*NURSING > EXAM REVIEW > NURSING 326 Mental Health Exam 2 DEPRESSIVE DISORDERS: Guaranteed A (All)
NURSING 326 Mental Health Exam 2 DEPRESSIVE DISORDERS: Guaranteed A
Document Content and Description Below
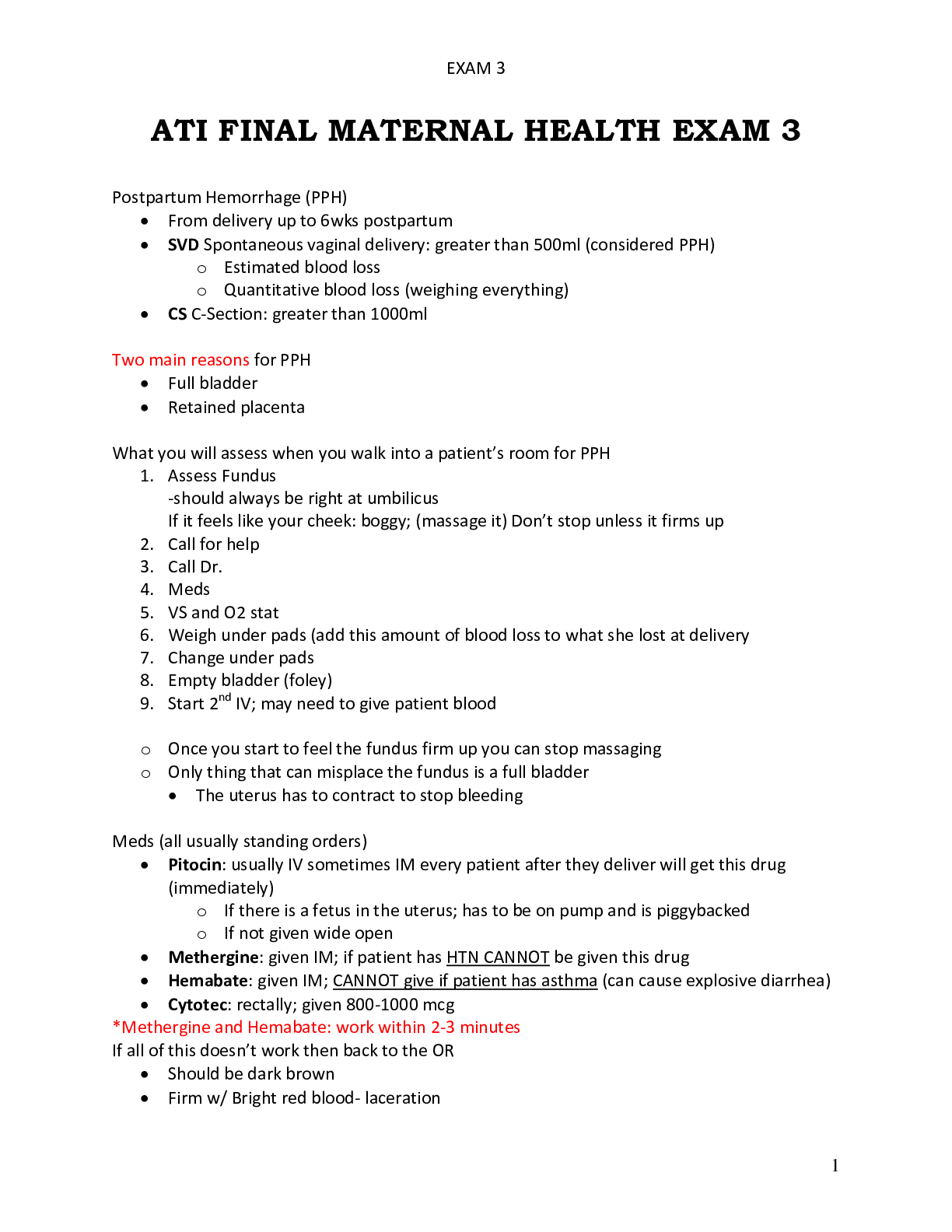
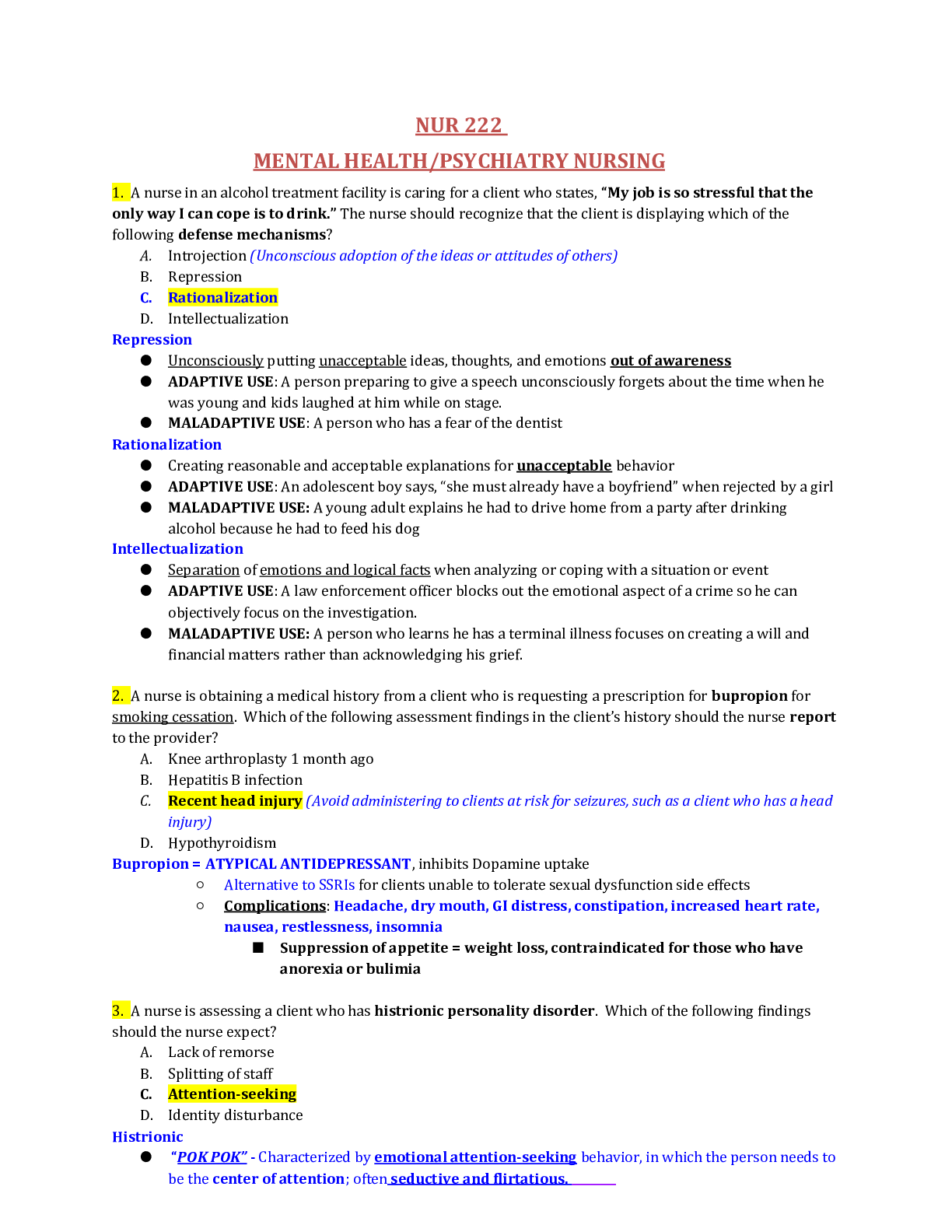
NURSING 326 Mental Health Exam 2 DEPRESSIVE DISORDERS: • Depression is the oldest and most frequently diagnosed psychiatric illnesses • Pathological depression occurs when the adaptation is i... neffective • Mood is aka affect • Depression is an alteration in mood that is expressed by feelings of despair, sadness, and pessimism RISK FACTORS • More prevalent in woman than men • More common in YOUNG women • Inverse relationship between social class and report of depression symptoms o Wealthy= increase in bipolar o Poor= increase in depression • Single and divorced people are more likely to experience depression • Seasons matter! More likely to be depressed in SPRING and FALL MAJOR DEPRESSIVE DISORDER • Depressed mood • Loss of interest in pleasure and activities (affects ADLs) • Present for MINIMUM 2 weeks • No history of manic behavior • Cannot be attributed to substance abuse or other medical conditions (i.e. hypothyroidism) PERSISTENT DEPRESSIVE DISORDER (DYSTHYMIA) • Sad • No psychotic symptoms (no distortion, hallucinations, voices, etc.) • Chronically depressed mood for most of the day, more days than not, for 2 years PREMENSTRUAL DYSPHORIC DISORDER • Depressed mood • Anxiety • Mood Swings • Decreased interest in activities • Begins a week before menses and relieves a few days after (PMS) Substance-Induced Depressive Disorders: direct result of substance abuse • Alcohol • Street drugs Depressive Disorder Associated with Another Medical Condition: attributed to the direct physiological effects of general medical conditions Depression: • May be genetic • Deficiency of serotonin, dopamine, or norepinephrine • Excessive cholinergic transmission • Possible failure within the hypothalamic-pituitary-adrenocortical axis Psychosocial Theories: • Psychosocial Theory o Loss is internalized and becomes directed against the ego • Learning Theory o Learned helplessness: excessive failures=giving up • Object Loss o Experiences loss within first 6 months of life o Feelings of helplessness and despair o Early trauma may cause lifetime of periods of depression • Cognitive Theory o Primary disturbance in depression is cognitive rather than affective o THREE cognitive distortions that are the basis for depression Negative expectations of the environment Negative expectations of the self