Nancy Campbell iHuman Case Study
Document Content and Description Below
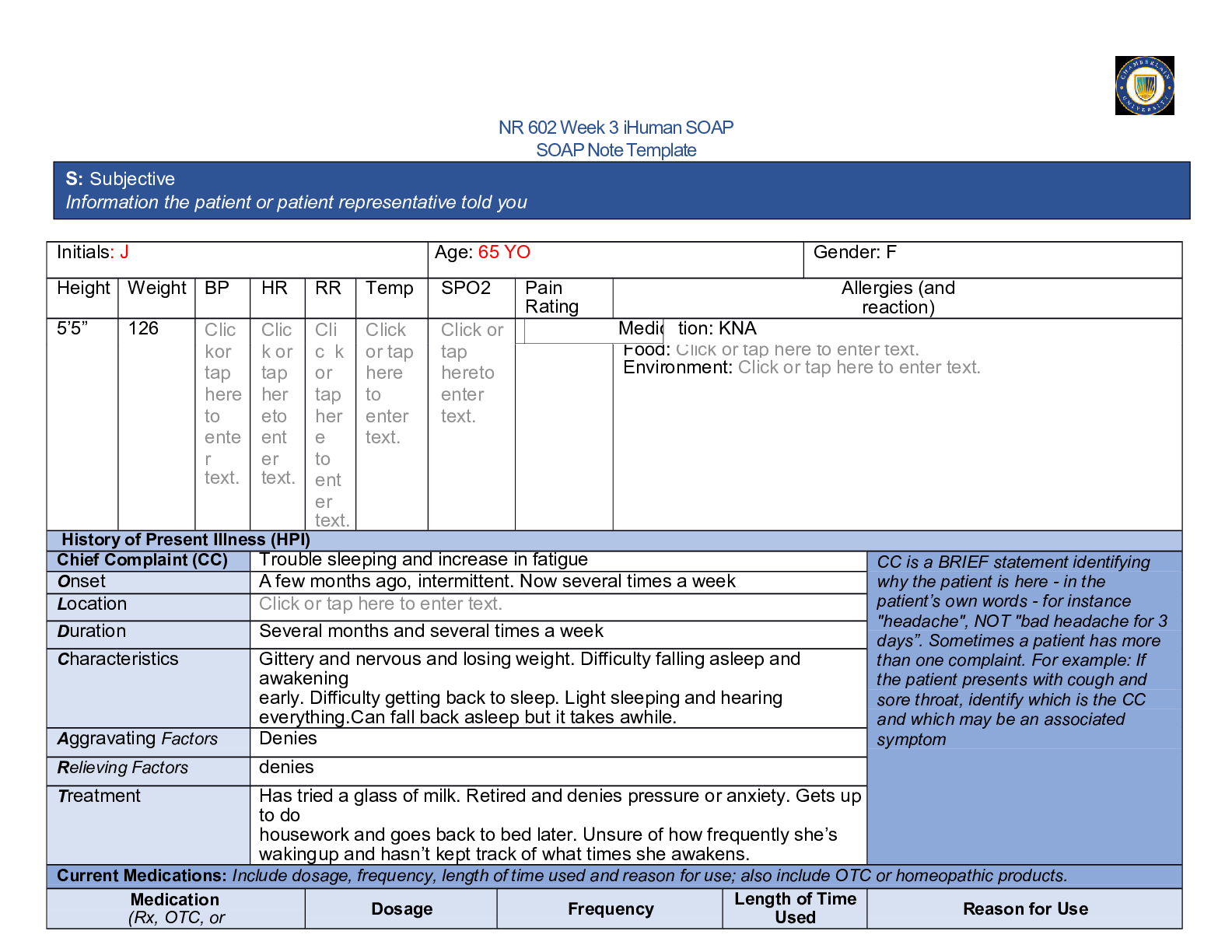
Nancy Campbell iHuman Case Study iHuman Case Study: Nancy Campbell Name Course DateCampbell Case Summary Ms. Nancy Campbell is 25 years old and comes to the clinic complaining of dysuria that ha... s lasted for three days. Other accompanying symptoms include a creamy vaginal discharge and an increased urination frequency. Ms. Campbell’s symptoms differ from those of UTI as she explains. She is sexually active and have more than one sexual partner and denies having protected sex instead opting for oral contraceptive pills. She denies ever being pregnant before and denies other symptoms. Symptoms presented suit those of cervicitis as described in this presentation. She denies chills, fever and other gastrointestinal symptoms such as nausea and vomiting. She was treated pharmacologically using Azithromycin 1000mg single dose to be taken orally and ceftriaxone 250mg IM single dose after a series of lab tests. The management plan was accompanied by patient education on abstinence and having protected sex. This illness has a clinical significance as it puts the patient at the risk of getting endometriosis or Pelvic Inflammatory Disease (PID). Other related risks are infertility, chronic pelvic pain and a higher risk of ectopic pregnancy. The pathogens that cause this illness can be sexually transmitted to the patient's sexual partners. According to Butaro, Trybulski, Polgar-Bailey & Sandberg, (2017), there is a high risk of shedding and acquisition of HIV-1 in patients with cervicitis.HPI CC: A Burning sensation that comes with urination History of Patient’s Illness: Ms. Nancy Campbell is a 25-year-old female patient who presents to the clinic with a chief complain of three-day old dysuria. She reports of a history of urinary tract infection and the burning sensation now is different from when she had UTI. Patient reports that other accompanying symptoms include increased urination frequency with urine that comes in small amounts. The patient reports that she has a creamy vaginal discharge that happens three times a day. Patient denies chills or fever, denies nausea, vomit or abdominal pain. Patient also denies breast tenderness. Patient reports that dysuria is relieved by soaking in warm water. After a physical examination, results show that there is a mucopurulent vaginal discharge that comes from the cervix. Tenderness is also noted. Patient reports of being sexually active and have more than one sexual partners and does not practice safe sex and instead takes contraceptive pills as a means of preventing pregnancy.Medical History Patient had urinary tract infection twelve months ago. No known allergies. No medical intolerances No chronic health complications or major traumas. No hospitalization or surgeries are done before. Medications: Oral contraceptive pills. And ibuprofen is taken for headache and menstrual pains. vaccinations are up to date.Family History Patient’s mother has type II diabetes and the father is battling high blood pressure, hyperlipidemia and coronary artery disease (CAD). Patient has a sister older than her and is healthy.Social History Ms. Campbell is a consultant and hence travels often. She reports to drinking two times a week and she drinks 4 or 5 drinks when she drinks. She previously used to smoke and denies other kinds of drug abuse. Patient has several sexual partners and denies using a condom but rather uses oral contraceptives.Review of Systems General: Patient