Chamberlain College of NursingNR 602NR 602 Week 3 Quiz.OSTEMYLITIS
Document Content and Description Below
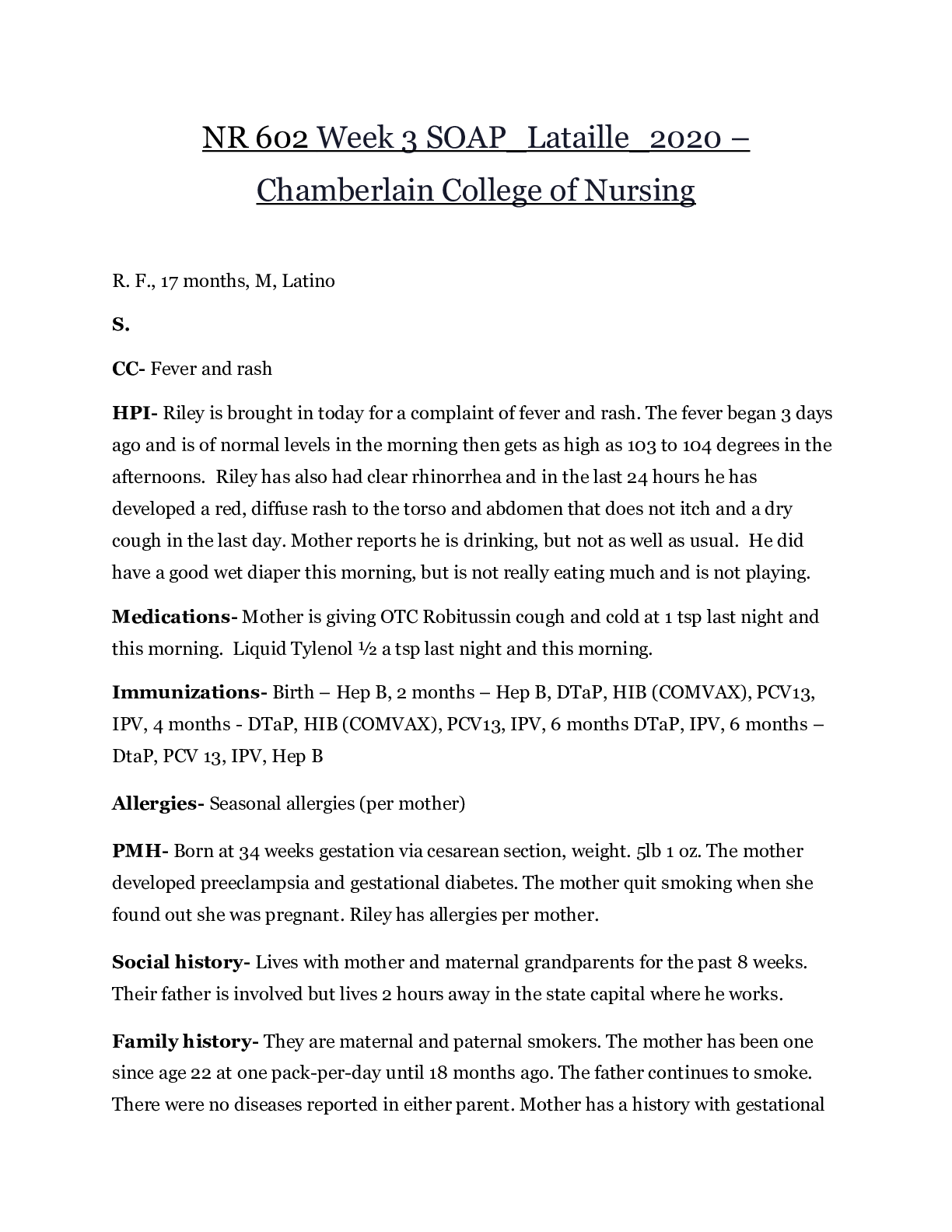
Osteomyelitis can occur if the puncture wound penetrates a bone or joint and is most commonly caused by P. aeruginosa in nondiabetic patients and is most commonly caused by S. aureus in diabetic pat... ients Examination findings consistent with osteomyelitisosteochondritis include: • Extension of pain and swelling around the puncture wound and to the adjacent bony structures • Exquisite point tenderness over the bone • Fever • Increasing erythema • Decreased use of the affected extremity Examination findings consistent with pyarthrosis (septic arthritis) include: • Pain, swelling, warmth, and erythema over the affected joint • Decreased range of motion and weight bearing of the affected joint • Fever DX: 1. Xray, 2. CT, 3. MRI. Bone scans are sensitive but not specific for osteomyelitis. Radiographs are specific, but findings for osteomyelitis are noted late. Clinical examination and laboratory studies and imaging should be considered early in the diagnosis of osteomyelitis MANAGEMENT: Obtain imaging studies as indicated. If imaging studies demonstrate that the foreign object has invaded bone, growth cartilage, or a joint space, refer the child immediately to an orthopedic surgeon. Always suspect a retained foreign object if the puncture wound is infected, the infection is not responding to antibiotic therapy, or if pain or aching of the injured site is still present weeks after the injury. In order to prevent a catastrophic outcome, wounds that are deep or highly contaminated should be referred to an orthopedic surgeon so that débridement can take place in an operating room. if there are signs of infection, the puncture is the result of a cat bite, or if the wound is deep or contained debris, antibiotics should be part of the treatment plan. Appropriate antibiotics for puncture wounds include amoxicillin clavulanate or cephalexin. Clindamycin should be used when children are allergic to penicillins. Plantar puncture wounds require ciprofloxacin. If methicillin-resistant Staphylococcus aureus (MRSA) is cultured from the wound or pus is present at the puncture site, then trimethoprimsulfamethoxazole (TMP-SMX) 1128or clindamycin is recommended until 1 sensitivities are known. All antibiotics should be prescribed for 7 to 14 days depending on severity of infection (Baddour, 2013). A recheck appointment should be scheduled 48 hours from the start of antibiotics for the patient receiving outpatient therapy. Treatment for severe infections secondary to puncture wounds, such as septic arthritis and osteomyelitis, includes surgical debridement and parenteral antibiotics. [Show More]
Last updated: 1 year ago
Preview 1 out of 22 pages
Reviews( 0 )
Document information
Connected school, study & course
About the document
Uploaded On
Sep 28, 2021
Number of pages
22
Written in

Additional information
This document has been written for:
Uploaded
Sep 28, 2021
Downloads
0
Views
55
.png)
.png)
.png)
.png)
.png)
.png)
.png)