication or add a second agent. It is also important to consider the patient’s financial status because two agents will sometimes mean increased cost with two copayments instead of one. When making a decision, we should also consider the individual needs of the patient. There are several antihypertensives to consider, including thiazide diuretics, beta-blockers, angiotensin-converting enzyme (ACE) inhibitors, angiotensin II receptor blockers (ARBs), and calcium channel blockers. If Mr. Russell cannot afford a second copayment, the first line of treatment would be to increase the dosage of HCTZ. Thiazide diuretics have proven to be extremely effective in reducing blood pressure through sodium and water excretion (Woo & Robinson, 2016). If Mr. Russell is currently taking 12.5 mg HCTZ daily, I would titrate the dosage to 25 mg once daily. I would then reassess Mr. Russell in a month to see if we achieved our target blood pressure goal. At that time, we would reassess and consider other therapies if necessary. If Mr. Russell has no financial issues, I would opt to add a second agent to minimize adverse effects by keeping all doses low. As a second line of treatment, I would add an ACE inhibitor such as Lisinopril. The starting dosage of Lisinopril is 10 mg once a day. Lisinopril and HCTZ can be prescribed as a combination pill (10 mg/12.5 mg tablets taken daily). Lisinopril helps to reduce peripheral vascular resistance while HCTZ helps to secrete excess salt and water from the kidneys (Woo & Robinson, 2016). ACE inhibitors are effective in managing hypertension by inhibiting the conversion of angiotensin I to angiotensin II and aldosterone, and causing vasodilation. When an ACE inhibitor is used in combination with a diuretic, it is one of the most effective medications in treating hypertension in the elderly population. What are the five key patient education points based on the new pharmacologic plan for Mr. Russell? There are several education points to discuss with Mr. Russell when adding a second agent such as Lisinopril in addition to his current medication regimen. 1) The patient must be educated on the common side effects of Lisinopril. The most common side effects of ACE inhibitors include dry cough, headaches, hyperkalemia, orthostatic hypotension, and dizziness (Woo & Robinson, 2016). If any of these side effects become bothersome to the patients, encourage the patients to address these issues with their health care provider. The cough often takes up to a month to subside. A serious side effect of ACE inhibitors is angioedema, which is a rapid swelling of the mucous membranes within the mouth of throat (Cooper-Dehoff & Johnson, 2016). This type of symptom must be addressed immediately because it can impair respiratory function. 2) The patient must be educated on the importance of monitoring blood pressure and adhering to a strict medication regimen. Mr. Russell needs to understand that hypertension is often known as a “silent killer” because it typically does not produce any symptoms. Treating blood pressure on a consistent basis will help prevent long term consequences such as stroke, heart failure, cardiovascular disease, and kidney failure (Cooper-Dehoff & Johnson, 2016). 3) While there are other risk factors that cannot be modified, such as age, sex, or ethnicity, Mr. Russell should be educated on maintaining a healthy weight through healthy eating. High sodium consumption can raise blood pressure. Encourage Mr. Russell to refrain from excessively eating processed foods with high sodium concentration. A DASH diet is also recommended. The DASH diet consists of low sodium intake, as well as appropriate amounts of whole grains, fruits, vegetables, and low-fat dairy products. This type of dietary approach can help prevent or treat hypertension, and lower the risk of heart disease, stroke, and diabetes (American College of Cardiology, 2017). 4) Along with a healthy diet, Mr. Russell should participate in physical activity. Regular physical activity of light to moderate intensity helps improve overall health and fitness. As an older adult, Mr. Russell can be encouraged to do light exercises such as brisk walking and low intensity muscle strengthening exercises. Any type of physical activity will help manage the weight, strengthen the heart and muscles, and lower stress levels. 5) If Mr. Russell is currently smoking, smoking cessation is highly encouraged to reduce the risk of coronary artery disease, stroke, asthma, and lung cancer. The chemicals from smoking damages the lining of the vessels, which ultimately causes narrowing of the vessels. Therefore, education on smoking cessation is also essential. Lastly, Mr. Russell should be encouraged to elevate his feet to help reduce the edema and refrain from standing for prolonged period of time. He can also wear compression stockings to help control the swelling of his lower extremities. How would your plan change if your patient is African American? If Mr. Russell is African American, I would change the pharmacological plan. This is due to the fact that racial differences in adverse responses may occur. In the African American population, the risk of angioedema is three to four fold higher (Woo & Robinson, 2016). Since African Americans are susceptible to the adverse responses of ACE inhibitors, I would recommend calcium channel blockers. Calcium channel blockers have demonstrated effectiveness in the management of hypertension in the African American population. There have been recent studies that show lower responsiveness in maintaining optimal blood pressure control with the use of ACE inhibitors in the African American population (Prendergast et al., 2014). In the hypertensive African American population, the suggested initial therapy is a calcium channel blocker or thiazide diuretic. In this particular case, I would substitute Lisinopril with a calcium channel blocker, such as Amlodipine. In the United States, the prevalence of hypertension in African Americans is among the highest. Therefore, proper treatment to reduce adverse effects is essential for this population. References American College of Cardiology. (2017). High blood pressure in adults: Guideline for the prevention, detection, evaluation and management. Retrieved from