denies changes in weight, sweating at night, fever and chills. Denies decreased energy levels. Skin: Denies delayed healings, lesions or bruises. Denies moles or discolorations of the skin. Eyes: Denies using corrective lenses, blurred vision or changes in vision. Ears: Denies ringing, discharge from the ears and hearing loss. Nose/Mouth/Throat: Patient denies sinus complications, nose bleeds or dysphagia. Denies dental complications, hoarseness or throat pain. Cardiovascular: Denies irregular heartbeats, orthopnea, chest pains and edema. Respiratory: Denies breathing complications, wheezing, coughing or dyspnea. Denies a history of tuberculosis or pneumonia.Review of systems cont’d Gastrointestinal: Patient denies gastrointestinal symptoms such as abdominal pain, constipation or black tarry stool. Denies eating complications, ulcers and hemorrhoids. Genitourinary: Positive for increased urination frequency, creamy vaginal discharge that is yellowish in color. Positive for spotting after sexual intercourse. Denies urine being frothy, denies hematuria. Last PAP test was twenty four months ago and showed normal results. Denies being pregnant before. Breast: Denies tenderness, bumps, skin changes around the breast and lumps. Denies pruritus and retraction of the nipples. Musculoskeletal: Denies pain in the back, joint complications such as swelling or stiffness. Denies a history of osteoporosis or fracture. Heme/Lymph/Endo: Denies blood transfusion, glands that are swollen, heat or cold intolerance and sweating at night. Denies increased hunger or thirst. Neurologic: Denies black-out spells, seizures and syncope. Denies weakness, transient paralysis or paresthesia. Psychiatric: Denies depression, anxiety or insomnia. Denies a history of suicidal thoughts or attempts.Examination Vital Signs Temperature: 98.7 F Weight: 135lbs Height: 5’5” Pulse: 66 bpm BMI: 22.5 B/P: 116/64 Resp.: 12 General Ms. Campbell is a healthy-appearing female who is in mild distress due to her condition. Patient is alert and well-oriented. Answers questions in the right way. Her skin is pink, intact, warm and clean with no rashes.Examination cont’d HEENT: Head is atraumatic and normocephalic with no lesions. Normally distributed hair. Eyes: PERRLA. EOMs are intact with no sclera injection or conjunctiva. Ears: Patent canals. TMs are bilateral and appear pearly gray with light reflexes that are positive. Easily visualized landmarks. Nose: Pink nasal mucosa with normal turbinates. No case of septal deviation. Neck: Supple with full ROM. No cervical lymphadenopathy or occipital nodes. No nodules or thyromegaly. Pink and moist oral mucosa. Nonerythematous pharynx with no exudates. Teeth are healthy. Cardiovascular: Normal S1 and S2 with normal rhythm and rate. No case of extra sounds, no murmurs, no clicks or gallops. Respiratory: Symmetrical chest wall and lungs are bilateral and clear to auscultation. Respirations are easy and regular. Gastrointestinal: No scars noted in the flat abdomen. Bowel sounds are audible in all the four quadrants. Abdomen non-tender, soft with no masses. No case of hepatosplenomegaly.Examination cont’d Breast: No changes in skin color around the breasts, nipples with no retraction. Both breasts have striae at the base. No tenderness to palpitation. No masses noted. Genitourinary: Bladder with no CVA tenderness. No case of cervical motion tenderness. No masses. Creamy discharge seen from the cervix. Cervix friable is notable. Musculoskeletal: ROM is full and is visible in all the four extremities upon