*NURSING > EXAM REVIEW > Nur 280 Comprehensive Review (All)
Nur 280 Comprehensive Review
Document Content and Description Below
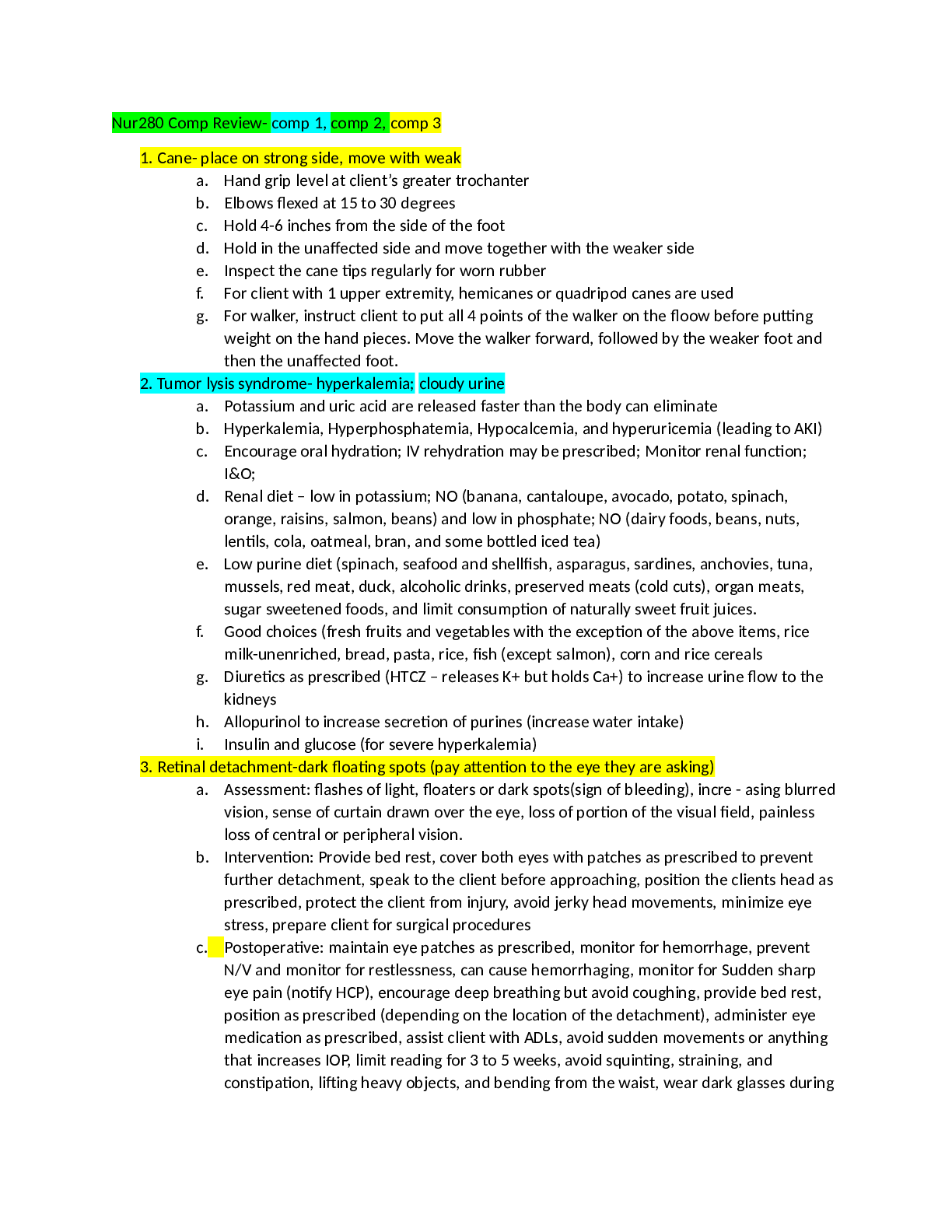
Nur280 Comp Review- comp 1, comp 2, comp 3 1. Cane- place on strong side, move with weak a. Hand grip level at client’s greater trochanter b. Elbows flexed at 15 to 30 degrees c. Hold 4-6 inches... from the side of the foot d. Hold in the unaffected side and move together with the weaker side e. Inspect the cane tips regularly for worn rubber f. For client with 1 upper extremity, hemicanes or quadripod canes are used g. For walker, instruct client to put all 4 points of the walker on the floow before putting weight on the hand pieces. Move the walker forward, followed by the weaker foot and then the unaffected foot. 2. Tumor lysis syndrome- hyperkalemia; cloudy urine a. Potassium and uric acid are released faster than the body can eliminate b. Hyperkalemia, Hyperphosphatemia, Hypocalcemia, and hyperuricemia (leading to AKI) c. Encourage oral hydration; IV rehydration may be prescribed; Monitor renal function; I&O; d. Renal diet – low in potassium; NO (banana, cantaloupe, avocado, potato, spinach, orange, raisins, salmon, beans) and low in phosphate; NO (dairy foods, beans, nuts, lentils, cola, oatmeal, bran, and some bottled iced tea) e. Low purine diet (spinach, seafood and shellfish, asparagus, sardines, anchovies, tuna, mussels, red meat, duck, alcoholic drinks, preserved meats (cold cuts), organ meats, sugar sweetened foods, and limit consumption of naturally sweet fruit juices. f. Good choices (fresh fruits and vegetables with the exception of the above items, rice milk-unenriched, bread, pasta, rice, fish (except salmon), corn and rice cereals g. Diuretics as prescribed (HTCZ – releases K+ but holds Ca+) to increase urine flow to the kidneys h. Allopurinol to increase secretion of purines (increase water intake) i. Insulin and glucose (for severe hyperkalemia) 3. Retinal detachment-dark floating spots (pay attention to the eye they are asking) a. Assessment: flashes of light, floaters or dark spots(sign of bleeding), incre - asing blurred vision, sense of curtain drawn over the eye, loss of portion of the visual field, painless loss of central or peripheral vision. b. Intervention: Provide bed rest, cover both eyes with patches as prescribed to prevent further detachment, speak to the client before approaching, position the clients head as prescribed, protect the client from injury, avoid jerky head movements, minimize eye stress, prepare client for surgical procedures c. Postoperative: maintain eye patches as prescribed, monitor for hemorrhage, prevent N/V and monitor for restlessness, can cause hemorrhaging, monitor for Sudden sharp eye pain (notify HCP), encourage deep breathing but avoid coughing, provide bed rest, position as prescribed (depending on the location of the detachment), administer eye medication as