*NURSING > QUESTIONS & ANSWERS > NCSBN Practice Questions and Answers 2022 Update(Full solution pack), Questions with answers, Graded (All)
NCSBN Practice Questions and Answers 2022 Update(Full solution pack), Questions with answers, Graded A+
Document Content and Description Below
NCSBN Practice Questions and Answers 2022 Update(Full solution pack) Assistive devices are used when a caregiver is required to lift more than 35 lbs/15.9 kg true or false Correct Answer-True Duri... ng any patient transferring task, if any caregiver is required to lift a patient who weighs more than 35 lbs/15.9 kg, then the patient should be considered fully dependent, and assistive devices should be used for transfer If a draining wound tests positive for MRSA, the patient is placed on contact precautions True or False Correct Answer-True Patients with abscess or draining wounds who tests positive for MRSA are placed on contact precautions Hands can be cleaned with alcohol-based hand rub after caring for a patient with C. diff True or False Correct Answer-False Alcohol does not kill C diff spores and soap and water should be used for hand hygiene as recommended by CDC Disaster triage differs from route emergency department triage True or False Correct Answer-True Disaster triage categories range from most urgent (first priority), urgent, nonurgent (the walking wounded), and dead/catastrophic/coma. Newborns are fitted with tamperproof security sensors during their stay at the hospital True or False Correct Answer-TrueWearing a tamper proof safety device reduces the risk of abduction. The sensor shows the location of the infant and the security system can activate other devices (such as cameras, door locks, public address systems, sirens, and other alarms) in the event of an attempted abduction Restraints can be ordered prn by health care providers True or False Correct Answer-False HCP are required to specify duration and circumstances for which restraints are required and for how they should be used. Nurses and HCPs must frequently monitor patients to reassess for the continued need for restraints. Sensor pads may be used on beds of individuals who are a fall risk True or False Correct Answer-True Bed alarms and sensor pads can be used to alert caregivers when a patient is attempting to get up from a bed or chair, especially for a patient that is at risk for a fall. This is an effective alternative to the use of restraintts The 3 elements of radiation protection are time, duration, and shielding True or False Correct Answer-True The farther away people are from a radiation source, the less their exposure; as a rule, if you double the distance, you reduce the exposure by a factor of four. The amount of radiation exposure typically increases with the time people spend near the source of radiation You should quickly remove contaminated clothing by pulling it over your head True or False Correct Answer-False Contaminated clothing should never be removed quickly, but it should be cut off instead of pulled over your head. place contaminated clothing inside a plastic bag, seal the bag, and then place inside another plastic bagStandard precautions also includes respiratory/cough etiquette True or False Correct Answer-True Standard precautions are used to reduce the risk of transmission of bloodborne and other pathogens from both recognized and unrecognized sources. Respiratory hygiene/cough etiquette is now considered part of standard precautions The nurse is making patient room assignments. In order to minimize the risk of a hospital acquired infection, which of these children would be the most appropriate roommate for a 3-year-old child diagnosed with minimal change disease a. 3 year old with fracture, with a sibling that has Fifth disease b. 2 year old diagnosed with respiratory infection c. 6 year old with sickle cell disease experiencing vaso-occlusive crisis d. 4 year old with bilateral inguinal hernia repair Correct Answer-d. 4 year old with bilateral inguinal hernia repair Minimal change disease is a kidney disorder that can lead to nephrotic syndrome. Corticosteroids can cure the disease in most children but cytotoxic therapy and other drugs may be needed, but this treatment can reduce the child's ability to fight infection. The charge nurse must select a roommate who does not have an infection, which is the child child who had surgery. The sickle cell crisis may have triggered an infection. The child's sibling who has a viral disease has the potential to develop an infection. The nurse is setting up a patient's dinner tray. When the nurse turns her back to the patient, the patient grabs the nurse's buttocks and states that he is hungry for much more than dinner. Which of the following response by the nurse is indicated? a. ignore the behavior b. call the HCP c. quickly leave the room and ask UAP to assist the patient d. complete an incident report Correct Answer-d. complete an incident reportTo keep the therapeutic relationship intact, a nurse needs to set limits on appropriate behavior and not ignore bad behavior. Sexual harassment is a form of violence and is never part of the job. The nurse should report the incident to her supervisor and complete an incident report. The nurse has the right to ask not to be assigned to this patient. The paramedics are transporting a poisoning victim to the local hospital. In which of these cases does the nurse anticipate that hyperbaric O2 therapy will be used? a. 6yo found sitting on bathroom floor beside an empty bottle of diazepam b. 21 yo with suspected ethanol intoxication c. 35 yo found unconscious with suspected CO poisoning 2 yo who ate an undetermined amount of crystal drain cleaner Correct Answer-c. 35 yo found unconscious with suspected CO poisoning CO poisoning is the leading cause of poisoning in the US. It causes severe hypoxia which is why treatment includes high-dose oxygen. In severe poisoning, hyperbaric O2 therapy may be used. Treatment for: -crystal drain cleaner and diazepam may include gastric lavage and/or activated charcoal -alcohol intoxication may include gastric lavage, IV fluids, and supportive care A neonate is having difficulty maintaining a temperature above 98F and is placed in an infant warming system. Which of the following actions will ensure the safety of the neonate? a. monitor temperature continuously b. avoid touching neonate with cold hands c. warm all medications and liquids before administration d. wrap the neonate snugly in a cotton blanket Correct Answer-a. monitor temperature continuously When using the warming device, the neonate's temperature should be continuously monitored using a probe that securely attached to the skin. Monitoring the neonate's temperature is the priority safety concern because the skin burns, permanent brain damage or even death can result due to improper useor monitoring of equipment. No clothing or swaddling is needed in the IWS; usually babies are dressed only in a diaper (although bubble wrap blankets or plastic wrap blankets can be used to minimize heat loss in high risk newborns). For healthy term newborns, nurses should warm their hands and stethoscopes prior to contact with the baby. A nurse is conducting a community-wide seminar on childhood safety issues. Which of these children is at the highest risk for poisoning a. 20 month old who has just learned to climb the stairs b. 10 yo who occassionally stays at home unattended c. 15 yo who likes to repair bicycles d. 9 month old who stays with a sitter 5 days a week Correct Answer-a. 20 month old who has just learned to climb the stairs Toddlers, aged 1-3 years, are at highest risk for poisoning because they are increasingly mobile, need to explore and engage in autonomous behavior A nurse is performing well-child assessments at a day care center when a staff member interrupts the exam for assistance with another child. The nurse finds a 3 yo child on the floor with bleeding gums and 2 unlabeled open bottles nearby. What should the nurses first action be? a. call poison control and then 911 b. administer syrup of Ipecac to induce vomiting c. ask the staff member about the contents of the bottles d. give the child milk to coat the stomach Correct Answer-c. ask the staff member about the contents of the bottles The nurse needs to asses the situation and determine what the child ingested. Once the substance is identified, the poison control center and the emergency medical services should be called. The nurse administer a new medication to the patient. Which of the following actions best demonstrates an awareness of safe and proficient nursing practice?a. verify order prior to administration. ask for patient name b. verify patient's allergies on chart and name on door, ask date of birth c. ask name and allergies, then check wristband and allergy band d. ask name then check wristband Correct Answer-c. ask name and allergies, then check wristband and allergy band A dual check is always done for the patient's name. This would involve verbal and visual checks. Because this is a new medication an allergy check is appropriate. The other option have parts that might be correct actions. However, to be the correct answer all the parts of an option need to be correct. The nurse is caring for a patient who is not oriented to time, place, or person and has repeatedly attempted to pull out IV line and a feeding tube. The nurse receives an order from HCP to apply a vest and soft wrist restraints. Which of the following actions by nurse are appropriate? Select all that apply a. release the restraints and provide care Q4 b. call HCP for new order Q48 c. document which alternative interventions were used or attempted d. tie restraints using quick release knots e. explain the rationale for restraints to patient f. conduct a thorough assessment of the patient Correct Answer-c. document which alternative interventions were used or attempted d. tie restraints using quick release knots e. explain the rationale for restraints to patient f. conduct a thorough assessment of the patient Prior to applying restraints, the nurse must first conduct a thorough assessment of the patient and document the behavior and/or events leading up to the use of the restraints. The nurse should also document which alternatives to restraints were tried and the patient's response to those measures. Even though the patient is confused, nurse must still explain the reason for applying the restraints. A physician's order is renewed daily. Many policies state that the patient in restraints must be assessed hourly, care is given and documented at least every 2 hours.A patient diagnosed with gastroenteritis, caused by a salmonella infection. Which of these actions is the primary nursing intervention designed to limit the transmission of salmonella? a. hand hygiene before and after patient contact b. decontaminate with alcohol-based skin disinfectant c. wear 2 pairs of gloves when changing contaminated linens d. isolate the patient in a single room without a roommate Correct Answer-a. hand hygiene before and after patient contact Salmonella is a bacteria and of the causes for gastroenteritis. Gastroenteritis is characterized by acute onset of nausea, vomiting, abdominal cramps, and/or diarrhea. The CDC recommends using standard precautions for this illness, which is the why the primary nursing intervention is thorough handwashing before and after contact with patient using soap and water. Skin disinfectants can reduce the number of bacteria on the hands but cannot replace the importance of washing with soap and water. Contact isolation is not needed. Symptomatic patients can be cohorted. Double-gloving can be effective in surgery, but it is probably not needed when changing contaminated linens. The medication benztropine mesylate is ordered, but the nurse incorrectly administers carvedilol. What are the most important actions the nurse should take after making this medication error? Select all that apply a. document administration of carvedilol b. monitor and document the patient's BP c. notify HCP d. notify patient e. notify nurse manager Correct Answer-a. document administration of carvedilol b. monitor and document the patient's BP c. notify HCP e. notify nurse manager When the nurse makes a medication error, the patient's safety and well-being are the top priority. The nurse will document giving the beta blocker carvedilol and as well as any effects the medication has onthe patient. The HCP must be notified; the nurse will document that the provider was called and that orders were implemented. The nurse manager must be notified. Once the patient is stable, the nurse will complete an incident/variance/quality assurance report within 24 hours of the incident. The initial disclosure of the medication error with the patient should occur as soon as reasonably possible after the event, usually 1-2 days after the event. After an explosion at a factory, one of the employees approaches the nurse and says, "I am a CNA at the local hospital." Which of these tasks would be appropriate for nurse to assign to this worker who is assisting in the care of the injured. a. take temp b. palpitate pulses c. measure BP d. check alertness Correct Answer-b. palpitate pulses The heart rate and regularity would indicate if the patient is in shock or has the potential for shock. If pulses cannot be easily palpitated or are irregular, those patients would be seen first and further assessment by the nurse could be done (including measuring BP). Taking the temperature is not a priority at this time Which situation requires hand washing? Select all that apply a. after cleaning a wound b. after contact with inanimate objects in the immediate vicinity of a patient c. prior to eating d. before having direct contact with a patient e. after making a chart entry Correct Answer-a. after cleaning a wound b. after contact with inanimate objects in the immediate vicinity of a patient c. prior to eating d. before having direct contact with a patientHandwashing is still the simplest and most effective strategy to prevent the spread of infection. It is necessary to wash one's hands to protect oneself prior to eating, after removing gloves following any patient procedure, and even after having contact with intact ski or objects in the patient's room. However, it is not necessary to wash hands after handling every chart (although using an alcohol-based hand rub would be advisable). The nurse is offering safety instructions to a parent with a 4-month old infant and a 4 yo child. Which statement by the parent indicates a correct understanding of the appropriate precautions to take with the children. a. "I have the 4 yo hold and help feed the 4 month old a bottle with me." b. "I place my infant in the middle of the living room floor on a blanket to play with my 4yo while I make supper in the kitchen." c. My sleeping baby lies so cute in the crib with the little buttocks stuck up in the air while the 4 yo naps on the sofa." d. "I strap the infant car seat on the front seat to face backwards." Correct Answer-a. "I have the 4 yo hold and help feed the 4 month old a bottle with me." The infant seat should be placed on the rear seat. Small children and infants should not be left unsupervised. Infants are to be placed on their backs when they are sleeping or lying in a crib. A 4 yo could assist with the care of an infant, such as feeding with proper direct supervision. A patient is admitted to an impatient crisis unit with the diagnosis of acute mania and has been placed in seclusion. The nurse is assigned to observe the patient at all times. It is now time for the patient's dinner. What action should the nurse take next? a. Serve dinner in the seclusion room maintaining close observation. b. Obtain a contract for safe behavior before accompanying the patient to the dining room c. Accompany the patient to the dining room and maintain observation d. Hold the meal until after the seclusion order is discontinued. Correct Answer-a. Serve dinner in the seclusion room maintaining close observation. Seclusion is ordered by the physician and requires continuous observation, unless the order is discontinued or amended. It is incorrect to amend the seclusion or mealtime. Meals can be eaten in theseclusion room with the nurse continuing 1:1 observation. Meals should be offered on time and should not be withheld. Contracts for safe behavior are meaningless in the presence of psychotic behavior - mania The hospital sounded the call for disaster drill on the evening shift. Which of these patients would the nurse put first on the list for discharge in order to make room for new admissions? a. A middle-aged patient with 7-year history of being ventilator dependent and who was admitted with bacterial pneumonia 5 days ago. b. An older adult with a history of hypertension, hypercholesterolemia, and lupus, and who was admitted with Steven Johnson syndrome that morning c. A young adult with DM2 for more than 10 years and was admitted with antibiotic induced diarrhea d. An adolescent with a positive HIV test and was admitted with cellulitis of the lower leg 48 hours ago. Correct Answer-a. A middle-aged patient with 7-year history of being ventilator dependent and who was admitted with bacterial pneumonia 5 days ago. The best candidate for discharge is one who has a chronic condition and has an established plan of care. The patient who has been on a ventilator for years is most likely stable and could continue medication therapy at home. The other patients have a risk for instability or are unstable. The school nurse is providing information for teachers at a school where 10 