patient’s movement. Neurological: Clear speech with a good tone. Erect posture, Balance is stable and gait is normal. Psychiatric: Patient is well-oriented and alert. Properly dressed and keeps a good eye contact. Patient answers questions in the right way.Labs (In-house) Urinalysis: Leukocytes esterase are present, urine is slightly cloudy and a high WBC count Urine culture: No growth of bacteria Neisseria Gonorrhoeae culture: Positive Chlamydia culture: No isolation of species of chlamydia. Cervical swab/gram stain: Negative for diplococci. STD culture: Positive for N. gonorrhea. No trichomonas, negative for syphilis, no HSV, candida or vaginalis related causal organisms present. Potassium Hydroxide: Negative Vaginal wet mount/vaginal smear: Leukocytes are present No motile flagella or clue cells. hCG plasma: Pregnancy test negative. Vaginal pH: 4.0 Anime test: Normal odor, negative. HIV: NegativePrimary and Differential Diagnoses Primary Diagnosis: Cervicitis O86.11 This is due to the fact that she has more than one sexual partners and does not use condoms. Patient has been having a yellowish vaginal discharge that is creamy for the last three days. After examination, results show friable cervix with no case of cervical tenderness motion. Symptoms include vaginal bleeding after sex, dysuria, bleeding between periods, painful sex, and creamy vaginal discharge, frequent urination with pain. Differential Diagnoses Pelvic Inflammatory Disease (PID) N73.9 Symptoms include; Lower abdominal pain, painful intercours, bleeding between menstrual cycles Urinary Tract Infection (UTI) N39.0 Symptoms include dysuria, increased urination frequency, pain in the lower abdomen, cloudy urine, fever and chills. Bacterial Vaginosis N76.0 Major symptoms include vaginal discharge, vaginal itching and dysuria.Management Plan Medications; Azithromycin 1000mg single dose to be taken orally and ceftriaxone 250mg IM single dose. Non-pharmacological interventions: Patient is to abstain from sex until she is healed. She should also consider safe sex and maintain one sexual partner. Tests ordered: Hepatitis B, HIV, screening for syphilis and PAP smear test. Patient is advised to take a HPV vaccine. Follow-up after two weeks and repeat the tests after three to six months. Referral: Gynecologist for the PAP test.Evidence-Based Article 1 “Managing sexually transmitted infections” by Johnson-Mallard et al., (2018) is a research article that gives insights into the management of STIs. The authors give the guidelines necessary for the prevention and the management of sexually transmitted illnesses. The article updates the tips periodically based on developing science. The article provides recent updates relevant to the management of STIs. The authors focus on the treatment plans, retests and detection repeat infections and updated vaccines on HPV. In conclusion, the authors of the article state that creation of awareness on STIs is the first step of prevention and management and it is the responsibility of the advanced practice registered nurses to ensure that the public knows the STIs. The authors identify some of the best prevention and management strategies that Ms Campbell could use in managing her condition.Evidence-Based Article 2 Tang (2018) wrote “Updates on Sexually Transmitted Infections: Gonorrhea, Chlamydia, and Syphilis Testing and Treatment in the Emergency Department”. The article focusing on the relevant updates on sexually transmitted illnesses. The author focused on illnesses such as chlamydia, gonorrhea and