prescribed, assist client with ADLs, avoid sudden movements or anything that increases IOP, limit reading for 3 to 5 weeks, avoid squinting, straining, and constipation, lifting heavy objects, and bending from the waist, wear dark glasses during the day, and patches during the night, encourage follow-up because it may occur in the other eye. 4. Chest tube- bad if drainage is >100ml/hr a. Gentle bubbling in the suction chamber b. Water seal chamber tidaling is normal during inspiration and expiration, small bubbling but not continuous c. Needs to be placed lower than the patient d. Occlusive sterile dressing at the insertion site e. Do not strip or milk tubing unless instructed by HCP f. Have a clamp and occlusive dressing at the bedside at all times g. Encourage coughing and deep breathing h. Never clamp tubes without HCP prescription i. If drainage system cracks or break, place tube on sterile water, then replace with new system j. When removing tube instruct client to deep breath and hold it, or take a deep breath and bear down (valsalva maneuver). Dry sterile or petroleum gauze dressing is taped. k. If the chest tube is pulled out, pinch the skin opening together (close it), then apply an occlusive dressing then taped with overlapping pieces of 2 inch tape and notify HCP. 5. Diverticulosis- high fiber diet/ Diverticulitis- low fiber diet a. Outpouching or herniation occurring commonly in the sigmoid colon b. Watch for rigid board like abdomen, rebound tenderness, guarding of abdomen, increasing temp and chills, pallor, restlessness, tachycardia, and tachypnea (Peritonitis) c. Assesment: N/V, left lower quadrant pain that increases with coughing, straining or lifting, elevated temp, flatulence, cramplike pain, blood in stools, palpable tender rectal mass d. Interventions: During acute phase – bed rest, maintain NPO or provide clear liquids as prescribed. Introduce fiber containing diet gradually when inflammation has resolved. Administer antibiotics, analgesics, and anticholinergics to reduce bowel spasm as prescribed. Instruct client to refrain from lifting, straining, coughing, bending that increases intra-abdominal pressure. 6. 70/30- 70 NPH/30 regular insulin a. When mixing NPH and regular i. Roll NPH gently (do not shake) ii. Wipe both vials with alcohol wipes iii. Inject air to cloud (NPH) and then inject air to clear (regular) iv. Pull from clear (regular) and then pull from cloudy (NPH) b. Onset of 70/30 is 30 minutes and peak is 2-12 hours. c. Make sure client eats within 30 minutes of taking insulin d. Watch for signs of hypoglycemia 70 mg/dL (irritability, cool, clammy, tachycardia, palpitations, sweating, tremors, later signs involves changes in LOC and impaired coordinations up to loss of consciousness and seizures) e. Treatment for hypoglycemia – 4 tsp of sugar, 4 sugar cubes, 1 Tbsp honey, ½ cup fruit juice or non-diet soda, 6 saltine crackers, 3 graham crackers, 6 to 10 life savers or