yo child with epilepsy attends. What is the most important action a teacher can take when the child experiences a tonic-clonic seizure in the classroom. a. Clear the immediate are of anything that could harm the child b. provide privacy and reassure the other children c. note the sequence of movements with the time lapse of the event d. Place something soft and flat under the child's head Correct Answer-d. Place something soft and flat under the child's head During seizure activity, the priority would be to protect the child from physical injury. The teacher could place something soft and flat, like folded jacket under the child's head to help prevent head trauma. After protecting the head, the prioritized sequence would be to move furniture away from the child, note movements and time, and then provide privacy, if possible, while reassuring the other students.The charge nurse on the evening shift is asked to determine which patient is a candidate for discharge following an internal disaster in the hospital at 2100. which of these patients would the nurse select as a potential candidate for discharge? a. An older adult female who is actively dying and has a DNR b. A middle-aged adult with a history of DM1 and 1 day post DKA c. A young adult admitted at the beginning of the shift, with an asthma exacerbation d. An adolescent admitted on the day shift to rule out acute pancreatitis, who reports a history of alcohol abuse Correct Answer-b. A middle-aged adult with a history of DM1 and 1 day post DKA The patient selected to be discharged should be one whose condition is more stable than the others and where there is less of a risk for complications or instability after discharge. Although the patient with asthma has a chronic condition, she was just admitted and is experiencing acute exacerbation of the condition. The adolescent is experiencing an acute condition, probably brought on by alcohol abuse. Neither of these patients are stable enough for discharge. It is a humane choice to allow the patient who is in the process of dying to stay in the hospital. The patient is admitted to same day surgery for carpal tunnel release of the left wrist. Before the anesthetic is administered, what measures are used to prevent surgical errors? Select all that apply a. The pre-op nurse reviews all relevant documents b. The anesthesiologists asks if anyone has any concerns c. Surgical site is marked by surgeon d. The patient is asked to confirm correct surgical site e. The patient is asked to state name and DOB Correct Answer-c. Surgical site is marked by surgeon d. The patient is asked to confirm correct surgical site e. The patient is asked to state name and DOB Marking the correct site helps prevent wrong site operations. The patient must also verbally state name and DOB (and any other identifiers required by facility). Pre-op verification of all required document is done independently by at least 2 providers. When the patient is in the OR suite, a time out is called. Thisis the final safety check between the surgical, nursing, and anesthesia care teams immediately before the procedure. It is not enough for one person to ask if there are any other questions or concerns. The parent of a toddler ask the nurse how long their child will have to sit in a car seat while in an automobile. What is the nurse's best response to the parents? a. "The child can use a regular seat belt when can sit still." b. "Your child must reach a height of 50 inches to sit in a seat belt." c. "The child must be 5 yo to use a regular seat belt." d. "Your child must use a car seat until he weighs at least 40 lbs." Correct Answer-d. "Your child must use a car seat until he weighs at least 40 lbs." The guidelines for car seats depend on the child's weight, height, age, and car type. Children should use car seats until they weight 40 lbs according tho the US National Highway Traffic Safety Administration. The nurse observes a nursing assistant using aseptic hand rub and rubbing hands vigorously after leaving the room of a patient with C diff. Which action is most appropriate by the nurse? a. Ensure that visitors wash hands thoroughly before and after visiting. b. Require that the nursing assistant wash hands again using soap and water. c. Tell the patient to ask caregivers if they have all washed their hands d. Praise the nursing assistant for proper use of antiseptic hand rub Correct Answer-b. Require that the nursing assistant wash hands again using soap and water. Anyone who is hospitalized should be encouraged to ask caregivers if they washed their hands and to remind visitors to wash their hands. However, it is the nurse's responsibility to supervise the nursing assistant and to correct practice errors as needed. C diff is one of the few pathogens that require soap and water for cleansing the hands. Since antiseptic hand rub is ineffective against the hardy spores produced by the bacterium, the nurse should require the nursing assistant to wash his or her hands with soap and water, especially after providing care to this patient. An 80 yo patient has taken a benzodiazepine for insomnia for many years. The patient now reports experiencing anxiety and some confusion. What is most likely the reason for this?a. Decrease GI motility b. Poor rate of elimination by the kidneys c. Decreased liver function d. Decrease in lean body mass and increase in body fat Correct Answer-d. Decrease in lean body mass and increase in body fat Absorption, distribution and elimination of medications are al affected by age-related changes. Since drug distribution is most affected by the change in the body fat and lean body mass, this can lead to increased elimination half-life and prolonged effect of lipid soluble drugs such as benzodiazepines. Dosages that may have a therapeutic effect of a 65yo can produce significant side effects for older patients. An adolescent patient arrives at a clinic three weeks after the birth of her first baby. She tells the nurse she is very worried about not returning to her pre-pregnancy weight. What approach should the nurse take first? a. Review the patient's pattern of weight gain over the past year b. Give her several pamphlets on postpartum nutrition c. Ask the mother to record her diet for the next few weeks d. Encourage her to talk about her self-image Correct Answer-d. Encourage her to talk about her selfimage Body image is very important to an adolescent. The nurse must acknowledge this and collect more information about the client's self-image before discussing nutritional needs, diet and/or exercise. Adolescents often need more support and information about what to expect after the birth of a child, especially since the postpartum period can be overwhelming for them. Nonjudgmental and developmentally appropriate interactions are needed to care for the physical and emotional needs of adolescents. The partner of a patient with Alzheimer's disease expresses concern about the burden of caregiving. Which of these actions by the nurse should be a priority? a. Link the caregiver with a support groupb. Ask the friends to visit regularly c. Schedule a home visit each week d. Request anti-anxiety prescription Correct Answer-a. Link the caregiver with a support group Assisting caregivers to locate and join support groups will be most helpful and effective. Families share feelings and learn about services such as respite care. Health education is also available through local and national Alzheimer's Association chapters. The school nurse is checking students for pediculosis capitis. Which manifestation observed by the nurse confirms the presence of pediculosis capitis? a. Scratching the head more than usual b. Whitish oval specks sticking to the hair shaft c. White flakes on the student's shoulders d. Oval patterns of occipital hair loss Correct Answer-b. Whitish oval specks sticking to the hair shaft Diagnosis of pediculosis capitis, or head lice, is made by observation of the white eggs (nits) firmly attached to the hair shafts. Treatment can include application of a medicated shampoo with lindane for children over 2 years-old and meticulous combing with a special comb for the removal of all nits. The nurse is explaining an illness to a 10yo child. What should the nurse keep in mind about the cognitive development of children at this age? a. Children of this age are able to make simple association of ideas b. They are able to think logically in the organization of facts c. Interpretation of events originate from their own perspective d. Conclusions are based on previous experiences Correct Answer-b. They are able to think logically in the organization of facts Children in concrete operations stage, according to Piaget, are capable of mature thought when they are allowed to mentally or physically manipulate and organize objects.The RN is making a presentation about Lyme disease to a group of volunteers who host hiking tours through grassy areas. Which statement made by one of the volunteers indicates that more teaching is needed? a. Lyme disease can spread to my brain if I don't seek treatment b. Lyme disease is caused by a virus because the symptoms are similar to the flu c. I should wear light-colored clothing and long pants when hiking d. I will call the doctor if I see a rash that looks like a bull's eye Correct Answer-b. Lyme disease is caused by a virus because the symptoms are similar to the flu Lyme disease is caused by bacteria called Borrelia burgdeorferi. It is transmitted by ticks that are passed it on from infected mice or deer. Because the ticks are so small, it is easier to see them on light-colored clothing; long pants and long-sleeved shirts help protect hikers. Symptoms of lyme disease are similar to influence and there may be a bull's eye rash at the site of the tick bite. Without antibiotics , the disease can spread to the brain, heart, and joints of the body. The nurse is assessing the mental status of a patient admitted with possible dementia. Which of these options would best assess the functioning of the patient's short-term memory? a. Ask the patient to recall 3 words the nurse had previously asked the patient to remember b. Ask the patient to copy an image of 2 simple, intersecting geometric shapes c. Ask the patient to calculate simple arithmetic operations d. Ask the patient to name the last four presidents Correct Answer-a. Ask the patient to recall 3 words the nurse had previously asked the patient to remember Short-term memory refers to the temporary storage of information in memory and the management of the information so that it can be used for more complex cognitive tasks, such as learning and reasoning. Tests of cognitive function are used to evaluate cognitive impairment. The Mini-Mental Status Exam, for example, measures orientation to time and place, calculation, language, short-term verbal memory, and immediate recall. To help determine short-term memory functioning, the health care practitioner would ask the client to recall three words that the client had previously been asked to remember. A nurse is providing foot care instructions to a patient with arterial insufficiency. The nurse would identify the need for additional teaching if the patient makes which statement?a. I will trim corns and calluses regularly b. I cannot go barefoot around my house c. I can only wear cotton socks d. I should ask a family member to inspect my fee daily Correct Answer-a. I will trim corns and calluses regularly Older adults should not cut their nails, corns, and calluses. They should have them trimmed by their HCP, nurses, or another provider who specializes in foot care. Older adult patients who have diagnosis of diabetes or vascular disease often have decreased circulation and sensation in one or both feet. Their vision may also be impaired. Therefore, they need to be taught to examine their feet daily or have someone else do so. They should wear cotton socks that have not been mended, and they should always wear shoes when out of bed. The nurse is performing the following actions immediately following a delivery of a health, normal newborn. Indicate the correct sequence of actions by dragging and dropping the options below into the correct order. a. Administer Vitamin K b. Assess the infant's airway and breathing c. Perform bulb suctioning if excessive mucus is present d. Assess the infant's heart rate e. Place ID bands on infant and mother Correct Answer-b. Assess the infant's airway and breathing c. Perform bulb suctioning if excessive mucus is present d. Assess the infant's heart rate e. Place ID bands on infant and mother a. Administer Vitamin K Assessing the airway and respirations is the first action. Next if indicated, the baby should be suctioned. Then the heart rate is assessed. After these initial assessments, the identification bands are placed on both mother and baby. IM administration of vitamin K is recommended for the newborn but this can be done after the initial assessments and proper identification.Using a vibrating fork, the nurse will perform the Rinne test to assess the patient's hearing. Where will the nurse place the tuning fork to assess for bone conduction of sound? Correct Answer-The Rinne test helps distinguish between conductive and sensorineural hearing loss. To assess for bone conduction of sound, the nurse holds the tip of a vibrating tuning fork against the mastoid bone. Normally, air conduction is audible longer than bone conduction, but the reverse is true for someone with conductive hearing loss. The nurse is assessing the heart sounds of a patient admitted to the telemetry unit with a diagnosis of mitral stenosis. Indicate where the nurse should place the stethoscope to best assess the mitral valve. Correct Answer-Auscultation of heart sounds is a key component of the physical assessment. It is important that the nurse is able to identify the area on the chest that corresponds to each of the four valves. The mitral area or apex of the heart is located at the fifth intercostal space, left midclavicular space. A parent asks the nurse about a Guthrie Bacterial Inhibition test that was ordered for her newborn. Which of the following points should the nurse discuss with the patient prior to this test? a. Routine screening of newborn infants is not mandatory in the US b. This test identifies an inherited disease c. This test will be delayed if the baby's weight is less than 5 pounds d. The urine test can be done after 6 weeks of age e. Positive tests require dietary control for prevention of brain damage f. Best results occur after the baby has been breast-feeding or drinking formula for 2 full days Correct Answer-b. This test identifies an inherited disease c. This test will be delayed if the baby's weight is less than 5 pounds d. The urine test can be done after 6 weeks of age e. Positive tests require dietary control for prevention of brain damage f. Best results occur after the baby has been breast-feeding or drinking formula for 2 full days Screening for PKU is mandated in all 50 states., though methods of screening vary. The Guthrie Bacterial Inhibition Assay (BIA) is one test used to diagnose phenylketonuria (PKU), a disease characterized by an enzyme deficiency. A blood sample is taken from the baby's heel shortly after birth, with a follow-up test 7 to 10 days later. Test results are more accurate if the baby weighs more than 5 pound and has been regularly drinking milk for more than 24 hours. A urine test is normally done after 6 weeks of age if a baby did not have the blood test.A patient is in the 3rd month of her first pregnancy. During the interview, she tells a nurse that she has several sex partners and is unsure of the identity of her baby's father. Which of these nursing interventions is best at this time? a. Refer the patient to family planning clinic b. Discuss the risk for cervical cancer c. Counsel the woman to consent to HIV screening d. Perform tests for STDs Correct Answer-c. Counsel the woman to consent to HIV screening The patient's behavior places her at high risk for HIV. While it would be a good idea to draw blood to test for STDs, this can't be one without informed consent of the patient. Since the woman is already at a clinic seeking health care, it would be best to provide information (and possibly begin treatment) now, instead of simply referring her to another health care facility. The best response is for the nurse to provide information and counsel the woman to consent to HIV screening. The nurse is assessing a patient in her 3rd trimester. The patient is informed that the ultrasound suggests the baby is small for gestational age. An earlier ultrasound indicated normal birth. The nurse understands that this change is most likely due to what factor? a. Exposure to teratogens b. STIs c. Maternal hypertension d. Chromosomal abnormalities Correct Answer-c. Maternal hypertension Pregnancy-induced hypertension is a common cause of late pregnancy fetal growth restriction. Vasoconstriction reduces placental exchange of oxygen and nutrients. The other 3 conditions are associated with the first trimester time period. The nurse performs a heel stick for a blood glucose check on a 1 hour old, full-term newborn who weighed 9 lbs at birth. The serum glucose reading is 45 mg/dL. What action is needed by the nurse? a. Repeat the test in 2 hoursb. Give oral glucose water c. Notify the pediatrician d. Check the pulse oximetry reading Correct Answer-a. Repeat the test in 2 hours A serum glucose of 45 mg/dL is considered normal (normal range for the neonate is about 40-90). Neonatal hypoglycemia is defined as a blood glucose level of less than 30 in the