syphilis. Updates on the testing and treatment of these illnesses are well defined in this article. The article was written to review and define the present guidelines and studies on the screening, diagnosis and treatment of STIs in the emergency department. This article entails information that Ms Campbell can use in ensuring that her illness does not reoccur and how she will be in a position to prevent herself from other sexually transmitted illnesses. Information on screening will be essential in early detection of any STI that she could be suffering from.Evidence-Based Article 3 “A clinical Conundrum: Chronic Cervicitis” is an article written by Hester & Middleman in 2019 and addresses cervicitis through a case study of a 22-year-old non-pregnant patient who has chronic cervicitis. The authors wrote the article to study the illness through a case study to come up with reliable findings that can be applied in the management and prevention of cervicitis. The authors show that any bacterial regarded to be normal vaginal flora in non-pregnant women such as Ms Campbell should be taken as potential pathogens. This article is relevant as Ms. Campbell is suffering from cervicitis and the authors offer reliable information that can be used in the case of the patient.Evidence-Based Article 4 “Pelvic Inflammatory Disease: Possible Catches and correct Management in Young Women” is an article written by Di Tucci et al., (2018) addressing pelvic inflammatory disease. The authors state that it is still unclear on ways that can be used to accelerate the present treatment options and opt for surgical options in the management of the illness. The article is relevant to the case of Ms. Campbell because Pelvic Inflammatory Disease is a differential diagnosis in this case hence can be used by the physician to learn more about the illness which is related to an increased urination urgency.Evidence-Based Article 5 Management of women with cervicitis is an article written by Marrazo & Martin, (2017) giving insights on cervicitis. The authors define cervicitis as the result of gonorrhea and chlamydia that are often characterized by the mentioned mucopurulent discharge, friability, cervical bleeding and cervical secretions that have elevated leukocytes. The authors have given a recommendation of the treatment options for patients and their partners. Authors mention Cefixime 400mg orally taken, azithromycin 1g single dose accompanied by ceftriaxone 250mg IM. This is a relevant article in the case of Ms. Campbell as the mentioned treatment options can be applied to treat her current diagnosis.References Buttaro, T. M., Trybulski, J., Polgar-Bailey, P., Sandberg-Cook, J. (2017). Primary care: A collaborative practice, 5th Edition. [South University]. Retrieved from https://digitalbookshelf.southuniversity.edu/#/books/ Di Tucci, C., Di Mascio, D., Schiavi, M. C., Perniola, G., Muzii, L., & Benedetti Panici, P. (2018). Pelvic inflammatory disease: Possible catches and correct management in young women. Case Reports in Obstetrics & Gynecology, 1–4. https://doi.org/10.1155/2018/5831029 Hester, E. E., & Middleman, A. B. (2019). A Clinical Conundrum: Chronic Cervicitis. Journal of pediatric and adolescent gynecology, 32(3), 342-344. [Show More]
Last updated: 1 year ago
Preview 1 out of 20 pages
Reviews( 0 )
Document information
Connected school, study & course
About the document
Uploaded On
Nov 07, 2022
Number of pages
20
Written in

Additional information
This document has been written for:
Uploaded
Nov 07, 2022
Downloads
0
Views
153