*NURSING > CASE STUDY > Renal Replacement Therapy Case Study. (All)
Renal Replacement Therapy Case Study.
Document Content and Description Below
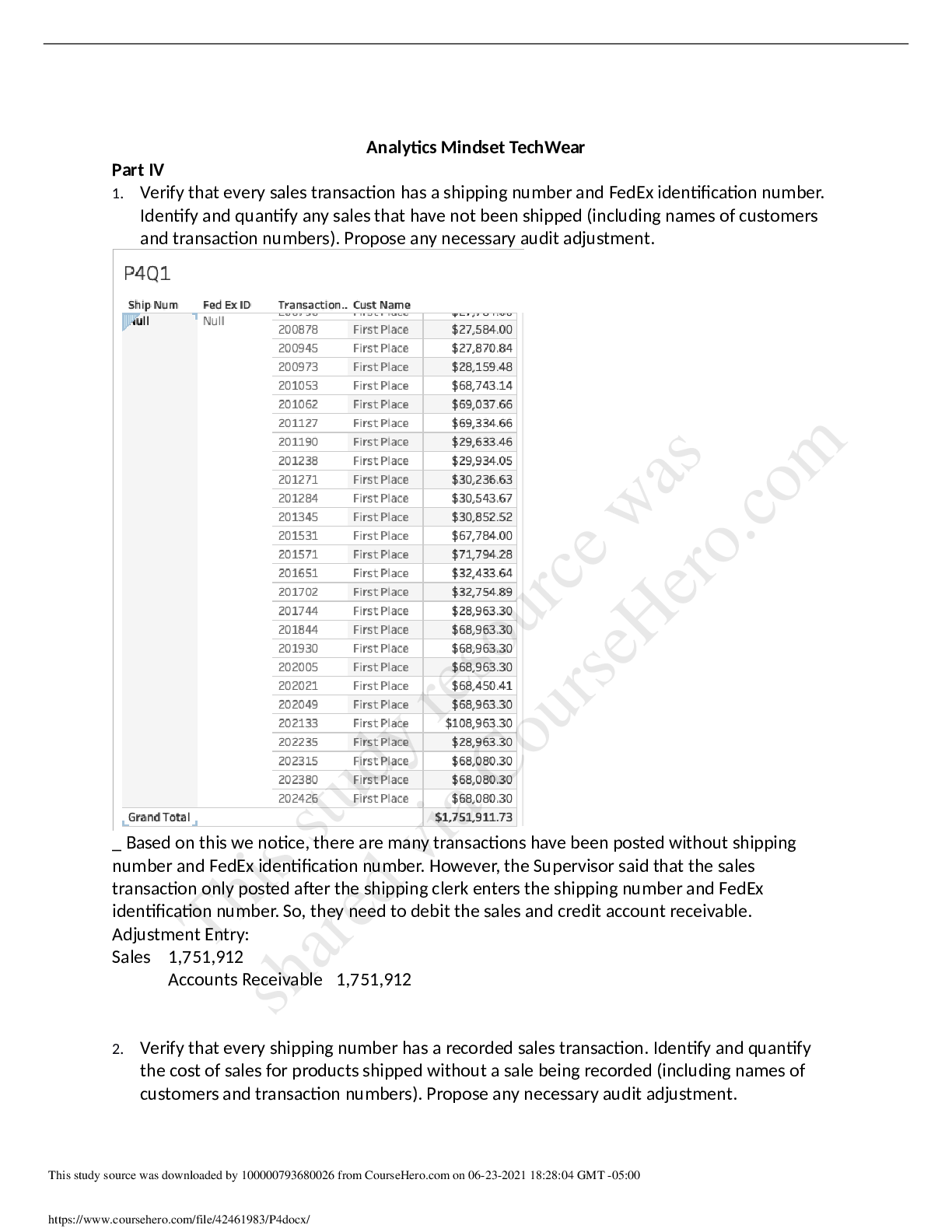
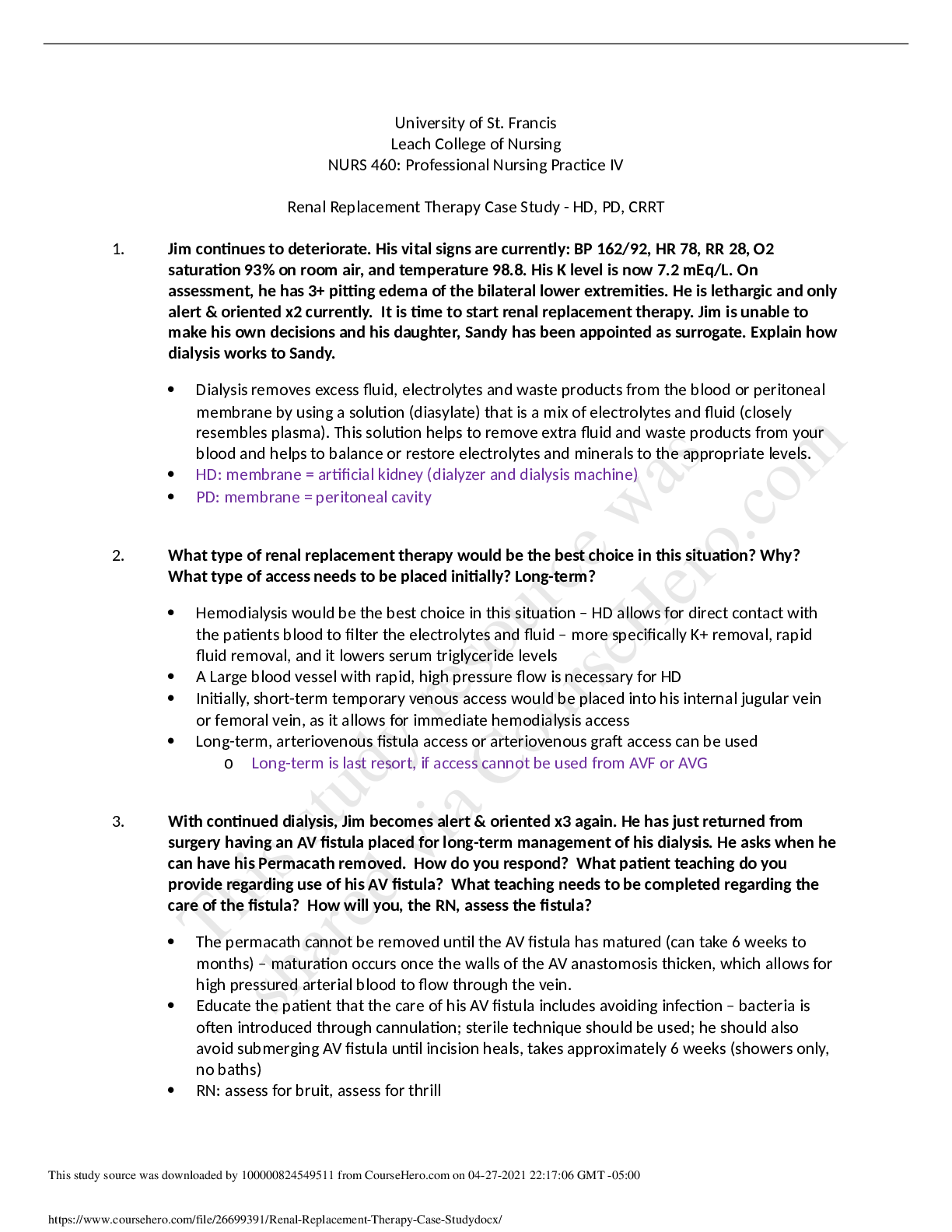
Renal Replacement Therapy Case Study - HD, PD, CRRT 1. Jim continues to deteriorate. His vital signs are currently: BP 162/92, HR 78, RR 28, O2 saturation 93% on room air, and temperature 98.8. His ... K level is now 7.2 mEq/L. On assessment, he has 3+ pitting edema of the bilateral lower extremities. He is lethargic and only alert & oriented x2 currently. It is time to start renal replacement therapy. Jim is unable to make his own decisions and his daughter, Sandy has been appointed as surrogate. Explain how dialysis works to Sandy. Dialysis removes excess fluid, electrolytes and waste products from the blood or peritoneal membrane by using a solution (diasylate) that is a mix of electrolytes and fluid (closely resembles plasma). This solution helps to remove extra fluid and waste products from your blood and helps to balance or restore electrolytes and minerals to the appropriate levels. HD: membrane = artificial kidney (dialyzer and dialysis machine) PD: membrane = peritoneal cavity 2. What type of renal replacement therapy would be the best choice in this situation? Why? What type of access needs to be placed initially? Long-term? Hemodialysis would be the best choice in this situation – HD allows for direct contact with the patients blood to filter the electrolytes and fluid – more specifically K+ removal, rapid fluid removal, and it lowers serum triglyceride levels A Large blood vessel with rapid, high pressure flow is necessary for HD Initially, short-term temporary venous access would be placed into his internal jugular vein or femoral vein, as it allows for immediate hemodialysis access Long-term, arteriovenous fistula access or arteriovenous graft access can be used o Long-term is last resort, if access cannot be used from AVF or AVG 3. With