first 24 hours of life and less than 45 in thereafter. Risk for hypoglycemia includes newborns who weigh more than 4 kg or less than 2 kg at birth, are large for gestational age; also gestational age less than 37 weeks and newborns suspected of hypoglycemia in the first hour of life. Due to the weight of the newborn, repeat blood glucose testing is indicated. A patient referred for mammography questions the nurse about the cancer risks from radiation exposure. What is the appropriate response by the nurse? a. You have nothing to worry about, it is less than tanning in the nude b. A chest x-ray gives you more radiation exposure c. The radiation from a mammography is equivalent to one hour of sun exposure d. Exposure to mammography every 2 years is not dangerous Correct Answer-c. The radiation from a mammography is equivalent to one hour of sun exposure A patient would have to have several mammograms in a year's time to be at a risk for cancer. The radiation exposure from one mammogram session is thought to be equivalent to being out in natural sunlight for one hour. This answer is concise and gives the patient a point of reference. To say not to worry is judgmental and non therapeutic. In the other 2 options one is not accurate and can cause further concern about radiation exposure and one does not clearly address the patient's question. The nurse is caring for a neonate immediately following a vaginal delivery. Which of the following interventions will promote temperature regulation in the neonate? Select all that apply. a. Place the neonate under a radiant warmer b. Bathe the neonate to remove contaminants after delivery c. Wrap the neonate in blankets d. Dry the neonate in warm towelse. Encourage skin to skin contact with the mother Correct Answer-a. Place the neonate under a radiant warmer c. Wrap the neonate in blankets d. Dry the neonate in warm towels e. Encourage skin to skin contact with the mother After drying off the wet amniotic fluid, placing the neonate under the radiant warmer or placing the neonate skin to skin against the mother will provide a source of heat for the neonate. Wrapping the neonate in blankets will help to reduce heat loss. The neonate should not be bathed until the temperature is stabilized. While giving care to a 2 yo patient, the nurse should remember that the toddler's tendency to say "no" to almost everything is an indication of what psychosocial skill? a. Frustration with adults b. Rejection of parents c. Assertion of control d. Stubborn behavior Correct Answer-c. Assertion of control Negativity is a normal behavior in toddlers. The nurse must be aware that this behavior is an important sign of the child's progress from dependency to autonomy and independence. Nurse is doing preconception counseling with a woman who is planning a pregnancy. Which statement suggests that the patient understands the connection between alcohol consumption and fetal alcohol syndrome? a. Beer is not really hard alcohol, so I guess I can drink some b. I understand that a glass of wine with dinner is healthy c. If I drink, my baby may be harmed before I know I am pregnant d. Drinking with meals reduces the effects of alcohol Correct Answer-c. If I drink, my baby may be harmed before I know I am pregnantAlcohol has the greatest teratogenic effect during organogenesis in the first weeks of pregnancy. Therefore, women considering a pregnancy should not drink any alcoholic beverages. A nurse prepares for Denver Screening II of a 3yo child in the clinic when the mother asks the nurse to explain the purpose of the test. What is the nurse's best response about the purpose of the Denver Screening II? a. It measures a child's intelligence b. It helps to determine problems c. It assesses a child's development d. It evaluates psychological responses Correct Answer-c. It assesses a child's development The Denver Development Test II is a screening test to assess children from birth through 6 years of age in the personal/social, fine motor adaptive, language and gross motor development. During this test a child experiences the fun of play. This screening test determines the highest level of functioning in these areas at the time of the examination. Fetal movement count during the third trimester should be at least 5 movements per day. True or false Correct Answer-False In the third trimester, an awake healthy fetus should move at least 3 times per hour. If the baby does not move, the mother should drink a glass of juice and then start a new count. The fourth stage of labor is placental separation and expulsion. True or false Correct Answer-False The third stage of labor is placental separation and expulsion and lasts about 5 to 30 minutes. The fourth stage of labor is maternal adaptation, occurring 1 to 2 hours after birth. When the fetus is active, its heart rate should increase by about 15 beats per minute.True or false Correct Answer-True When the fetus is active, its heart rate will accelerate by about 15 beats per minute above the baseline. Average fetal heart rate is about 130 ppm when near term. Most pregnancy tests measure the level of estrogen in the woman's blood. True or false Correct Answer-False Pregnancy tests measure the hormone human chorionic gonadotropin (hcG) in the urine or in the blood. Levels can be first detected about 12 to 14 days after conception and peak in the first 8 to 11 weeks of pregnancy. One if the first signs of pregnancy is Chadwick's sign, which is the softening of the cervix. True or false Correct Answer-False There are several findings of pregnancy during the first trimester, increased vascularity in the vagina is called the Chadwick's sign; the increased vascularization and softness of the uterine isthmus is Hegar's sign; and the softening of the cervix is Goodall's sign. The nurse will give Rh immune globulin (RhoGAM) to a Rh negative women after a miscarriage (spontaneous abortion). True or false Correct Answer-True RhoGam is administered to Rh negative women after any possible exposure to fetal blood such as after each ectopic pregnancy, miscarriage, abortion or amniocentesis, RhoGAM will be given to help prevent problems associated with incompatible blood types in future pregnancies. Chloasma is the first milk the new mother produces.True or false Correct Answer-False Chloasma is a skin discoloration of pregnancy. The first breast milk is called colostrum. Colostrum is low in fat, high in carbohydrates, protein and antibodies and is easy for the newborn to digest. The fetus receives more oxygenated blood when the laboring mother lies on her side. True or false Correct Answer-True Positioning the laboring mother on her (left) side usually results in a higher fetal oxygen saturation. Other measures to increase fetal oxygenation (and placental perfusion) include administering oxygen to the laboring woman. A gravida 3, para 3 woman should be rushed to the delivery room once engagement has occurred. True or false Correct Answer-False Engagement means that the baby's head no longer floats freely, but has dropped down into the pelvis. In the multipara, engagement normally occurs about 2 weeks before birth. An APGAR score of 2 for appearance means the newborn's fingers and toes are blush in color. True or false Correct Answer-False The normal color all over the newborn is pink; a pink baby earns a score of 2. A baby who is pink with pale blue toes/feet and fingers/hands will receive a score 1 on the APGAR test. A baby tapped briskly on the bridge of the nose will close both eyes.True or false Correct Answer-True Tapping on the glabella (flat bone between the eyebrows) causes a neurologically healthy baby to close both eyes. This is referred to as the glabellar reflex. About 5 days after delivery, loch is pink-brown in color. True or false Correct Answer-True Normal bleeding and discharge should be more watery and pink-brown colored (lochia serosa) about 3 to 5 days after delivery. It may take up to 2 to 4 weeks for discharge to taper off completely. Common issues on the first postpartum day include afterpains and episiotomy discomfort and swelling. True or false Correct Answer-True The nurse should provide information about prevention that will help the new mother cope with common physical and emotional changes she is experiencing. For example, the patient can apply ice or a cold pack to the perineum and use a gentle squeeze of warm water for cleaning after voiding. A woman cannot become pregnant when she is breastfeeding. True or false Correct Answer-False Pregnancy can occur with unprotected intercourse at or become the first menstrual cycle after birth. Nurses should caution women to avoid pregnancy for the first three months after delivery to allow the body time to heal. The safest time for the fetus is to give the mother analgesia when her cervix is dilated 8 to 10 centimeters.True or false Correct Answer-False The safest time to offer analgesia is when dilation is between 4 to 7 centimeters. Which statement is the correct stage of cognitive development for Piaget's: Infant - Sensorimotor stage a. Concepts are attached to concrete situations b. Analyzes situations and uses abstract logic and reasoning c. Uses sucking, grasping, listening, and looking to earn about the environment d. Uses magical thinking and imagination Correct Answer-c. Uses sucking, grasping, listening, and looking to earn about the environment Which statement is the correct stage of cognitive development for Piaget's: Early Childhood - Preoperational stage a. Concepts are attached to concrete situations b. Analyzes situations and uses abstract logic and reasoning c. Uses sucking, grasping, listening, and looking to earn about the environment d. Uses magical thinking and imagination Correct Answer-d. Uses magical thinking and imagination Which statement is the correct stage of cognitive development for Piaget's: School-age concrete operations stage a. Concepts are attached to concrete situations b. Analyzes situations and uses abstract logic and reasoning c. Uses sucking, grasping, listening, and looking to earn about the environment d. Uses magical thinking and imagination Correct Answer-a. Concepts are attached to concrete situationsWhich statement is the correct stage of cognitive development for Piaget's: Adolescence-formal operations stage a. Concepts are attached to concrete situations b. Analyzes situations and uses abstract logic and reasoning c. Uses sucking, grasping, listening, and looking to earn about the environment d. Uses magical thinking and imagination Correct Answer-b. Analyzes situations and uses abstract logic and reasoning When you examine the mouth, you see the soft palate is moist and pink with whitish spots Abnormal or expected findings Correct Answer-Abnormal The soft palate should be reddish pink; white spots are a sign of possible infection The patient is able to stand on one foot, with eyes shut, for five seconds. Abnormal or expected findings Correct Answer-Expected Balancing on one foot, with eyes shut is one sign of normal cerebellar function. A 42 yo breathes 30 times per minute. Abnormal or expected findings Correct Answer-Abnormal Normal respiratory rate in adolescents and adults is 12-20 breaths per minute. During a female patient's breast exam, you see a cluster of very tiny dimples near one nipple.Abnormal or expected findings Correct Answer-Abnormal There should be no dimples, in fact "orange peel" skin is a late sign of breast cancer Auscultation reveals bowel sounds in 2 of the 4 abdominal quadrants. Abnormal or expected findings Correct Answer-Abnormal findings Normally, you should hear bowel sounds in all 4 quadrants in a healthy patient. A 60 yo male has a left scrotal sac that is lightly lower than the right. Abnormal or expected findings Correct Answer-Expected Asymmetry in the scrotum is normal, with the left usually larger or having lower than the right. A patient can tell you her name, but does not know the day of the week week. Abnormal or expected findings Correct Answer-Abnormal Normal mental function includes orientation to person, place, and time. A 5 month old has a sunken anterior fontanel Abnormal or expected findings Correct Answer-Abnormal The fontanel should be flat; a sunken fontanel indicates possible dehydration. An 88 yo has decreased muscle strength in his bilateral upper extremities.Abnormal or expected findings Correct Answer-Expected A common age-associated change with musculoskeletal system is the decline in muscle mass and strength. The adolescent's spine is straight and posterior ribs are symmetrical when the patient bends forward. Abnormal or expected findings Correct Answer-Expected The adolescent patient should be assessed for scoliosis by asking the patient to bend forward and touch his or her toes. The patient's spine should be straight and without curvature or asymmetry. The nurse-patient relationship is mutually defined, social relationship. True or false Correct Answer-False Although it is mutually defined, the nurse-patient relationship is time-limited, goal-directed and bounded by standards of care and of professional practice. It is not a local relationship. In fact, one of the blocks to therapeutic communication is the social response. Only young patients suffer from abuse True or false Correct Answer-False Abuse can affect patients across the lifespan. Children to older adults. Abuse can be physical, emotional, or sexual. Depending on the jurisdiction, nurses may be mandated to report elder abuse. All US states have enacted laws and policies related to child abuse and neglect. Domestic abuse is not mandatory to report unless there is a threat to a child or unborn fetus.The grieving process lasts for approximately one year. True or false Correct Answer-False The time span of the grieving process varies and there is not set time limit for how long an individual grieves. Also, the stages of grieving are not linear. They may pass and later return. Primitive defense mechanisms are very effective for long-term use. True or false Correct Answer-False People use defense mechanisms to protect themselves from things they don't want to think about or deal with. Primitive defense mechanisms, such as denial, regression, acting out and projection, are often used by children and can have short-term advantages, but become less effective when used long term. Stress activates the parasympathetic nervous system True or False Correct Answer-False Stress activates the sympathetic nervous system (norepinephrine and epinephrine) and the endocrine system (especially the pituitary gland). The sympathetic nervous system is responsible for stimulating the "fight-or-flight" response often associated with stress. The process under which the body confronts stress is the General Adaptation Syndrome. Liquid medications are best for patients who are on suicide precautions True or false Correct Answer-True Although the nurse can inspect the client's mouth after giving oral medications in tablet form, medications given in oral liquid form can prevent the client from hiding and hoarding medications.Mental health disorders and substance use disorder rarely occurs together. True or false Correct Answer-False Mental health problems can often lead to alcohol or drug use and abuse. Many clients who suffer from substance use disorder are also diagnosed with mental health disorders (and vice versa). Mental and substance use disorders share some underlying causes, including changes in brain composition, genetics and early exposure to stress and trauma. The nurse should write everything down for a patient with Wernicke's aphasia True or false Correct Answer-False Patients with Wernicke's aphasia may have no understanding of language in any modality, whether spoken or written. They can speak, by what they say makes no sense. Communication may be more effective using non-verbal techniques, such as actions, movements, props, and gestures. Nurses must be aware of their own cultural values and beliefs to avoid biases when providing care to clients. True or false Correct Answer-True Nurses must be aware of and sensitive to the cultural needs and beliefs of their clients and their families, as well as themselves. Nurses must engage in self-awareness and critical reflection of their own beliefs to provide culturally sensitive care to all clients. This is especially true when caring for clients with mental health disorders because biases can hinder the therapeutic relationship. Religious beliefs influence decisions about health. True or false Correct Answer-TrueReligious beliefs impact all aspects of a client's life, including health and illness. Research supports that worship and prayer contribute to positive emotions, including hope and spiritual contentment. The only FDA-approved type of medication to treat this disorder are SSRIs Correct Answer-PTSD Sertraline and paroxetine are FDA-approved to treat PTSD. Other medications may be used for off-label or as adjunct treatment. For example, prazosin may be used to decrease migraines. Electroconvulsive therapy (ECT) is used to treat a severe form of this disorder Correct Answer-Severe depression ECT can be used to as a treatment for severe depression when medication does not ease the symptoms of clinical depression. ECT is not a cure for depression. ECT can also be sued to treat patients with symptoms of delusions, hallucinations or suicidal thoughts. Russell's sign can be observed with this disorder Correct Answer-Bulimia nervosa A person who repeatedly self-induces vomiting will have scraped or raw areas on the knuckles. Bulimia nervosa is a type of eating disorder that involves binging (eating large