Negative expectations of the future THE TRANSACTIONAL MODEL: Depression related to multiple factors including genetic, biochemical, and psychosocial CHILDHOOD DEPRESSION: • Younger than 3 o Feeding problems o Tantrums o Lack of playfulness o Emotional Expressiveness • Age 3 to 5 o Prone to accidents o Phobias o Excessive self-reproach • Age 6 to 8 o Physical Complaints o Aggressive behavior o Clinging behavior • Age 9 to 12 o Morbid thoughts o Excessive worrying ADOLESCENCE: a visible manifestation of behavioral change that lasts for several weeks **MANIFESTATIONS OF TEEN SYMPTOMS ARE MOSTLY THE SAME** • Anger, aggressiveness • Running away • Delinquency • Social withdrawal • Sexual acting out • Substance abuse • Restlessness, apathy ***All anti-depressants carry a black-box warning for increased risk of suicidality in children and adolescence***Most common precipitant to adolescent suicide is the PERCEPTION of abandonment by parents or close peer relationship***PROZAC ONLY*** Depression in Senescence: (older people) • Bereavement overload • High percentage of suicide among elderly • *Symptoms of depression are often confused with neurocognitive disorder* (dementia) • Tx includes medication, electroconvulsant therapy, and therapy **medicating elderly is very difficult** POST-PARTUM DEPRESSION • Associated with the serious hormonal changes that take place after giving birth • Inability to care for infant (may get psychotic) • Fatigue • Irritability • Loss of appetite • Sleep disturbances • Loss of libido • TX includes medication and psychosocial therapies MILD DEPRESSION (looks like normal grief) • Symptoms at this level are NOT necessarily dysfunctional • The ‘blues’ • Tearful, regression, mild anxiety • Difficulty getting mind off the event/loss/disappointment • Tired and Listless MODERATE DEPRESSION • ‘Eeyore’ (dysthymia) • Helpless, powerless • Sluggish • Slow thinking process SEVERE DEPRESSION • TOTAL despair • Feel worthless • Flat affect • Delusions: fixed false ideas and beliefs (no logic) o Somatic delusions • Psychomotor retardation, curled up position, absence of communication • Suicidal thoughts, general slow-down of the entire body ELECTROCONVULSIVE THERAPY: • Induction of a grand mal seizure through the application of electrical current through the brain • Electrodes are applied to the frontotemporal region or on the same side as the dominant hand • Seizure should last about 15 to 25 seconds • Normally administered every other day, 3x a week, for approx. 