http://www.onlinejacc.org/content/accj/71/19/e127.full.pdf? _ga=2.219622425.164853592.1541440094-1132604637.1541440094 Cooper-Dehoff, R., & Johnson, J.A. (2016). Hypertension pharmacogenomics: In search of personalized treatment approaches. Nature Reviews: Nephrology, 12(2), 110-122 Prendergast, H.M., Dudley, S., Brown, M., Daviglus, M., Kane, J., Bradshaw, B.E., . . . & Sanyaolu, R. (2014). Antihypertensive medications and diastolic dysfunction progression in an African American population. High Blood Pressure & Cardiovascular Prevention: The Official Journal Of The Italian Society Of Hypertension, 21(4), 269-274. doi:10.1007/s40292-014-0064-1 Woo, T & Robinson, M. (2016). Pharmacotherapeutics for the advanced practice nurse prescribers. (4th ed.) Philadelphia, PA: F. A. Davis Company Hi Ashley, Thank you for your informative post! As we know, there are many antihypertensive agents with different actions to lower blood pressure, such as decreasing cardiac output and renal blood blow, blocking sodium and chloride reabsorption in the kidneys, peripheral vasoconstriction, and affecting different receptors. Choosing an appropriate agent depends on the patient's medical history, age, race, co-morbidities, and renal function. Monitoring laboratory work, encouraging routine follow-up, and observing adverse effects of the drug are essential to the patient's plan of care. Currently, Mr. Russell is taking HCTZ, a diuretic that is often prescribed as the first line treatment for hypertension. I agree with you that adding an ACE inhibitor will help control his blood pressure. However, it is important that ACE inhibitors should not be given to elderly patients with reduced renal clearance (Woo & Robinson, 2016). Therefore, it would be beneficial to obtain Mr. Russell's renal function as well. Another important education for Mr. Russell is to keep track of his daily weight. A sudden weight gain may mean excess fluid building up in the body, which means the heart failure is getting worse (Flaten & Monte, 2017). Mr. Russell would need to be advised to contact his provider as soon as possible. ACE inhibitors are critical medications in the treatment to heart failure, and it is evident that Mr. Russell shows signs and symptoms of heart failure in this case study. Your pharmacological plan is a very thorough plan, and you provided rationale for every part of the plan. I would only add that before starting therapy with a statin, baseline laboratory values such as liver function and creatinine should be evaluated. References Flaten, H.K., & Monte A.A. (2017). Pharmacogenomic and metabolomic predictors of ACE inhibitor and angiotensin II receptor blocker effectiveness and safety. Cardiovascular Drugs & Therapy, 31(4), 471-482. doi:10.1007/s10557-017-6733-2 Woo, T & Robinson, M. (2016). Pharmacotherapeutics for the advanced practice nurse prescribers. (4th ed.) Philadelphia, PA: F. A. Davis Company Dr. McMahon, As many of us have learned, angioedema is one of the most serious adverse reactions heavily associated with ACE inhibitors. Angioedema is a rapid swelling of the mucous membranes within the mouth of throat (Cooper-Dehoff & Johnson, 2016). In many cases, angioedema can potentially cause respiratory issues that require immediate medical attention. ACE inhibitor- induced angioedema most commonly occurs within days of initiating therapy, but it also may occur weeks, months, or even years after the start of treatment. ACE inhibitors are responsible for the breakdown of bradykinin so bradykinin levels are increased. High bradykinin levels lead to increased vascular permeability and inflammation, which ultimately can increase the risk of angioedema (Woo & Robinson, 2016). There are risk factors that place certain patients at higher risk, including African Americans and people greater than sixty years of age. Other risk factors include those who have a history of idiopathic angioedema, head and neck surgery, and coexistent cardiopulmonary disease (Scalese & Reinaker, 2016). While ARBs are potential alternatives to treating hypertension, there is still a chance that angioedema may occur. According to Hjermitslev, Grimm, Wehland, Simonsen, & Kruger (2017), the adverse effects of cough and angioedema were seen less frequently during ARB therapy compared to those receiving ACE inhibitors. Other common adverse effects of ARB therapy include headache, dizziness, nausea, cough, and fatigue. It is important for healthcare providers to monitor renal function, and potassium and liver enzyme levels with patients taking ARBs. Education on ARB therapy, including proper dosage and side effects, is essential for better compliance rates. Most patients are noncompliant if they experience problematic side effects. ARB therapy has been shown to be effective in lowering blood pressure with same or fewer side effects as other treatment options, such as ACE inhibitors (Hjermitslev et al., 2017). References Cooper-Dehoff, R., & Johnson, J.A. (2016). Hypertension pharmacogenomics: In search of personalized treatment approaches. Nature Reviews: Nephrology, 12(2), 110-122 Scalese, M., & Reinaker, T.S. (2016). Pharmacologic management of angioedema induced by angiotensin-converting enzyme inhibitors. American Journal of Health-System Pharmacy, 73(12), 873-879. doi:10.2146/ajhp150482 Hjermitslev, M., Grimm, D.G., Wehland, M., Simonsen, U., Kruger, M. (2017). Azilsartan Medoxomil, an angiotensin II receptor antagonist for the treatment of hypertension. Basic & Clinical Pharmacology & Toxicology, 121(4), 225-233. doi:10.1111/bcpt.12800 Woo, T & Robinson, M. (2016). Pharmacotherapeutics for the advanced practice nurse prescribers. (4th ed.) Philadelphia, PA: F. A. Davis Company [Show More]
Last updated: 1 year ago
Preview 1 out of 6 pages
.png)
Also available in bundle (1)
NR 508 DISCUSSION TOPIC WEEK 1, CASE STUDY DISCUSSION WEEK 2, 3, 5 BUNDLE | 100% VERIFIED.
NR 508 DISCUSSION TOPIC WEEK 1, CASE STUDY DISCUSSION WEEK 2, 3, 5 BUNDLE | 100% VERIFIED.
By A+ Solutions 2 years ago
$14.5
4
Reviews( 0 )
Document information
Connected school, study & course
About the document
Uploaded On
Nov 11, 2021
Number of pages
6
Written in

Additional information
This document has been written for:
Uploaded
Nov 11, 2021
Downloads
0
Views
49


 Unfolding Reasoning.png)

.png)