amounts of food) and purging (vomiting). A client with this disorder may experience drastic changes in mood accompanied by extreme changes in energy, activity, sleep and behavior. Correct Answer-Bipolar disorder Patients with bipolar disorder may experience mood swings ranging from mania to depression, with periods of normal mood and activity in between. Sometimes the mood swings can be unusually intense or extreme; at other times, they are less extreme. "Drug holidays" are sometimes used in the management of this disorder. Correct Answer-ADHD A drug holiday refers to the deliberate interruption of pharmacotherapy for a defined period and for a specific clinical purpose. Sometimes a clinician will give a child with attention deficit hyperactivity disorder (ADHD) a "vacation" from medications on weekends or during summer break from school.A client with this disorder recognizes their behavior is excessive and unreasonable but cannot stop the behavior. Correct Answer-OCD Clients with obsessive compulsive disorder (OCD) cannot control their obsessions and/or compulsions, even though they recognize that they are unreasonable or excessive. A client with this disorder experiences hallucinations and delusional thoughts. Correct AnswerSchizophrenia A client with schizophrenia experiences hallucinations and delusional thoughts. There are different types of schizophrenia, but often the client is unable to think rationally, communicate properly, make decisions or remember information. Malabsorption syndrome and Wernicke-Korsakoff syndrome are associated with this disorder. Correct Answer-Chronic Alcoholism Nutritional deficiencies are common among clients who suffer from chronic alcohol abuse and are related to malabsorption of fat, nitrogen, sodium, water, thiamine, folic acid and vitamin B12. WernickeKorsakoff syndrome (also called Wernicke encephalopathy) is caused by a lack of thiamine (vitamin B1). This disorder includes Alzheimer's disease, traumatic brain injury and Huntington's disease. Correct Answer-Neurocognitive disorders This group of disorders was formerly referred to as "dementia, delirium, amnestic and other cognitive disorders." The child with this disorder has difficulties with social interaction and verbal and nonverbal communication and also exhibits repetitive behaviors. Correct Answer-Autism spectrum disorder A child with autism spectrum disorder (ASD) has difficulty with social interactions and verbal and nonverbal communication; the child also exhibits repetitive behaviors. ASD is considered a neurodevelopmental disorder.Lithium levels and overdose symptoms Correct Answer-0.8-1.2 nausea vomiting diarrhea drowsiness muscle weakness tremor lack of coordination blurred vision tinnitus A 12 yo child is admitted with a fracture of the arm and is told that surgery is required. A nurse finds the child crying and unwilling to talk. What is the most appropriate approach by the nurse? a. Give the child privacy b. Try to distract the child with hand-held electronic game c. Tell the child that the surgery will have no problems d. Make arrangements for the friends to visit as soon as possible Correct Answer-a. Give the child privacy A 12 year-old child needs the opportunity to express any emotions privately. A nurse should facilitate privacy in whatever manner possible. An 8 yo child is admitted to the children's inpatient mental health unit. After the mother's departure, the patient cries and refuses to eat dinner. Which of the following nursing actions is most appropriate? a. Explain that the parent will be upset if the child does not cooperate b. Remind the child of the expectation to eat some or all of the dinnerc. Offer to play with the child d. Tell the child that privileges will be denied for uncooperative behavior Correct Answer-c. Offer to play with the child Play can be used as a distraction and it also facilitates the development of a safe relationship. Play also helps children express their feelings more easily (through toys instead of words.) Setting limits is necessary, but this can be done later. Children must learn responsibility for their own behavior; it is not therapeutic to say their behavior will upset their parents. Parents bring their special needs child to a community health center one day after an explosion occurred at the child's high school. It is determined that the child may be in a crisis state. Which of these interventions is appropriate to implement at this time? a. Discuss of variety of alternative approaches with the child b. Ask the parent to identify the major issues c. Make the child identify a specific problem d. Examine a variety of options with the patient Correct Answer-b. Ask the parent to identify the major issues If a client is unable to participate in problem solving because of developmental delays or altered mental status, then crisis intervention should not be attempted with the client. However, the family can be approached with the use of crisis intervention methods. The crisis intervention method includes five steps: identify the problem and then the alternatives, selection of an alternative, implementation, and evaluation of the outcome. A client who is thought to be homeless is brought to the emergency department (ED) by the police. The client is unkempt, has difficulty concentrating, is unable to sit still, and speaks in a loud tone of voice. Which of these actions is the appropriate nursing intervention for the client at this time? a. Allow the client to randomly move about the holding area until a hospital room is available b. Isolate the client in a secure room until control is regained by the client c. Engage the client in an activity that requires focus and individual effort d. Locate a room that features minimal stimulation during the admission process Correct Answer-d. Locate a room that features minimal stimulation during the admission processTo be placed in a room with minimal stimulation allows the client with moderate anxiety or agitation to have human contact in an environment that does not exacerbate the condition. It also facilitates efficiency in the initial screening and admission process to the ED. By preventing behavioral escalation, this approach promotes safety for the client and staff. The nurse assesses the use of coping mechanisms by an adolescent one week after the client had a motor vehicle accident resulting in multiple serious injuries. Which of these characteristics are most likely to be observed by the nurse? a. Identification, assimilation, withdrawal b. Intellectualization, rationalization, repression c. Ambivalence, dependence, demanding d. Denial, projection, regression Correct Answer-d. Denial, projection, regression Helplessness and hopelessness may contribute to regressive, dependent behavior, which often occurs at any age with hospitalization. Denial or minimization of the seriousness of the illness is used to avoid facing the worst situation. Recall that denial is the initial step in the process of working through any loss. The nurse is assisting a client with substance use disorder (SUD) to deal with issues of guilt. Which response by the nurse would be best for this client? a. "You've caused a great deal of pain to your family and close friends. It will take time to undo all the things you've done." b. "What have you done that you feel most guilty about? What steps can you begin to take to help you lessen this guilt?" c. "Don't focus on the guilty feelings. These feelings will only lead to drinking and taking drugs." d. "Addiction usually causes people to feel guilty. Don't worry, it is a typical response due to your drinking behavior." Correct Answer-b. "What have you done that you feel most guilty about? What steps can you begin to take to help you lessen this guilt?" The correct response encourages the client to get in touch with his/her feelings and to utilize problemsolving steps to reduce guilt feelings; this is the only option that focuses on the client's actions. The other options are statements about general thoughts, with less focus on the client. Also note that threeof the options are statements; if you have no idea about the correct answer, select the odd option (the question) During an interview of a new admission, the nurse notices that the client is shifting positions, wringing the hands, and avoiding eye contact. It is important for the nurse to take which of these approaches? a. Ask the patient what the patient is feeling at this moment b. Refocus the discussion on a less anxiety-provoking topic c. Assess the patient for auditory hallucinations d. Recognize the behavior as a side effect of medication Correct Answer-a. Ask the patient what the patient is feeling at this moment An initial step in anxiety intervention is using the senses to observe, identify, and assess anxiety behaviors. The nurse then should seek client validation of the accuracy of observations and interpretations. The nurse should avoid drawing conclusions based on limited data. In the situation above, the client may simply need to use the restroom but be reluctant to communicate this elimination need! A client tells the nurse, "I have something very important to tell you if you promise not to tell." The nurse should respond with which statement? a. That depends on what you tell me b. I must document and report any information c. I can't make such a promise d. I must report everything to the treatment team Correct Answer-c. I can't make such a promise Secrets, inappropriate in therapeutic relationships, are counterproductive to the therapeutic efforts of the interdisciplinary team. Secrets may be related to risk for harm to self or others on the unit. The nurse should honor and help clients to understand the rights, limitations and boundaries regarding confidentiality and professional relationships A client of Hispanic heritage refuses emergency unit treatment until a curandero is called. What should the nurse understand about the practices of a curanderos?a. Herbal preparations will be used b. Uses holistic healing practices c. Offers spiritual advising d. Witchcraft Correct Answer-b. Uses holistic healing practices A curandero is a folk healer (or shaman) who uses a holistic approach that includes herbs, aromas and rituals, to treat the ills of the body, mind and spirit. Many times, the curandero works with traditional Western health care providers to restore health. A nurse is talking with a client. The client abruptly says to the nurse, "The moon is full. Astronauts walk on the moon. Walking is a good health habit." The client's remarks most likely indicate which finding? a. word salad b. neologisms c. loose associations d. flight of ideas Correct Answer-c. loose associations Though the client's statements are not typical of logical communication, the second and third remark contain elements of the preceding sentence (moon, walk). Neologisms refers to making up words that have personal meaning to the client. Flight of ideas defines nearly continuous flow of speech, jumping from one unconnected topic to another. Word salad refers to stringing together real words into nonsense "sentences" that have no meaning for the listener. The client reports seeing spiders crawling on the walls, over the bed, and on the food tray, but denies feeling spiders crawling on the skin. The nurse determines that there are no spiders in the room. Which of the following assessments should the nurse use to document these findings? (Select all that apply.)a. spiders are not found in room b. incoherent speech c. visual hallucinations d. spiders reported to be crawling on patient e. delusional thinking f. tactile hallucinations g. spiders reported to be crawling on surfaces Correct Answer-a. spiders are not found in room c. visual hallucinations g. spiders reported to be crawling on surfaces Charting should be factual and not judgmental. It is important to evaluate the client's statements. The nurse looks to see if there are indeed spiders in the room surfaces. When the client sees something that is not present, this is called a visual hallucination. Because this client did not feel crawling spiders, tactile hallucinations is not an acceptable answer. A client with a diagnosis of depression has recently been acting suicidal and is now more social and energetic than usual. Smiling, the client tells a nurse, "I've made some decisions about my life." What should be the nurse's initial response? a. "Are you thinking about killing yourself?" b. "You need to discuss your decisions with your therapist." c. "You've made some decisions. You seem happier now. " d. "I'm so glad to hear that you've made some decisions." Correct Answer-a. "Are you thinking about killing yourself?" Sudden mood elevation and energy may signal a higher risk of suicide. The nurse must validate suicidal ideation as a beginning step in evaluating degree of the risk. A more direct approach is used because a threat to harm exists in the client.At the geriatric day care program, a client who has been diagnosed with a neurocognitive disorder is crying and repeatedly saying: "I want to go home. Call my daddy to come for me." The nurse should take which action? a. Give the client simple information about what the client will be doing that day b. Direct the client firmly to the assigned group activity c. Tell the client you will call someone to come get the client and suggest the client to join an exercise group while waiting d. Inform the client that the client must wait until the program ends at 5:00 pm to leave Correct Answerc. Tell the client you will call someone to come get the client and suggest the client to join an exercise group while waiting Comfort and distraction are key approaches in validation therapy. They are the kindest and most effective actions for clients who have varying degrees of a neurocognitive disorder (formerly referred to as dementia.) The distressed, disoriented client should be gently oriented to reduce fear and increase the sense of safety and security. However, reorientation is often ineffective when the client is upset. Environmental changes provoke stress and fear, especially in clients diagnosed with any degree of Alzheimer's disease. A client who is a victim of domestic violence tells the batterer: "I need a little time away." How would the nurse expect that the batterer might respond? a. With a new commitment and an opportunity to seek counseling b. With fear of rejection, resulting in increased rage toward the client c. With relief, welcoming the separation as a means to have more personal time d. With acceptance, perceiving the comment as an indication that the relationship is in trouble Correct Answer-b. With fear of rejection, resulting in increased rage toward the client Those that batter others commonly react to such statements or actions with fear of rejection, abandonment and loss. These types of actions by the recipient of the battering only serve to increase the batterer's rage at the partner. A nurse is to present information about Chinese folk medicine to a group of student nurses. Based on this cultural belief system, the nurse would explain that illness is attributed to which focus?a. The use of improper hot foods, herbs and plants b. A failure to keep the physiological processes of life in balance with nature and others c. Yin, the negative force that represents darkness, cold and emptiness d. Yang, the positive force that represents light, warmth and fullness Correct Answer-b. A failure to keep the physiological processes of life in balance with nature and others Chinese folk medicine proposes that health is regulated by the opposing forces of yin and yang. Under normal conditions, there is a dynamic equilibrium of these two physiological processes. Yin is the negative force characterized by darkness, cold and emptiness. Excessive yin predisposes one to nervousness. Yang is the positive force that represents light, warmth and fullness. Illness occurs when the balance between yin and yang is broken. A Native-American chief visits his newborn son and performs a traditional ceremony that involves feathers and chanting. The charge nurse tells a colleague, "I wonder if he has any idea how ridiculous he looks - he's a grown man!" This statement is an example of which non-therapeutic approach? a. Prejudice b. Ethnocentrism c. Stereotyping d. Discrimination Correct Answer-a. Prejudice In this question, the nurse is reacting to the chief's behavior, which is an example of prejudice. Prejudice reflects the overall attitude and emotional response (both positive and negative, conscious and nonconscious) to a group. Discrimination refers to differences in actions towards different groups on the basis of prejudice. Stereotypes are cognitions or beliefs used to categorize others and systemize information in order to better predict behavior and react. Stereotypes can be used to develop prejudices toward others and to discriminate.Ethnocentrism is the practice of making judgments about other cultures based on the values and beliefs of one's own culture (especially related to language, customs and religion.) A postpartum Hispanic client refuses hospital food because it is "cold." What action should the nurse take initially? a. Have UAP reheat the food if the patient wishes b. Schedule the dietician to meet with patient c. Encourage the patient to eat for healing and strength d. Ask the patient what foods are acceptable or unacceptable Correct Answer-d. Ask the patient what foods are acceptable or unacceptable Many Hispanic clients subscribe to the rebalancing of "hot" and "cold" in the postpartum period. After giving birth, when a woman has lost