continued dialysis, Jim becomes alert & oriented x3 again. He has just returned from surgery having an AV fistula placed for long-term management of his dialysis. He asks when he can have his Permacath removed. How do you respond? What patient teaching do you provide regarding use of his AV fistula? What teaching needs to be completed regarding the care of the fistula? How will you, the RN, assess the fistula? The permacath cannot be removed until the AV fistula has matured (can take 6 weeks to months) – maturation occurs once the walls of the AV anastomosis thicken, which allows for high pressured arterial blood to flow through the vein. Educate the patient that the care of his AV fistula includes avoiding infection – bacteria is often introduced through cannulation; sterile technique should be used; he should also avoid submerging AV fistula until incision heals, takes approximately 6 weeks (showers only, no baths) RN: assess for bruit, assess for thrill This study source was downloaded by 100000824549511 from CourseHero.com on 04-27-2021 22:17:06 GMT -05:00 https://www.coursehero.com/file/26699391/Renal-Replacement-Therapy-Case-Studydocx/ This study resource was shared via CourseHero.com o If thrill or bruit is not assessed, use the Doppler. If not heard, need to check access of fistula or graft to make sure there’s adequate pressure for dialysis to occur Monitor for distal ischemia in the extremity (steal syndrome) – occurs from too much blood flow/shunting more blood through fistula or graft No BP, IVs, or blood draws in extremity with AVF ** - can alter access to dialysis 4. Jim has hemodialysis the next day. Prior to HD, he weighs 150 lbs. VS were T 98.7; BP 138/82; HR 98; RR 12. Upon return, you obtain the following data: weight 146 lbs.; T 99.4; BP 106/70; HR 89; RR 16. Are you concerned about any of these post-HD data? Why or why not? No, I am not concerned about any of these post-HD data. Hypotension is expected because of the rapid fluid removal; his temperature