6-12 treatments • MOST EFFECTIVE IN THE TREATMENT OF SEVERE DEPRESSION • HIGH RISK= persons with myocardial infarctions, CVA within preceding 3-6 months, aortic or cerebral aneurysm, severe underlying HTN, and CHF • We believe that it works because seizure cause an increase on the circulating levels of serotonin, norepinephrine, and dopamine • ***Most common side effects include TEMPORARY MEMORY LOSS AND CONFUSION*** • Although rare, some permanent memory loss is possible • Death is rare and when someone dies it is usually cardiovascular • Guardians CANNOT sign consent for ECT • Before treatment: o Client should be NPO 6-8 hours before o Jewelry and dentures should be removed o Atropine should be given to dry secretion o Patient should void • Consent should be obtained before EVERY INDIVIDUAL treatment • Muscle relaxant is give before the seizure is induced, there is no VISIBLE seizure • MOST USEFUL IN ELDERLY PTS SUICIDE: • SUICIDE is a behavior, not a disease or diagnosis • Third leading cause of death among Americans 15-24 years of age • Fourth leading cause of death for ages 25-44 • Eighth leading cause of death ages 45-64+ • Gunshot wounds are the leading cause of death among suicide victims RISK FACTORS • Marital status (single=more likely to commit suicide) • Gender o Women more like to attempt, men more likely to succeed o Men choose more lethal methods • Age o Risk of suicide increases with age, especially in men o White men 80+ who are alone are the most at risk • Religion (protective element) • Socioeconomic status o The extremely wealthy are more likely to commit suicide o So are the extremely poor • Ethnicity o More likely in whites • Psychiatric Illness • Severe insomnia • Use of alcohol and barbiturates • Psychosis • Chronic Illness • Family History of Suicide • Sexual Orientation • Loss of a loved one • Previous attempt • Lack of employment and increased financial burden • Not entirely proven that there is any type of biological factor Durkheim’s Three Categories of Suicide: • Egotistic Suicide o To “solve” one’s personal problems • Altruistic Suicide o Laying down one’s life for another (hero) • Anomic Suicide o So angry at another person that they go to the extreme to hurt that person (killing oneself) Suicidal Ideas or Acts: Assessment of • Seriousness of intent • Plan • Means • Verbal and behavioral clues Analysis of the Crisis: • Precipitating stressor • Relevant History • ***Life-Stage Issues*** o Has not successfully completed a life-stage BIPOLAR AND RELATED DISORDERS: MOOD: pervasive and sustained emotion that may have a major influence on a person’s perception of the world AFFECT: emotional reaction associated with