blood, she is considered to be in a cold state; therefore, she needs to restore her humoral balance. What defines "cold" and "hot" can best be explained by the client and this needs to be incorporated into the plan of care. Note that the correct response allows for client feedback; this is the only client-centered option. A client diagnosed with a terminal condition is admitted to the nursing unit. What should be the initial action taken by the nurse? a. Ensure that the patient is free from pain, nausea, or dyspnea b. Refer the patient's family to the chaplain c. Discuss the options for Advanced directives with the patient and family d. collaborate with the multidisciplinary team members Correct Answer-a. Ensure that the patient is free from pain, nausea, or dyspnea Keep in mind the nursing process where the client is the center of attention. Also, recall that physiological needs are priority to psychosocial needs. Thus, the client should be kept as comfortable as possible. After the physiological needs are met, any of the other choices would be appropriate with the discussion of the advanced directives being first. This would not be the initial action because a "discussion" may take some time and the client needs would be ignored during any discussion.Behaviors of alcohol and drug abuse have outcomes of impaired judgment and increased risk-taking behavior. What nursing diagnosis best applies to this data? a. Risk for knowledge deficit b. Risk for injury c. Altered thought process d. Disturbance in self-esteem Correct Answer-b. Risk for injury Accidents increase as a result of intoxication of substances. Studies indicate alcohol is a factor in more than 50% of motor vehicle fatalities, in 53% of all deaths from accidental falls, in 64% of fatal fires, and in more than 80% of suicides. A nurse in the emergency department suspects domestic violence as the cause of a client's injuries. What action should the nurse take first? a. Refer the patient to a victim advocate b. Interview the patient privately c. Photograph the specific injuries and include with documentation d. Ask the client if there are any old injuries Correct Answer-b. Interview the patient privately It is critical to separate the client from anyone who came in with the client, whether it be a partner or friend, and interview the client in privacy. With the use of the nursing process, the nurse's first action when a client is unstable or has potential problems is further assessment of the situation. The correct answer is the one most focused on gathering more information. During the private intake assessment the nurse would possibly institute the other actions in the remaining options. Protein is the body's only source of nitrogen True or false Correct Answer-TrueIn a healthy did, a nitrogen balance is achieved when dietary intake is balanced by excretion of urea wastes. A negative nitrogen balance occurs if excretion is greater than the nitrogen content of the diet, as seen in burns, infections, injuries, fever or starvation. Women who are planning on becoming parents need about 200 ug daily of folic acid. True or false Correct Answer-False Prior to conception and during early pregnancy, women need to add 400 ug of folic acid (vitamin B9) each day. Research has demonstrated that this significantly decreases the risk of neural tube defects. Less than 4 to 8 wet diapers may be a sign of dehydration in a baby. True or false Correct Answer-True Babies should have a minimum of 4 to 8 wet diapers daily. Babies can become quickly dehydrated. Other signs of dehydration in infants include sunken fontanel, decrease or absence of tears, dry mouth and irritability. Glucose is the only fuel used by brain cells. True or false Correct Answer-True Although most energy needs could be met by fats and proteins, the brain requires carbohydrates, specifically glucose. Neurons need a constant supply of glucose since they cannot store it. Patients with insomnia either have difficulty falling asleep or staying asleep. True or false Correct Answer-True Insomnia is a sleep disorder. There are 2 types of insomnia: primary and secondary.The patient using a cane should hold it on his strong side and move the can at the same time as the weaker leg. True or false Correct Answer-True A cane can provide stability when walking. The standard cane is fine if it's only needed for balance but if the patient needs the cane to bear weight, an offset can with four tips might be best. Iron is one of the macro minerals fond in a healthy human body. True or false Correct Answer-Iron is considered a trace mineral. The seven major minerals in the body are calcium, magnesium, sodium, potassium, phosphorus, sulfur, and chlorine. Complementary and integrated health therapies replace the need for pharmacologic interventions. True or false Correct Answer-False Complementary and integrated health therapies are widely used among patients for various disorders and are often used in conjunction with medial treatment. Pain management may consist of pain medication, as well as relaxation or acupuncture. Complementary and integrated health therapies may also be effective at reducing anxiety, improving mood and increasing a patient's sense of control over the environment. The thirst center is located in the parathyroid center. True or false Correct Answer-False A dry mouth and dehydration will activate the thirst center, which is located in the hypothalamus. As a result, there will be a conscious desire to drink. There will also be a series of subconscious steps to correct the dehydration, including vasopressin secretion by the pituitary gland.A patient with gout is prescribed a pureed diet. True or false Correct Answer-False Patients with gout should eat a low-purine diet because purines are turned into uric acid, which aggravates the symptoms of gout. Almost any food contains purines: organ meats, anchovies and sardines in oil, mushrooms, spinach, dried beans and peans contain higher levels. The pureed diet is indicated when chewing or swallowing is difficult or causes discomfort. The nurse will hold the tube feeding when the gastric residual is greater than 100-150mL True or false Correct Answer-False If the residual volume exceeds the amount of formula given in the previous 2 hours, it may be necessary to consider reducing the rate of feeding. Current protocols state not to stop feedings unless there are other signs of intolerance, such as bloating abdominal pain, emesis, or nausea. Urinary incontinence is a normal part of aging. True or false Correct Answer-False Urinary incontinence is not normal, regardless of the patient's age. Kegal exercises, medications (anticholinergics, topical estrogen), medical devices (pessary), or surgery (sling procedures, bladder neck suppression) can help to counteract incontinence. A 7yo child can be taught to self-catherize him or herself. True or false Correct Answer-TrueChildren with neurogenic bladder complications or spina bifida may successfully learn self-catherization as young as 6 or 7 yo. Training initially starts with performing the procedure using a doll. The patient with a sigmoid colectomy will have semi-liquid stool collect in a colostomy bag. True or false Correct Answer-False A colectomy is the primary treatment for colon cancer. The cancerous part of the large intestine is removed and remaining bowel is joined together (anastomosis). The patient will not need a colostomy. Bowel managements may be more frequent after a colectomy. Neuropathic pain is also called musculoskeletal pain. True or false Correct Answer-False Somatic pain is also known as musculoskeletal pain because it originates in the tissues such as the skin, muscle, joints, bones, and ligaments. Neuropathic pain originates from the nervous system. The mother of a 3 month old infant tells the nurse. "I want to change from formula to whole milk and add cereal and meats to my infant's diet." What should be emphasized as the nurse teaches about nutrition. a. Fluoridated tap water should be used to dilute milk b. Solid foods should be introduced at 3 to 4 months c. Whole milk is difficult for infants to digest d. Supplemental apple juice can be used between feedings. Correct Answer-c. Whole milk is difficult for infants to digest Cow's milk is not given to infants younger than a year old because the tough, hard curd that develops in the digestive tract is difficult to digest. In addition, it contains little iron and creates a high renal solute load.If infants drink milk with a minimal introduction to solid food they will have the tendency to develop anemia. The nurse is caring for a patient who had a sigmoid colostomy and requests assistance with removing flatus from one-piece drainable ostomy pouch. Which should be the course intervention by the nurse? a. Pull the adhesive seal around the pouch to allow flatus to escape b. Pierce the plastic of the ostomy pouch with a pin to vent the flatus. c. Assist the patient to ambulate to reduce the flatus in the pouch. d. Open the bottom of the pouch to allow the flatus to be expelled. Correct Answer-d. Open the bottom of the pouch to allow the flatus to be expelled. The only correct way to prevent flatus from a one-piece drainable ostomy pouch is to instruct the patient to obtain privacy because the release of the flatus will cause odor. The patient should open the bottom of the pouch, allow the flatus to escape, and then close the bottom of the pouch. Parents are concerned that their 11yo child is a very picky eater. The nurse suggests which of these approaches be the best initial action? a. Provide fruit, vegetables, and protein snacks b. Encourage the child to keep a daily log of foods eaten c. Discuss the consequence of an unbalanced diet with the child d. Consider a liquid supplement to increase calories Correct Answer-c. Discuss the consequence of an unbalanced diet with the child A priority is to educate the preadolescent as to appropriate diet, and the outcomes that result if the diet is not adequate. Afterwards the other options are appropriate to implement The nurse is assisting patients diagnosed with trigeminal neuralgia (tic douloureux) to meet their nutritional needs. Which approach should the nurse recommend? a. Encourage the patient to eat fish, liver, and chicken.b. Offer small meals consisting of high calories, soft foods. c. Provide additional servings of fruits and raw vegetables d. Assist the patient to sit in a chair for meals. Correct Answer-b. Offer small meals consisting of high calories, soft foods. If the patient is losing too much weight because of poor appetite due to pain in the jaw, the nurse needs to teach about foods that are high in calories and nutrients as well as food that require less chewing. The nurse should also suggest frequent, small meals that are eaten every two hours instead of 3 large meals daily. The patient needs assistance to insert bilateral in-the-ear hearing aids. What action should the nurse take before inserting hearing aids? a. Identify the hearing aid programmed for each ear. b. Adjust the volume control to its highest setting c. Clean the hearing aid with plain soap and water d. Grasp the open battery door to use as a handle Correct Answer-a. Identify the hearing aid programmed for each ear. Since hearing aids are customized for each ear, the nurse should make sure that the correct hearing aid is inserted in the correct ear (a red dot indicates the right ear). The volume should be turned down when inserting the devices and adjusted after they are in the ear. Hearing aids should only be cleaned with soft cloth; water or alcohol can damage the device. The battery door should never be used as a handle. The nurse is making a home visit to a patient diagnosed with COPD. The patient tells the nurse that he used to be able to walk from the house to the mailbox without difficulty. Now, he has to pause to catch his breath halfway through the trip. Which nursing diagnosis is appropriate for the patient based on this assessment? a. Impaired mobility related to COPD as evidenced by a change b. Activity intolerance related to chronic tissue hypoxia as evidenced by fatigue c. Self-care deficit related to dyspnea as evidenced by fatigued. Ineffective airway clearance related to increased bronchial secretions as evidenced by complaints Correct Answer-b. Activity intolerance related to chronic tissue hypoxia as evidenced by fatigue Activity intolerance describes a condition in which the patient's physiological capacity for activities is compromised. The other nursing diagnoses are not supported with data from the situation. The nurse is caring for a patient in labor. Which non-pharmacologic measures can the nurse implement to provide the laboring patient with a sense of control and comfort? Select all that apply a. Childbirth education b. Amnioinfusion c. Intrauterine pressure catheter d. Aromatherapy e. Coujnterpressure f. Lamaze breathing techniques Correct Answer-a. Childbirth education d. Aromatherapy e. Coujnterpressure f. Lamaze breathing techniques Nonpharmacologic labor pain management techniques incorporate special attention to all the senses. Aromatherapy - smell Relaxing music - auditory Coujnterpressure, massage, effleurage - tactile Childbirth education helps to prepare the patient and support person to understand what to anticipate prior to, during, and after L&D, giving the patient a sense of control, initiation of breathing techniques to close the gate to nerve stimulation caused by pain is also used.Intrauterine pressure catheter, which provides an exact measurement of contractions and amnioinfusion, which involves the infusion of fluid into the uterus during labor, are unrelated to pain management. A patient is diagnosed with gastroesophageal reflux disease (GERD). The nurse's instruction to the patient about the approaches to dietary changes should include which topic? a. Decrease intake of fatty foods b. Focus on 3 average meals daily c. Increase intake of milk products d. Avoid all raw fruits and vegetables Correct Answer-a. Decrease intake of fatty foods GERD may be aggravated by fatty diet. A diet low in fat would decrease the symptoms of GERD. Other agents that should also be decreased or avoided are: cigarette smoking - nicotine caffeine alcohol chocolate narcotic analgesic - meperidine (Demerol) A patient tells the nurse "I'm in a lot of pain. As the nurse collects more information about the patient's pain, what should be the first step in pain assessment? a. Have the patient identify previous methods that relieved the pain b. Ask the patient to rate the pain on a scale of 1 to 10 c. Determine the location of the pain d. Accept the patient's report of pain Correct Answer-d. Accept the patient's report of pain Before anything else, the nurse must simply accept the fact that the patient is experiencing pain - pain is subjective. The nurse would then determine the intensity of pain, quality, location, onset, and pain relief.A nurse is caring for a patient in skeletal traction. Which nursing intervention is appropriate for this patient? a. Maintain correct body alignment b. Use alcohol or iodine-based products to clean around the pins c. Remove the weights when turning the patient d. Maintain a supine position at all times Correct Answer-a. Maintain correct body alignment The best response is to maintain correct body alignment. Skeletal traction is used to maintain proper alignment of the bones while healing. A pin or wire is inserted through the bone and weights are applied, using a system of ropes and pulleys attached to the bed frame to provide a constant pulling pressure - weights should not be removed or lived. Iodine-based solutions or alcohol should not be used for pin care because they can corrode the pins and/or stain the skin. Skeletal traction allows the patient to change position without interfering with the pull of traction, by the head of the bed must be completely lowered several times a day to prevent hip flexion contractures. A 78yo reports having difficulty moving his bowels. What information is most important for the nurse to obtain during the assessment process? a. Trends in weight gain or loss b. Health history and patient's diet c. Elimination patterns over the past week d. Lab reports, including a CBC with differential Correct Answer-b. Health history and patient's diet The nurse should obtain the patient's health history, noting risk factors, comorbid conditions, and medications. The nurse should assess for patient's diet, including fiber intake. The nurse can then ask the patient to clarify what he means when he reports having difficulty moving his bowels (and determine if there are any misconception about bowel habits). Assessing the patient's health history and diet should uncover any eating or swallowing difficulties that could contribute to weight loss. During a 12-hour shift a patient who underwent a transurethral resection of the prostrate (TURP), had an IV intake of 1200 mL, oral intake of 400 mL, continuous bladder irrigation of 2400 mL, 2 syringe flushes of 50mL each and indwelling urinary catheter output of about 3000 mL.What is the end of shift fluid intake Correct Answer-4100 A nurse is performing nutritional assessment on a 2yo child. Which of these principles should the nurse apply? a. Serving size at this age is about 2 tablespoons b. Increased serum albumin or pre albumin levels indicate malnutrition c. An accurate measurement of intake is not reliable d. Total intake varies greatly every day Correct Answer-a. Serving size at this age is about 2 tablespoons In children, a greater guide to serving sizes is one tablespoon of solid