hard candy 7. Addison’s disease- hyperkalemia; hyponatremia and decreased blood glucose (not enough sugar, salt, sex) a. S/S: bronze skin, hypotension, lethargy, fatigue, muscle weakness, weight loss (hypovolemia due to low aldosterone), menstrual changes (women), impotence in men (low testosterone) b. Treatment: Lifelong glucocorticoid (hydrocortisone, cortisone, betamethasone, prednisone) and mineralocorticoid (fludrocortisone) treatment c. Watch for Addisonian Crisis (severe headache, severe abd pain, lower back, and leg pain, severe hypotension, hypovolemic shock, generalized weakness, and irritability and confusion. d. Intervention during crisis: i. Administer IV glucocorticoids as prescribed ii. IV fluids iii. After crisis, administer glucocorticoid and mineralocorticoid PO iv. Monitor VS, especially BP v. Monitor neurologic status (confusion and irritability) vi. Monitor I&O, electrolytes (K+, Na+), and blood glucose vii. Prevent infection (steroid therapy decreases immune function) viii. Maintain bed rest and provide a quiet environment 8. TPN- always have 2 nurses check order; change tubing Q24HR a. Hypertonic due to high glucose and amino acids b. Administered through PICC or midline (Central Venous catheters) c. If bag is empty and no other TPN is available hang 10% Dextrose in water. d. Lipids (fat emulsions) can be added and administered through a different line below the filter of the main IV set by Y-connector or as an admixture 3in1. If globules is observed or separation of emulsion, return it to pharmacy. No additives should be placed on the fat emulsion. Filter size should be 1.2um or larger. Infused at 1mL/min (60mL/hr), and monitor VS every 10 minutes for the first 30 minutes. (S/S: chest and back pain, chills, diaphoresis, cyanosis, dyspnea, flushing, headache, fever, N/V, thrombophlebitis, vertigo). Check patient with allergy to eggs before administering. If any reactions occur, stop infusion and notify HCP. e. No blood products on the PN line to prevent infection. f. Monitor blood glucose q4h. Risk of hyperglycemia from PN solution. 9. Urgent-can wait (multiple fx; 1+ pedal pulses) 10. Emergent-see NOW! (lung collapse, MI, sudden onset of chest pain, change in Vitals signs out of normal) 11. Non-urgent (walking around with wound, new onset of flu, cold, Closed fractures) 12. Abruptio placenta- no oxygen, painful, dark red bleeding, uterine rigidity a. LION – Lateral position, increase fluids, increase oxygen, Notify HCP b. Fetus is in distress and maternal shock may occur due to bleeding c. Interventions: Monitor maternal VS and fetal heart rate d. Assess for excessi [Show More]
Last updated: 1 year ago
Preview 1 out of 14 pages
Reviews( 0 )
Document information
Connected school, study & course
About the document
Uploaded On
Apr 20, 2022
Number of pages
14
Written in

Additional information
This document has been written for:
Uploaded
Apr 20, 2022
Downloads
0
Views
39

.png)