did not raise more than one degree (expected finding because solution is warmed); weight loss is expected d/t fluid removal; a decrease in HR is also an expected finding – the heart is not working as hard because there is less fluid to circulate If low-grade temperature persists for longer than an hour, then we would be concerned. Pts receiving dialysis have a blunted febrile response – continuous low-grade temp may indicate an infection 5. Jim’s AV fistula is in the right forearm. What are the 3 major complications associated with AV fistulas? What interventions would you take to prevent each of these potential complications? Aneurysm formation – avoid sticking in the same location – weakens vessel wall and increases risk of aneurysm Thrombosis – heparin is added to solution to prevent clotting Infection – sterile technique should be used Disequilibrium syndrome – cerebral edema and increased ICP due to a rapid decrease in BUN and fluid volume. Assess for headache, mental confusion, decreasing LOC, nausea, vomiting, twitching, possible seizures. Treat with anticonvulsants; prevention includes dialyzing for shorter times or reduce blood flow rates early in the course of therapy Hypotension – during and/or after procedure HD machine destroys protein Infectious disease – hepatitis B or HIV 6. While he waits to use his AV fistula, Jim is considering trying peritoneal dialysis for a few months. How does peritoneal dialysis work? Can any ESRD patient receive peritoneal dialysis? Why or why not? Peritoneal dialysis – a catheter is surgically placed through the abdominal wall (catheter has numerous perforations to allow for fluid to move in and out), the dialysis solution fills the [Show More]
Last updated: 1 year ago
Preview 1 out of 4 pages
Reviews( 0 )
Document information
Connected school, study & course
About the document
Uploaded On
Apr 28, 2021
Number of pages
4
Written in

Additional information
This document has been written for:
Uploaded
Apr 28, 2021
Downloads
0
Views
28