food per year of age. Understanding this, the nurse can access adequacy of intake for any child. During a home visit, the nurse observes the mother of a school-aged child in a long leg synthetic cast using a cloth covered wooden spoon handle to relieve itching inside the cast. Which response by the nurse is most appropriate? a. Suggest placing an ice pack (protected by plastic) over the area that is itching b. Instruct them to blow hot air from a hand-held hair dryer into the cast c. Remind the mother and child that itching is normal d. No response is needed because the mother's behavior is appropriate Correct Answer-a. Suggest placing an ice pack (protected by plastic) over the area that is itching Because itching is a common and frustrating problem for a person with a cast, it would not be therapeutic to simply remind the mother and child that itching is normal. But using anything to scratch the skin inside the cast is not recommended because it can injury the skin and increase risk for infection. Patents can use a hair dryer on cool setting. Cool temperatures can constrict blood vessels, minimizing itching (just like heat vasodilates to intensify itching). A patient is admitted with a diagnosis of renal caliculi. The patient reports oral temperature is 100.8 F. Which of these goals is the priority nursing focus for this patient?a. Control nausea b. Prevent infection c. Manage pain d. Maintain fluid balance Correct Answer-c. Manage pain An immediate goal of therapy is to alleviate pain, which can be quite severe. The nurse discusses nutrition with a pregnant woman who is iron-deficient and follows a vegetarian diet. The selection of which foods indicates the woman has learned food sources of iron? a. Cereal and dried fruits b. Fish and dairy products c. Carrots and other yellow-orange vegetables d. Whole grains and yellow vegetables Correct Answer-a. Cereal and dried fruits Cereals are often fortified with vitamins and iron. Fruits rich in iron include: apricots currants raisins dates figs prunes Other sources for iron: dark, leafy green vegetables beanslentils chick peas soybeans Following a major burn to the lower extremities, a diet high in protein and carbohydrates is ordered for a 7yo child. What reason would the nurse give the family that would help explain these dietary requirements? a. Stimulate peristalsis for enhanced absorption of nutrients b. Spare protein catabolism to meet the child's metabolic needs c. Provide a well-balanced and nutritionally complete diet d. Strengthen the immune system to prevent infection Correct Answer-b. Spare protein catabolism to meet the child's metabolic needs Child's energy and protein requirement will be high due to catabolism of trauma, heat loss, and the demands of tissue regeneration. Good nutrition is important for wound healing and helps reduce the risk of infection, but a child who has been burned needs about 2 to 3 times more calories and proteins to help him/her heal and grow. A patient is admitted to the rehab unit after having had a CVA with residual mild dysphagia. The appropriate intervention for this patient is which action? a. Place the patient in an upright position while eating b. Tilt the head back while eating to facilitate the swallowing reflex c. Offer finger foods such as crackers or pretzels d. Initially place patient on clear liquids Correct Answer-a. Place the patient in an upright position while eating An upright position facilitates proper chewing and swallowing. Liquid diet is contraindicated with patients with swallowing difficulties.The nurse is reinforcing teaching with a patient about compromised host precautions. The patient is receiving filgrastrim (Neupogen) for neutropenia. Which lunch selection suggests that the patient has learned abut the necessary dietary changes? a. BBQ beef, baked beans, and coleslaw from the deli b. Roast beef, mashed potatoes, sautéed green beans c. Peanut butter sandwiches, apple, cold-brewed iced tea d. Chicken sandwiches made with sprouts and farmer's cheese, skim milk Correct Answer-b. Roast beef, mashed potatoes, sautéed green beans Food should be cooked or canned. Avoid raw fruits and vegetables, undercooked meat and eggs, soft "moldy" cheeses, lunch meat, and salads from the deli. Should only consume pasteurized dairy products and fruit juices and avoid cold-brewed teas and drinks. A nurse is caring for a patient diagnosed with an unstable spinal cord injury at the T7 level. Which intervention should take priority during the planning of care? a. Increase caloric intake to aid healing b. Place the patient on a pressure-reducing support surface c. Increase fluid intake to prevent dehydration d. Use skin care products designed for use with incontinence Correct Answer-b. Place the patient on a pressure-reducing support surface Patient is at the greatest risk for skin breakdown due to immobility and decreased sensation below the level of injury. The initial approach should be the selection and placement of the patient on the best support surface for the relief of pressure, shear, and friction forces. The client receives furosemide 40 mg by mouth daily. The pharmacy stocks furosemide 20 mg tablets. How many tablets does the nurse administer for a 40 mg dose? Correct Answer-2 tabletsOrder: Acetaminophen elixir 100 mg by mouth every 4 hours as needed for pain. Available concentration of acetaminophen is 80 mg/0.8 mL. How much acetaminophen elixir will the nurse administer? Correct Answer-1 mL The client receives 300 mg phenytoin by mouth daily for seizures and the pharmacy sent phenytoin 125 mg/5 mL suspension. How many mL of suspension will the nurse administer? Correct Answer-12 mL/day The child weighs 68.2 pounds. The nurse must administer amoxicillin by mouth at 30 mg/kg/day in divided doses every 6 hours. How much amoxicillin does the nurse administer each day? How many milligrams of amoxicillin does the nurse administer for each dose? Correct Answer-233 mg of amoxicillin for each dose The nurse prepares vancomycin 500 mg IV in 250 mL of normal saline to infuse over 2 hours. What is the administration rate in mL/minute? Correct Answer-2 mL/min for 2 hours The prescription is linezolid 600 mg IV in 300 mL of D5W to infuse over 2 hours. The IV tubing drip rate is 10 gtts/mL. What drip rate should the nurse use? Correct Answer-the drip rate is 25 gtts/minute The client receives epinephrine 0.25 mcg/min IV via infusion pump. The pharmacy sends epinephrine 0.1 mg in 250 mL of normal saline. What rate in mL/hr will the nurse use to program the infusion pump? Correct Answer-37.5 mL/hour The nurse applies mild pressure to the inner canthus of the eye after instilling eye drop medication. True or False Correct Answer-True Applying pressure to the inner aspect of the eye for about a minute or so helps decrease systemic absorption of the medication. Sublingual medications avoid the first-pass effect. True or False Correct Answer-TrueMedications given sublingually and rectally bypass metabolism by gastrointestinal and hepatic enzymes. When a medication is given orally, the amount of available medication is reduced before it reaches the general circulation due to the first-pass effect. Examples of Schedule I medications include morphine and secobarbital. True or False Correct Answer-False Schedule I drugs have no medical use and there is a high potential for abuse. Examples of Schedule I drugs include heroin and LSD. While morphine and short-acting barbiturates like secobarbital also have a high risk for abuse, they also have safe and accepted uses; they are examples of Schedule II drugs. A nurse should ask a client with emphysema to bear down during the insertion of a non-tunneled central venous catheter (CVC). True or False Correct Answer-True Intravenous pressure must exceed atmospheric pressure during CVC insertion to prevent air from entering the catheter and traveling to the heart and lungs. Any client, regardless of his or her diagnosis, should be asked to bear down during CVC insertion. An elderly client is more sensitive to the active substance in a transdermal patch than a younger adult. True or False Correct Answer-True Transdermal medication application requires adequate tissue perfusion to absorb and distribute the medication. Skin permeability varies based on hydration, temperature, age (the skin of babies and the elderly is more permeable than that of other age groups) and ethnicity (the skin of Caucasians is more permeable than that of African Americans). Therefore an older client would be more sensitive to medication administered this way than a younger adult. Lactated Ringer's (LR) solution is a hypotonic fluid.True or False Correct Answer-False Lactated Ringer's is an isotonic fluid solution used in many different clinical situations, including fluid resuscitation. An example of a hypotonic fluid is 0.45% sodium chloride. Clients increase their risk of adverse effects if they use herbal supplements along with prescription medications. True or False Correct Answer-True There is an inherent risk of adverse effects when a client combines herbal agents with prescription drugs. Because herbal remedies have drug actions of their own, the client taking prescription drugs should not take herbal supplements or over-the-counter drugs until they have discussed these with their health care providers. The nurse can crush the oral medication disopyramide CR and mix it with applesauce. True or False Correct Answer-False CR means 'controlled release' and this medication must not be crushed. Do not crush any oral medication that ends in the following abbreviations: CR (controlled release), CD (controlled delivery), LA (long acting), SR (sustained release), XL (extended release), XR (extended release) or XT (extended release). Hypovolemia is a risk for the client receiving whole blood products. True or False Correct Answer-False Hypervolemia (circulatory or fluid overload) develops when too large a volume of blood is given too quickly. To avoid hypervolemia, blood products should be infused at a rate no faster than 2 to 4 mL/kg/hour (but not to exceed a 4 hour hang time).The nurse can use the deltoid muscle, vastus lateralis muscle, ventrogluteal muscle and dorsogluteal muscle to administer an intramuscular injection. True or False Correct Answer-False The accepted sites for intramuscular injections include the deltoid muscle, vastus lateralis muscle and ventrogluteal muscle. The dorsogluteal muscle should not be used for IM injections due to the risk of sciatic nerve damage. The triage nurse identifies that a 16 yo patient is legally married ad has signed the consent form for treatment. What should be an appropriate action by the nurse? a. Withhold treatment until telephone consent can be obtained from the parter b. Proceed with the triage process in the same manner as any adult patient c. Refer the teenager to a community pediatric hospital emergency department d. Ask the teenager to wait until a parent or legal guardian can be contacted Correct Answer-b. Proceed with the triage process in the same manner as any adult patient Minors can become known as an emancipated minor through marriage, pregnancy, high school graduation, independent living, or service in the military. Therefore, this married patient has the legal capacity of an adult. Otherwise the page for legal signature is 18 years of age. A nurse is assigned to care for four clients. After listening to change-of-shift report, how would the nurse prioritize care for the following clients? (Drag the responses into the correct order.) a. The postop patient who has an order to be discharged home b. Patient with tracheostomy c. Patient with colonoscopy d. Patient in skeletal traction Correct Answer-b. Patient with tracheostomy c. Patient with colonoscopy d. Patient in skeletal traction a. The postop patient who has an order to be discharged homeThe nurse will check on the client with a tracheostomy (airway) first. The nurse would then check on the client who is to undergo a procedure (to ensure the prep was completed and the results of the bowel movements are clear). Next, the nurse would check on the client in skeletal traction, and finally the nurse would prepare the client who is ready for discharge. A client who is unconscious is brought to the emergency department by an ambulance. What document should be given priority to guide the approach for the care of this client? a. Orders written by the health care provider in an emergency department b. A notarized original of the Advanced Directive brought in by the partner c. National statement of patient rights and the patient self-determination act d. Clinical pathway protocol of the agency and the emergency department Correct Answer-b. A notarized original of the advance directive brought in by the partner This document specifies the client's wishes of what actions are to be taken when the client becomes unable to make health care decisions. The advance directive often includes a living will and the power of attorney to whom will make the decisions for the client. The next document that would take precedent are the orders written by the heath care provider. The clinical pathways are used to evaluate the client's progress during therapy. The nurse manager is interviewing a prospective employee who just completed the agency application. Which approach should the nurse manager use to assess skills competencies of this potential employee? a. "Let's review your skills checklist for type and level of skill for tasks." b. "Let's talk about your comfort zone for working independently." c. "What degree of supervision for basic care do you think you need?" d. "What types of complex client-care tasks or assignments do you prefer?" Correct Answer-a. "Let's review your skills checklist for type and level of skill for tasks." The nurse needs to know that the potential employee has competence in certain tasks that are common on the unit. One way to do this is to do mutual review of the agency list of skills. The other questions might be asked during the skills checklist review.A client asks the nurse for information about a living will. Which statement made by the client demonstrates an understanding of a living will? (Select all that apply.) a. "It lists all my assets and how they should be divided among my family after I die." b. "I will need to identify someone to be my health care proxy." c. "My wishes for end of life treatment are stated in writing." d. "I should sit down and discuss my wishes for end of life care with my loved ones." e. "A living will is a legal document that becomes a permanent part of my health care record." f. "A living will must be renewed by a designated family member each time I am hospitalized." Correct Answer-b. "I will need to identify someone to be my health care proxy." c. "My wishes for end of life treatment are stated in writing." d. "I should sit down and discuss my wishes for end of life care with my loved ones." e. "A living will is a legal document that becomes a permanent part of my health care record." An advance health care directive is also known as a living will. It is a legal document in which a person specifies his or her wishes concerning medical treatments at the end of life, when s/he is unable to make those decisions. Advance care planning involves sharing personal values and wishes with loved ones and selecting someone, (called a medical power of attorney or health care proxy) who will eventually make medical decisions on the client's behalf. A living will does not expire; it remains in effect unless it is changed. A living will does not include information regarding assets or a person's estate. The registered nurse (RN) and the unlicensed assistive person (UAP) are caring for clients on a surgical unit. Which action(s) by the UAP warrant immediate intervention? (Select all that apply.) a. The UAP assists a client, who had a total knee replacement two days ago, to shave using a straightedge razor b. The UAP assists a client, who received an IV narcotic analgesic 30 minutes ago, to ambulate in the hall c. The UAP applies moisture barrier cream to the client's excoriated perianal area d. The UAP empties the indwelling catheter bag for the client who had a transurethral resection of the prostate (TURP) yesterdaye. The UAP applies a fingertip pulse oximeter on a client's finger with dark blue nail polish Correct Answer-a. The UAP assists a client, who had a total knee replacement two days ago, to shave using a straight-edge razor b. The UAP assists a client, who received an IV narcotic analgesic 30 minutes ago, to ambulate in the hall e. The UAP applies a fingertip pulse oximeter on a client's finger with dark blue nail polish The UAP can perform a number of nursing tasks, such as emptying an indwelling urinary catheter bag and applying moisture barrier cream after peri care. However, it is unsafe for the UAP to ambulate a client who recently received an IV push narcotic. Although UAP can shave clients, it is unsafe to shave someone using a straight-edge razor because a client who had knee replacement surgery is probably taking an anticoagulant; only an electric razor should be used. Pulse oximeter readings must be done on a finger that is warm and free from dark fingernail polish. The nurse is assessing a client who is two days post-surgery and notes new and sudden onset of confusion. There is an order to discharge the client to go home today. What would be the best action for the nurse to take? a. Teach a family member clean dressing change technique and address safety measures in the home b. Collaborate with the health care provider about the change of condition c. Make a clinic appointment with the primary health provider for follow-up care the next day d. Collaborate with the dietitian for increasing protein and calcium in the diet Correct Answer-b. Collaborate with the health care provider about the change of condition Although all the responses may be correct for a post-surgical client, a status change involving confusion must be reported, particularly if it is a new finding. As an advocate for the client, the nurse should protect the client from physical harm and collaborate with the health care provider about a change in the plan for discharge. The charge nurse sends a certified nursing assistant (CNA) to help a registered nurse (RN) with the admission of a client with multiple health problems. Which of the following tasks would be appropriate for the the CNA to perform with the nurse during the admission process? (Select all that apply.) 