an experience MANIA: alteration in mood that is expressed by feelings of elation, inflated self-esteem, grandiosity, hyperactivity, agitation, and accelerated thinking and speaking. ***Bipolar disorder is characterized by mood swings from profound depression to extreme euphoria (mania)*** • Average onset is early 20s • More common in single than in married persons • Gender incidence is pretty equal • 6th leading cause of disability in the middle-age group • If a person has EVER had a history of mania they CANNOT be diagnosed as major depressive BIPOLAR I: • Little bit depressed through severe mania • Full syndrome of manic symptoms BIPOLAR II: • Has never met criteria for FULL manic episode • SEVERE depression and hypomania CYCLOTHYMIC DISORDER: • Chronic mood disturbance • At least 2-year duration SUBSTANCE INDUCED BIPOLAR: Direct result of the physiological effects of substance abuse PREDISPOSING FACTORS: • Biological lesions • Enlarged ventricles • Medication side effects • ***Psychosocial theories are not really valid*** • Transactional Model: Combination of factors BIPOLAR AND ADOLESCENCE • FIND o Frequency: symptoms occur most days in a week o Intensity: severe enough to cause extreme disturbance o Number: Symptoms occur 3 or 4 times a day o Duration: Symptoms last for 4 or more hours a day • Treatment o Medications Lithium Divalporex Carbamazepine Atypical antipsychotics o ADHD is most common comorbidity **ADHD medications tend to exacerbate manic episodes. Be sure that bipolar is under control before administering ADHD medications** • Categories of Mania: o Stage I Hypomania Not severe enough to cause impairment or to require hospitalization Cheerful mood Rapid flow of ideas o Stage II Acute Mania Marked impairment in functioning, usually requires hospitalization Accelerated, pressured speech Hallucinations and delusions Little need for sleep o Stage III Delirious Mania Labile mood, panic anxiety Disorientation, Exhaustion Death without intervention LITHIUM: • Therapeutic Range: o 1.0 to 1.5 mEq/L (acute mania) o 0.6 to 1.2 mEq/L (maintenance) • SYMPTOMS OF TOXICITY: o Blurred vision o Ataxia o Tinnitus o Persistent nausea & vomiting o Severe Diarrhea ***Ensure that the client consumes adequate sodium and fluids. DO NOT RESTRICT SODIUM*** [Show More]
Last updated: 1 year ago
Preview 1 out of 9 pages
Reviews( 0 )
Document information
Connected school, study & course
About the document
Uploaded On
Mar 18, 2021
Number of pages
9
Written in

Additional information
This document has been written for:
Uploaded
Mar 18, 2021
Downloads
0
Views
41





.png)