15of123 Ref # 4435The charge nurse sends a certified nursing assistant (CNA) to help a registered nurse (RN) with the admission of a client with multiple health problems. Which of the following tasks would be appropriate for the the CNA to perform with the nurse during the admission process? (Select all that apply.) a. Collect a urine specimen b. Obtain routine vital signs (temperature, pulse, respirations, blood pressure) c. Assist the client to change into a gown d. Orient the client to the room e. Observe and document the client's ability to walk to the bathroom Correct Answer-a. Collect a urine specimen b. Obtain routine vital signs (temperature, pulse, respirations, blood pressure) c. Assist the client to change into a gown d. Orient the client to the room CNAs can obtain routine vital signs, measure height and weight, and obtain urine specimens. CNAs also routinely help clients with activities of daily living (ADLs). Although nursing assistants can measure vital signs, it's up to the RN to determine how to use this data when developing the plan of care. The CNA cannot assess clients or perform any of the other steps of the nursing process. Any nursing intervention that requires independent, specialized nursing knowledge, skill or judgment must be performed by a nurse. After working with a client, an unlicensed assistive personnel (UAP) tells the nurse, "I have had it with that demanding client. I just can't do anything that pleases him. I'm not going in there again." The nurse should respond with which statement? a. "He may be scared and taking it out on you. Let's talk to figure out what to do next." b. "I will talk with him and try to figure out what to do or what the problem is." c. "Ignore him and get the rest of your work done. Someone else can care for him the rest of the day." d. "He has a lot of problems. You need to have patience with him." Correct Answer-a. "He may be scared and taking it out on you. Let's talk to figure out what to do next." This response explains the client's behavior without belittling the UAP's feelings. The UAP is encouraged to contribute to the plan of care to help solve the problem. The other responses are incorrect becausethey either belittle the UAP or ignore the problem and do not include the UAP in planning of how to deal with the issue. The 86 year-old client will be participating in a transitional care program after discharge from the hospital. What is the primary purpose of a transitional care program? a. Increase client understanding of discharge instructions b. Reduce insurance costs c. Increase satisfaction with nursing care d. Reduce readmissions to the hospital Correct Answer-d. Reduce readmissions to the hospital Older adults who complete a transitional care program after being discharged from the hospital are much less likely to be readmitted to the hospital. The Affordable Care Act mandates that each facility have a "quality assurance and performance improvement program", designed to help reduce unnecessary hospital readmissions. The nurse is named in a lawsuit. Which of these factors will offer the best protection for the nurse in a court of law? a. Clinical specialty certification by an accredited organization b. Above-average performance reviews prepared by nurse manager c. Complete and accurate documentation of assessments and interventions d. Sworn statement that health care provider orders were followed Correct Answer-c. Complete and accurate documentation of assessments and interventions The medical record is a legal document. Documentation should include all steps of the nursing process; it must be complete, accurate, concise and in chronological order. Inaccurate or incomplete documentation will raise red flags and may indicate the nurse failed to meet the standards of care. The attorney will review the medical record with the nurse before giving a deposition (sworn pretrial testimony.) Above-average performance reviews could be considered supporting information. Certification is an "extra" based on the nurse's initiative; it is, however, unrelated to accurate charting.A nurse manager suspects a staff nurse of substance use disorder (SUD). Which approach would be the best initial action by the nurse manager? a. Confront the nurse about the suspicions in a private meeting b. Counsel the employee to resign to avoid investigation and rumors c. Consult with human resources personnel about the issue and needed actions d. Schedule a staff conference, without the nurse present, to collect information Correct Answer-c. Consult with human resources personnel about the issue and needed actions The nurse manager needs to consult with human resources to determine the proper procedures for documenting and reporting the nurse's behavior. The nurse manager could also consult the EAP if one is available. If the staff nurse is also suspected of diversion, and a written policy exists, the nurse manager would follow these procedures. Attempts should be made to help the nurse with SUD by providing counseling and treatment for this disease. The nurse has just listened to the change of shift report on an orthopedic unit. Which of the following clients should the nurse check first? a. A 20 year-old in skeletal traction for two weeks since a motorcycle accident b. A 75 year-old who is in skin traction of the left leg prior to a scheduled fractured hip repair surgery c. A 16 year-old who had an open reduction of a fractured wrist 10 hours ago d. A 72 year-old who returned from a right hip replacement surgery two hours ago Correct Answer-d. A 72 year-old who returned from a right hip replacement surgery two hours ago The nurse should compare clients to screen for one who has the most imminent risks and acute vulnerability for being unstable. The client who returned from surgery two hours ago is at risk for hemorrhage because the hip and femur are considered vascular areas and should be checked first. The 16 year-old is within the initial 24 hours post-op period and should be seen next. The 75 year-old is potentially vulnerable to age-related physical and cognitive impairments from being on bedrest and having a large bone fracture. The client who can safely be visited last is the 20 year-old who is two weeks post-injury. A nurse has been assigned to four clients in the emergency department, with each client experiencing one of these conditions. Which client should the nurse check first?a. Viral pneumonia with atelectasis b. Spontaneous pneumothorax with a respiratory rate of 38 c. Acute asthma with episodes of bronchospasm d. Tension pneumothorax with slight tracheal deviation to the right Correct Answer-d. Tension pneumothorax with slight tracheal deviation to the right Tracheal deviation indicates a significant volume of air being trapped in the chest cavity with a mediastinal shift. In tension pneumothorax the tracheal deviation is away from the affected side. The affected side is the side where the air leak is in the lung. This situation also results in sudden air hunger, agitation, hypotension, pain in the affected side, and cyanosis with a high risk of cardiac tamponade and cardiac arrest. An elderly client is admitted to a home care agency following hospitalization for exacerbation of heart failure. The client lives alone, has difficulty completing activities of daily living (ADLs), and is unable to drive. List the order of the steps in the case management process by dragging and dropping the options below. a. Reassessment of health status and ADL ability b. Assessment of biophysical and sociocultural considerations c. Evaluation of progress towards client's goals d. Referral to personal care attendant and transportation services e. Identification of nursing diagnoses Correct Answer-Assessment of biophysical and sociocultural considerations Identification of nursing diagnoses Referral to personal care attendant and transportation services Reassessment of health status and ADL ability Evaluation of progress towards client's goals Case management is a collaborative process that assesses, plans, implements, coordinates, monitors, and evaluates options and services to meet an individual's health needs.The new graduate nurse interviews for a position in a nursing department of a large health care agency that uses the approach of shared governance. Which of these statements best illustrates the shared governance model? a. Non-nurse managers supervise nursing staff in groups of units b. An appointed board oversees any administrative decisions c. Staff groups are appointed to discuss nursing practice and client education issues d. Nursing departments share responsibility for client outcomes Correct Answer-d. Nursing departments share responsibility for client outcomes Shared governance or self-governance is a method of organizational design. It promotes empowerment of nurses to give them responsibility for client care issues and outcomes with other divisions in the agency. The nurse, who is caring for a client with complex and unique health needs, describes the nature of the illness in an online social forum for nurses. Neither the client's real name nor any other personal identifiers are used. What, if any, consequence could result from posting this information online? a. here won't be any consequences because the information was posted on a website for nursing professionals b. There won't be any consequences because the client's real name was not used c. The nurse could be reprimanded for not clearing the information first with hospital administration d. The nurse could be fired for breach of confidentiality Correct Answer-d. The nurse could be fired for breach of confidentiality Even though the client was not identified by name, someone could probably figure out who the nurse was writing about. Many health care facilities have adopted a social media policy; it is important to understand that nurses can be fired for posting personal information about clients online, because this is an invasion of privacy. In addition to being a HIPAA violation, the Health Information Technology for Economic and Clinical Health Act (HITECH Act) gives states attorneys the right to pursue violations of patient privacy. The client states to the nurse: "I am ready to stop all of these treatments. I just want to go home and enjoy my family for the little bit of time I have left." Which action is most appropriate?a. Encourage the client to discuss this decision with the health care provider and family b. No action is needed at this time unless the client repeats the statement to another caregiver c. Tell the family members that the client's preference is to go home to die d. Call in a referral to a social worker and explain that the request will need to be discussed in more detail at a later time Correct Answer-a. Encourage the client to discuss this decision with the health care provider and family The client has the right to stop treatment and should be supported in clearly communicating this decision with the health care provider and family. The nurse needs to act as an advocate for the client. It is factually incorrect to wait until the request is repeated; clients should not need to express their wishes repeatedly before caregivers listen to them. The nurse should not be the one to share sensitive information with the family; the client controls that information. Social services may get involved but time is of the essence for those who are terminally ill. A client frequently admitted to the locked psychiatric unit repeatedly compliments and then invites one of the nurses to go out on a date. The nurse should take which of these approaches? a. Discuss the boundaries of a therapeutic relationship with the client b. Inform the client that the hospital policy prohibits staff to date clients c. Ask to not be assigned to this client or request to work on another unit d. Tell the client that such behavior is inappropriate and unethical Correct Answer-a. Discuss the boundaries of a therapeutic relationship with the client The nurse-client relationship is one with professional not social boundaries. Consistent adherence to the limits of the professional relationship builds trust. The client may need to be educated about the interactions in a therapeutic relationship. The nurse is checking on clients in the unit. Which of these findings indicates that an infusion pump set to deliver a morphine drip basal rate of 10 mL per hour, plus PRN dosages for breakthrough pain, is not functioning correctly? a. The client states: "I just can't get relief from my pain."b. The level of the drug is 100 mL at 9 am and is 50 mL at 12 noon c. The level of the drug is 100 mL at 8 am and is 80 mL at 12 noon d. The client complains of discomfort at the IV insertion site Correct Answer-c. The level of the drug is 100 mL at 8 am and is 80 mL at 12 noon The minimal dose is 10 mL per hour, which would mean 40 mL is given in a four-hour period. If any PRN doses were given then less would be in the bag. Minimally, 60 mL should be left at 1200 (12 Noon). The pump is not functioning when more than expected medicine is left in the container. A parent calls the hospital hot line and is connected to the triage nurse. The caller states: "I found my child with odd stuff coming from the mouth and an unmarked bottle nearby." Which of these comments would provide the best information to help the nurse to determine if the child has swallowed a corrosive substance? a. "Ask the child if the mouth is burning or throat pain is present." b. "Has the child had vomiting, diarrhea or stomach cramps?" c. "Take the child's pulse at the wrist and see if the child has trouble breathing lying flat." d. "What color are the child's lips and nails and has the child voided today?" Correct Answer-a. "Ask the child if the mouth is burning or throat pain is present." Local irritation of tissues indicates a corrosive poisoning. The other comments may be helpful in determining the child's overall condition. However, the question concerns evaluation for ingestion of a caustic substance. A client with hepatitis A (HAV) is newly admitted to the unit. Which action would be the priority to include in this client's plan of care within the initial 24 hours? a. Wear masks with shields if there is potential for fluid splash b. Use disposable utensils and plates for meals c. Provide soft easily digested food with frequent snacks d. Wear gown and gloves during client contact Correct Answer-d. Wear gown and gloves during client contactHAV is usually transmitted via the fecal-oral route, or when someone with the virus handles food without washing hands after using the bathroom. The virus can also be contracted by drinking contaminated water, eating raw shellfish from water polluted with sewage or by being in close contact with a person who is infected - even if that person has no findings. In fact, the disease is most contagious before findings ever appear. The nurse should recognize the importance of isolation precautions from the initial contact with the client on admission until the noncontagious convalescence period. The health care team is planning discharge for a 90 year-old client diagnosed with musculoskeletal weakness. Which intervention would be the priority to help prevent falls in the home? a. Begin therapy for muscle strengthening and balance b. Place night lights in the bedroom and bathroom c. Wear eyeglasses and hearing aid d. Take calcium and vitamin D supplements Correct Answer-b. Place night lights in the bedroom and bathroom Family members and the client should understand the simple actions they can take to help prevent falls in the home. More falls occur in the bedroom than in any other location; a simple environmental change would be to add night lights in the bedroom and bathroom. Muscle strengthening and balance exercises, taking calcium and wearing glasses may be all indicated for this client, but using night lights is an immediate and effective action to help prevent falls. The clinic nurse assists the health care provider with physical examinations and the collection of laboratory specimens. Which of these findings does the nurse recognize as being reportable to the public health department? a. Positive eye discharge confirming conjunctivitis b. Clinical findings of impetigo c. Skin scraping confirming the presence of ringworm d. Positive stool culture for shigella Correct Answer-d. Positive stool culture for shigella The Centers for Disease Control and Prevention (CDC) have a list of notifiable infectious diseases that is updated yearly. Shigellosis is the only reportable infection of those listed. Shigella are bacteria that caninfect the digestive tract and cause (painful) diarrhea, cramping, vomiting, nausea; in severe cases it can cause seizures and kidney failure. Ringworm is a contagious fungal infection. Impetigo is a contagious, superficial bacterial skin infection. Conjunctivitis has many causes and is usually diagnosed from signs and symptoms and patient history. Mass casualty survivors are brought to the emergency department (ED) after a disaster. The nurse is assigned to four clients who were triaged in the field and have just arrived in the ED. Which client will the nurse care for first? a. The person with multiple wounds and an open fracture b. The person with hypotension and a sucking chest wound c. The person with head trauma requiring mechanical ventilation d. The person with an undisplaced fracture of the radius Correct Answer-b. The person with hypotension and a sucking chest wound Typically, the tab colors used in triage are black, yellow, green and red. Red-tagged clients have immediate threats to life and require care right away; this would be the survivor with hypotension and a sucking check wound. Yellow-tagged clients have major injuries that need treatment within 30 minutes to 2 hours (the client with the open fracture), and green-tagged client have injuries that can be delayed more than 2 hours (the closed fracture). Black-tagged clients are treated last during a mass casualty situation because there is little chance for survival. The client, who is diagnosed with dementia, wanders throughout the long-term care facility. How can the nurse best ensure the safety of a client who wanders? a. Attach a monitoring band to the client's wrist b. Explain the risk of walking with no purpose c. Frequently reorient the client to time, person, place d. Apply a restraint to keep keep the client in a chair when awake Correct Answer-a. Attach a monitoring band to the client's wrist A wander management system is used to give people with dementia and other "at risk" clients the ability to move freely where they live. The sensor in the bracelet trips an alarm that's attached to exterior doors if the client attempts to leave the facility. It is inappropriate to use restraints or otherrestrictive devices to keep clients in chairs or beds (unless they are potentially harmful to themselves or others.) Reality orientation is inappropriate for someone with dementia. A severely injured client is moved into an examination area of the emergency department. The family member who accompanied the client to the ED is screaming at the nurse, saying that someone better start doing something right away. What is the best response by the nurse? a. "I need you to go to the waiting area. You can come back when you're more in control." b. "I'm going to give you a few minutes alone so you can calm down." c. "I can't think when you are yelling at me. Talk to me in a normal voice." d. "I know you are upset. But please control yourself and sit down. Otherwise I will have to call security." Correct Answer-vd. "I know you are upset. But please control yourself and sit down. Otherwise I will have to call security." Most violent behavior is preceded by warning signs, such as yelling or swearing. The challenge for nurses is to apply interventions that de-escalate a person's response to stressful or traumatic events. The keys to effective limit setting are using commands to express the desired behavior and providing logical and enforceable consequences for noncompliance. Nurses should acknowledge the agitated person's feelings and be empathetic, reminding him or her that they are there to help. A client is scheduled to receive an oral solution of radioactive iodine (131I). What information is the priority for the nurse to include when teaching the client about this treatment? a. "Your family can use the same bathroom as you are using, without any special precautions." b. "Drink plenty of water and empty your bladder often during the initial three days of therapy." c. "In the first 48 hours, you should avoid contact with children and pregnant women; be sure to flush the commode twice after urination or defecation." d. "Use disposable utensils for two days; if you feel nauseous within 12 hours of the first dose, please vomit in the toilet and flush it twice." Correct Answer-c. "In the first 48 hours, you should avoid contact with children and pregnant women; be sure to flush the commode twice after urination or defecation." The client's urine and saliva are radioactive for 24 hours after ingestion, and vomitus is radioactive for six to eight hours. The client should drink 3 to 4 liters of fluid a day for the initial 48 hours to help remove the (131I) from the body. To minimize exposure to radiation, nursing staff should plan to givecare in the shortest time possible (less time equals less exposure), working as far away from the radiation source as possible. Each nurse should also wear a personal film badge or pocket dosimeter. he client is observed falling out of bed when reaching for something on the overbed table. The client then states: "Don't just stand there. I feel fine - help me up." What is the correct order of actions the nurse should take? a. Call the health care provider b. Complete an incident report c. Obtain a complete set of vital signs d. Assist the client back to bed, with help from other staff Correct Answer-c. Obtain a complete set of vital signs d. Assist the client back to bed, with help from other staff a. Call the health care provider b. Complete an incident report The first step is always to assess the client for any obvious injuries and to obtain a complete set of vital signs (especially blood pressure) and neurologic assessments. If the client does not appear to be injured, staff members can assist the client back into bed. The nurse should then call the health care provider to report the incident. Finally, the nurse should complete the incident report. Of course, personal items should be placed close to the client so that s/he can reach them. The nurse listens to report about a newly admitted client who has a skin ulcer that's tested positive for MRSA (methicillin-resistant Staphylococcus aureus). What precautions must be taken for this hospitalized client? (Select all that apply.) a. Keep all equipment in the client's room for his/her sole use Correct! b. Place the client in a single room Correct! c. Wear mask when providing routine care to the client d. Perform hand hygiene after direct contact with the client and before leaving the roomCorrect! e. Keep the door to the room closed, with a notice for visitors Correct Answer-a. Keep all equipment in the client's room for his/her sole use b. Place the client in a single room d. Perform hand hygiene after direct contact with the client and before leaving the room e. Keep the door to the room closed, with a notice for visitors Contact precautions are recommended in acute care settings for MRSA when there's a risk for transmission or wounds that cannot be contained by dressings. The client should be in a single room, with the door closed; the sign on the door instructs visitors to report to the nurse before entering the room. All equipment, such as stethoscopes and blood pressure devices, should be for the client's sole use and kept in the room. Health care workers must perform hand hygiene (wash hands with soap and water) after direct contact with the client and his/her environment and before leaving the isolation room. Contact precautions require health care workers to wear gloves and a gown; a face mask is not necessary for routine care. A client arrives in the emergency department after a radiologic accident at a local factory. After placing the client in a decontamination room, the nurse gives priority to which intervention? a. Ensure physiologic stability of the client b. Double bag the client's contaminated clothing c. Wrap the client in blankets to minimize staff contamination d. Begin decontamination procedures for the client Correct Answer-a. Ensure physiologic stability of the client The nurse must initially assist in the stabilization of a client prior to the performance of any other tasks related to radiologic contamination. A radiation survey meter reading above background radiation levels indicates the possibility of contamination. Radiologic contamination rarely results in loss of consciousness or immediate visible signs of injury. Thus, other causes of injury or illness should be ruled out. The nurse is assessing the uterine fundus of a client who delivered a healthy neonate 10 hours ago. Identify the area where the nurse would expect to feel the fundus. Correct Answer-The uterus should be felt at the level of the umbilicus from about 1 to 24 hours after birth.A community health clinic nurse is assessing a walk-in client who is experiencing lightheadedness. The client has a history of arthritis and takes naproxen (Aleve) and treats high cholesterol with fish oil and garlic. The assessment reveals that the client is pale, blood pressure is 88/40, pulse is 114, respiratory rate is 22, and temperature is 98.2 F (36.7 C). What specifically should the nurse ask this client about? (Select all that apply.) a. Tingling or numbness in the extremities b. Color of bowel movements c. Bruising d. Frequency and amount of naproxen used e. Photophobia Correct Answer-b. Color of bowel movements c. Bruising d. Frequency and amount of naproxen used NSAIDS (Aleve), fish oil, and garlic can all increase the risk for bleeding. The vital signs and pale skin color indicate possible hypovolemia (tachycardia and hypotension) secondary to blood loss. The nurse should inquire about other findings that may indicate bleeding, i.e., black tarry stools, bruising, and should determine the amount of NSAIDs taken daily. The nurse is assessing a 28 year-old female for risk factors contributing to osteoporosis. Which statement reported by the client should alert the nurse that additional teaching about this disease is indicated? (Select all that apply.) a. "I get sun exposure daily and always use sunblock protection." b. "I'm just started following the Mediterranean diet and already feel more energized." c. "I'm a professional dancer and train 8 to 10 hours a day." d. "I consume only skim milk, never whole milk." e. "I take 1000 mg OsCal (calcium carbonate) every morning with breakfast." Correct Answer-c. "I'm a professional dancer and train 8 to 10 hours a day." d. "I consume only skim milk, never whole milk."A nutritional plan that emphasizes fruits and vegetables, low-fat dairy and protein sources, and increased fiber (found in the Mediterranean diet) is beneficial to maintaining bone health and reducing the risk of heart disease. Adequate daily sun exposure is important for vitamin D synthesis, which is important for bone health. Although a calcium supplement is a good idea for this client and calcium carbonate should be taken with food for better absorption, calcium is absorbed more efficiently when it's taken in amounts of 500 to 600 mg at one time. Also, overtraining in women causes decreased estrogen levels and may increase the risk for osteoporosis. The nurse is preparing a speech to a local service organization about clinical trials in cancer care. Which of the following statements would be correct to include? (Select all that apply.) a. Clinical trials have led to improved cancer prevention and treatment b. There is a clinical trial protocol for all types of people with cancer c. A clinical trial is one of the first steps in the research process d. Clinical trials require approval of a human subjects review board Correct Answer-d. Clinical trials require approval of a human subjects review board Clinical trials involve the use and study of treatments on actual human subjects and have been important in making advances in cancer outcomes. After many stages of research have been completed, the clinical trial becomes one of the final steps of the process. Because they involve real people, human subjects review boards must approve the research. There is not a clinical trial for every type of cancer victim, as potential participants in clinical trials must meet specific protocols. A male client admitted with a diagnosis of a spinal cord injury (SCI) at level C-5 asks the nurse how the injury will affect his sexual function. Which statement is the best response? a. "Normal sexual function is not possible." b. "Ejaculation will be normal." c. "Sexual functioning will not be impaired at all." d. "Sexual functioning may be possible." Correct Answer-d. "Sexual functioning may be possible." Even though sexual function is controlled by parts of the central nervous system, sexual function after a SCI will depend on many factors, such as the severity of the injury and even the age of the client. Theclient will need to get to know his body and learn how it reacts in certain situations. The client should also talk to his health care provider for options to achieve an erection. A nurse enters a 2 year-old child's hospital room in order to administer an oral medication. When the nurse asks the child, "Are you ready to take your medicine?" the response is an immediate, "No!" What would be an appropriate next action by the nurse? a. Give the medication to the parent and ask the parent to give it b.Explain to the child that the medicine must be taken now c. Leave the room and return five minutes later and give the medicine d. Mix the medication with ice cream or applesauce Correct Answer-c. Leave the room and return five minutes later and give the medicine Because the nurse gave the child a choice about taking the medication, the nurse must comply with the child's response in order to build or maintain trust. Toddlers do not have an accurate sense of time, so leaving the room and coming back later is another episode to the toddler. Medications should not be mixed with food nor fluids because the amount taken, especially in children, cannot be controlled. Indicate the location of pain that supports the diagnosis of suspected pancreatitis. Correct Answer-Acute pancreatitis produces sharp pain in the epigastric area because of the anatomical position of the pancreas behind the stomach. It is not unusual for a client to report "my stomach hurts" yet be holding the pelvic or periumbilical region. The client may even report upper back pain. Nurses need to clearly assess correct locations regardless of how the client identifies it verbally. A registered nurse (RN) works for a visiting nurse agency (VNA) and makes a home visit to admit a client newly diagnosed with type 1 diabetes. The client has a small foot ulcer that was debrided and needs daily wound care. Which of the following options is the most important intervention to ensure a successful outcome? a. Involve the client in making health care decisions b. Schedule daily RN visits to the client c. Refer to a local diabetes support group d. Arrange for a friend or relative to visit daily Correct Answer-a. Involve the client in making health care decisionsAlthough all interventions may benefit the client, the involvement of the client in making health care decisions improves outcomes. The client is more motivated to adhere to recommendations when involved in the process, setting priorities and making decisions. A nurse is anticipating providing guidance to parents of a toddler about readiness for toilet training. Which statement describes what the nurse should know in order to provide such guidance? a. Neuronal impulses are interrupted at the base of the ganglia b. Myelination of the spinal cord is completed by this age c. The child learns voluntary sphincter control through repetition d. The toddler can understand cause and effect Correct Answer-b. Myelination of the spinal cord is completed by this age Voluntary control of the sphincter muscles can be gradually achieved due to the complete myelination of the spinal cord. The time frame is between the ages of 18 to 24 months of age. If the child has not begun walking without holding on then myelination of sphincters is not complete and toilet training would not be successful. The nurse is assessing a client in the labor and delivery unit. Which of the following actions is correct when using palpation to assess the characteristics and pattern of uterine contractions? a. Place a hand on abdomen below the umbilicus and palpate uterine tone with fingertips b. Evaluate intensity by pressing fingertips into the uterine funds c. Determine frequency by timing the end of one contraction until the end of the next contraction d. Assess uterine contractions every 30 minutes throughout the first stage of labor Correct Answer-b. Evaluate intensity by pressing fingertips into the uterine funds To assess contractions for frequency, duration and intensity, the nurse will place one hand on the uterine fundus and use his or her fingers to feel the changes in the uterus as it contracts. The nurse can determine the frequency of the contractions by noting the time from the beginning of one contraction to the beginning of the next one. To determine the duration of the contraction, the nurse will note the time when tensing of the fundus is first felt (the beginning of one contraction) an [Show More]
Last updated: 1 year ago
Preview 1 out of 466 pages
.png)
Reviews( 0 )
Document information
Connected school, study & course
About the document
Uploaded On
Sep 08, 2022
Number of pages
466
Written in

Additional information
This document has been written for:
Uploaded
Sep 08, 2022
Downloads
0
Views
120

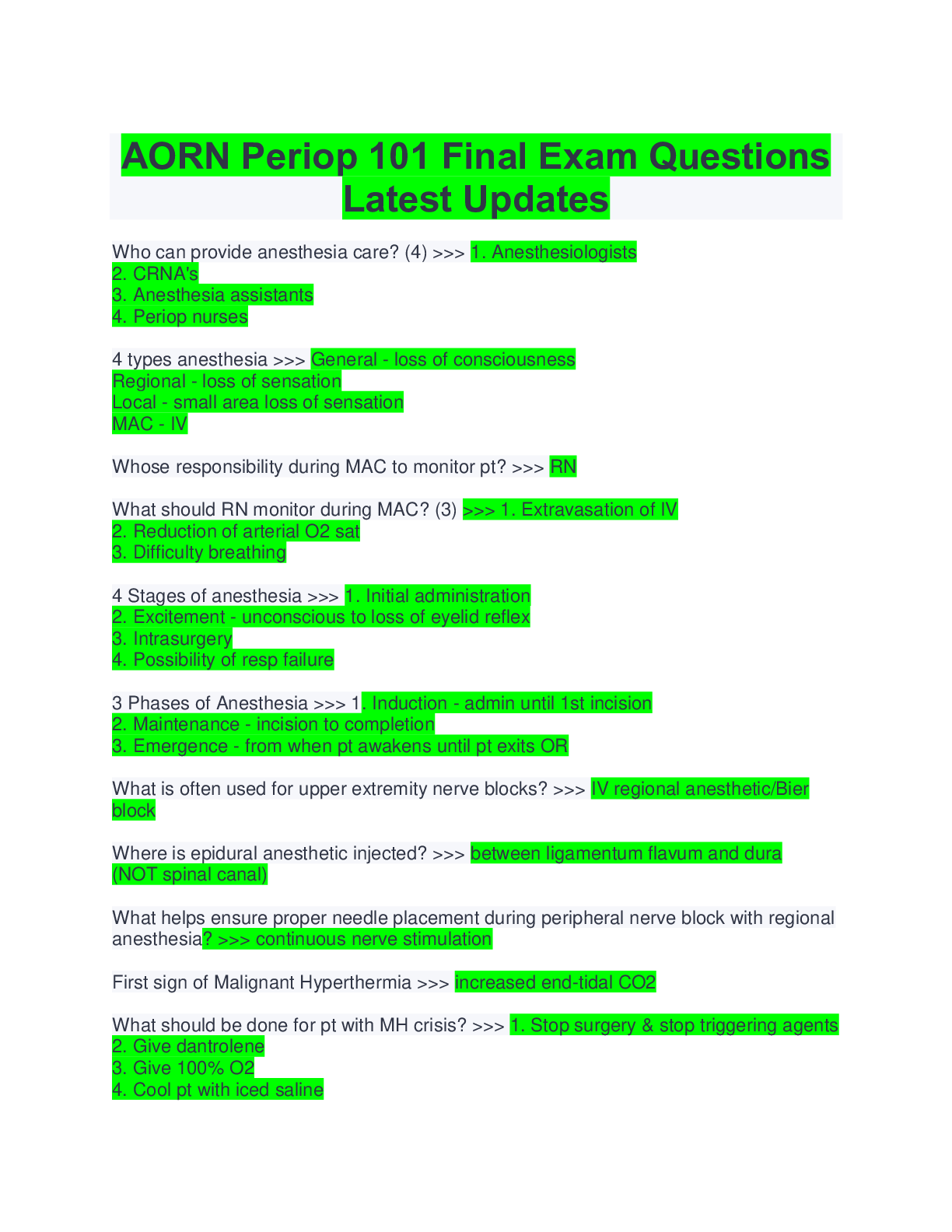
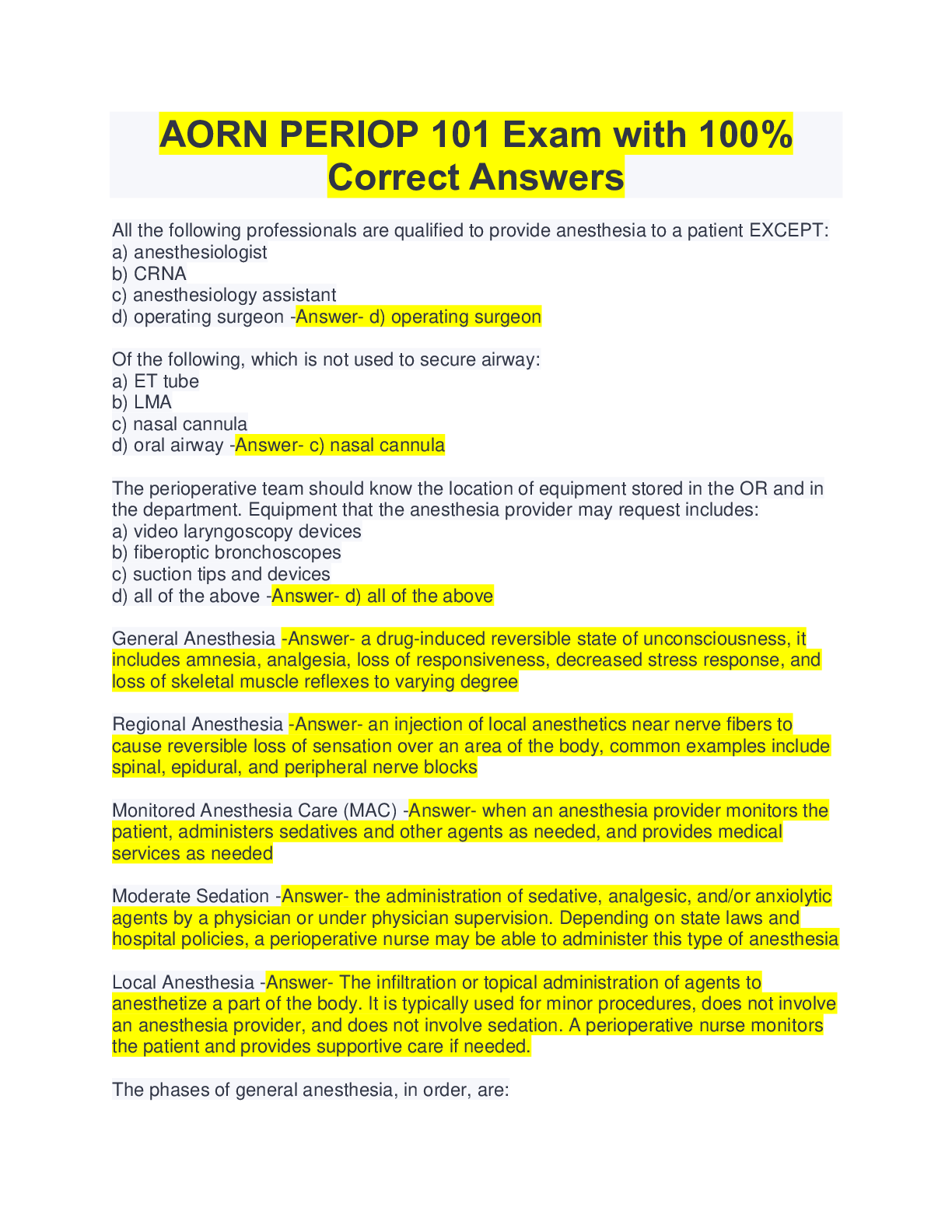
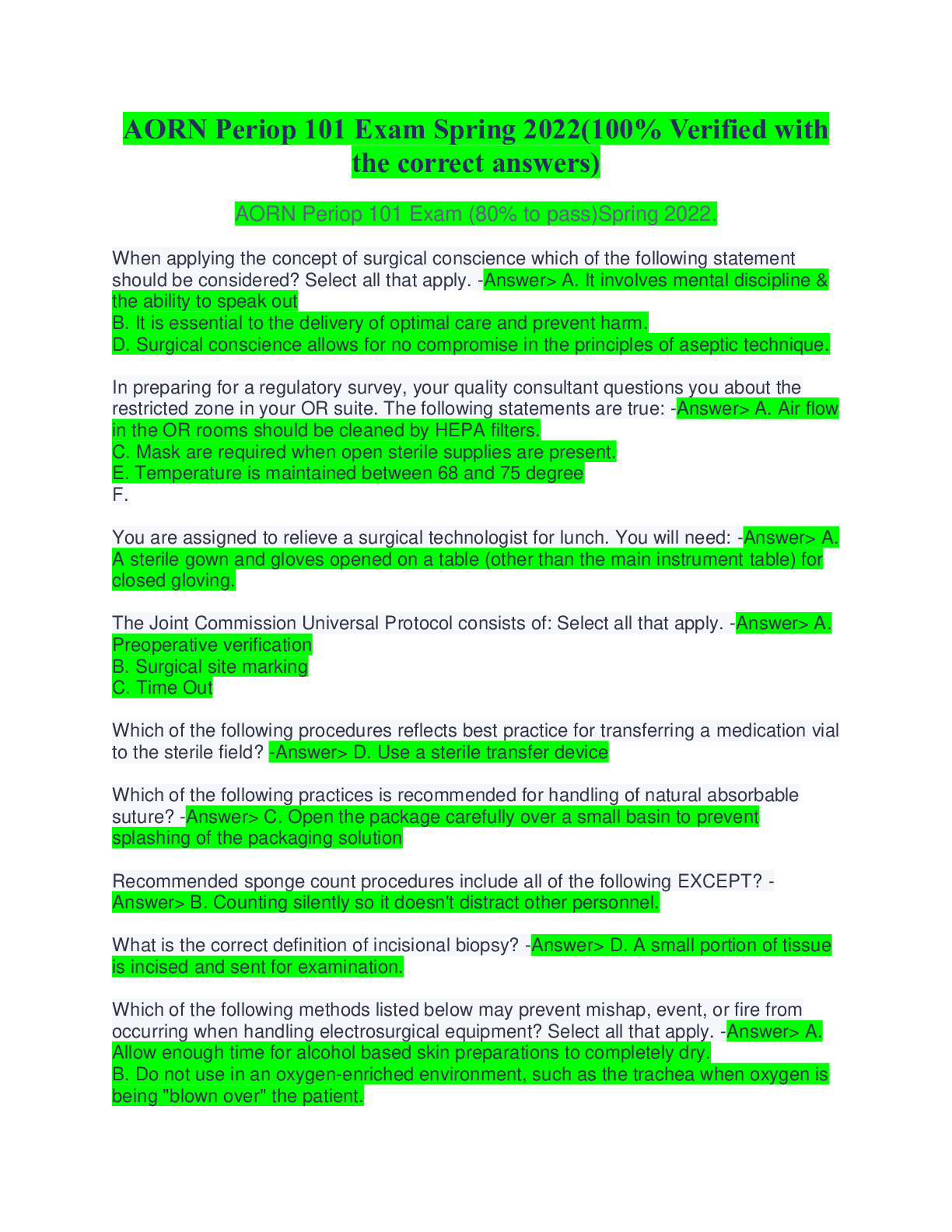
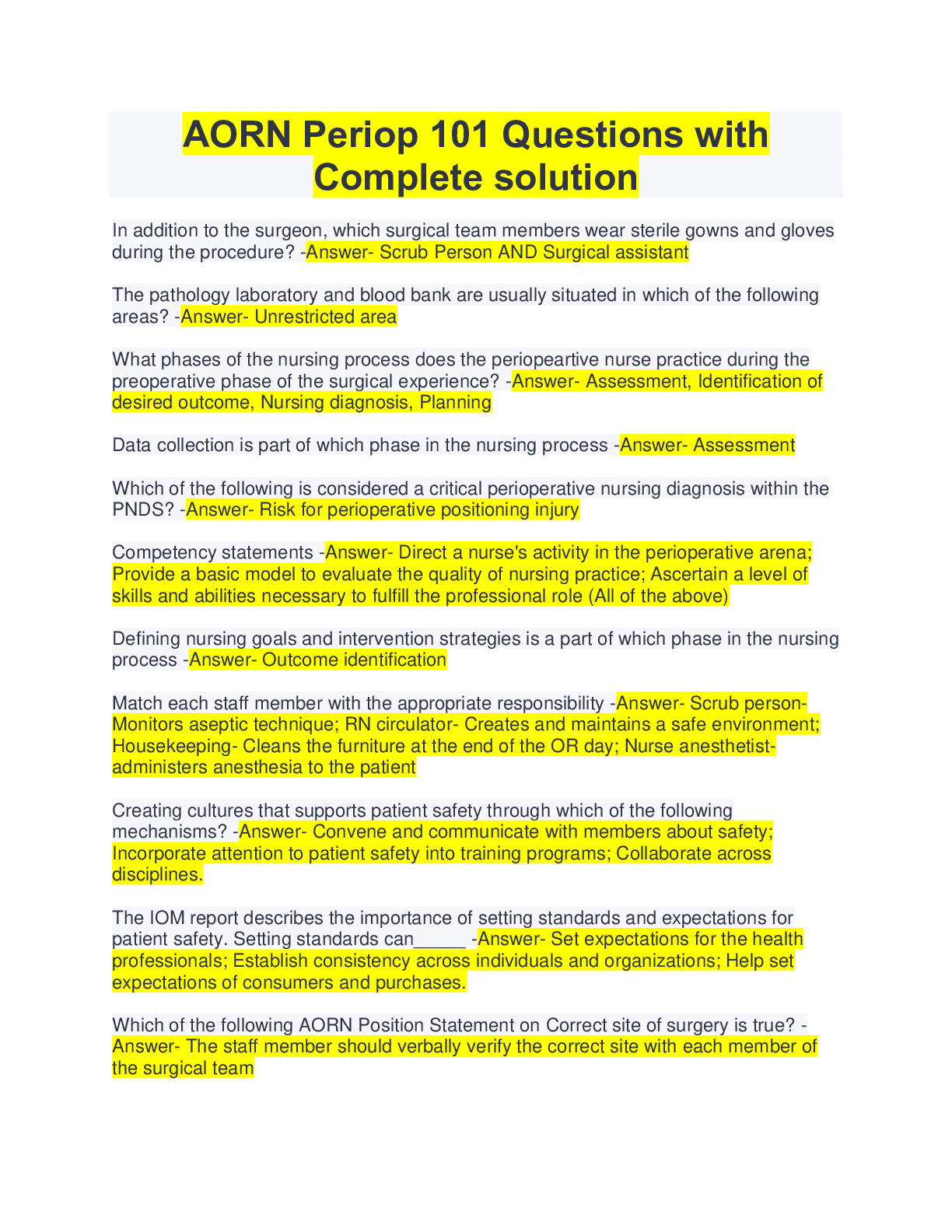
.png)
.png)
.png)
.png)

.png)
.png)
.png)
.png)
.png)
.png)
.png)
